
Abstract
We evaluated Amsterdam HIV Testing Week (HTW) 2016 regarding its primary goals of raising awareness and prompting HIV testing. Participating services offered free, anonymous HIV testing, with a focus on reaching men who have sex with men (MSM) and people with a non-western migration background. Sociodemographic characteristics, HIV testing history, intention to test regularly, beliefs about personal risk and severity of HIV, and perceived social norms regarding HIV testing and people living with HIV were assessed among all who tested. A community quick scan assessed awareness of Amsterdam HTW 2016 and attitudes and intentions regarding HIV testing. Of 806 people tested, 59.6% (405/679) belonged to key populations. None tested HIV-positive and 37.6% intended to test regularly in the future. The community quick scan found moderate awareness of Amsterdam HTW 2016. Awareness was highest among recent testers and HIV-positive MSM and not associated with HIV testing attitudes and intentions. People tested during Amsterdam HTW 2016 were from key populations and/or were not (adequately) reached via traditional testing approaches. The contribution of the Amsterdam HTW approach to raising awareness and prompting HIV testing in key populations may benefit from focusing on HIV-negative individuals who have not been tested recently.
Keywords
Introduction
Timely diagnosing individuals with HIV is important for individual health outcomes and the prevention of HIV transmission.1,2 The proportion of people living with HIV (PLHIV) in the Netherlands who are unaware of being infected is estimated at 12%, although some studies estimate this proportion as larger. For Amsterdam specifically, 8% of PLHIV are estimated to be unaware of living with HIV.3,4 People who do not know their HIV status are found to disproportionately contribute to onward transmission. 5
Various approaches have been implemented to reduce the number of people who are unaware of their HIV infection in the Netherlands. Online, free, and anonymous HIV testing is available for men who have sex with men (MSM) at specific services in Amsterdam and other parts of the Netherlands, 6 and members of key populations can access sexually transmitted infection (STI) clinics for free HIV testing. All people can test for HIV at their request at their general practitioner (GP). HIV testing at a GP clinic may incur a cost for the person requesting the test, if their compulsory but capped financial contribution to annual health care costs has not yet been exceeded.
Despite the availability of these various client-initiated testing opportunities, people may experience barriers associated with HIV testing. An important psychosocial barrier is that people underestimating their risk of being infected with HIV are less likely to initiate testing themselves.7–9 People may also be reluctant to test when they are afraid of the consequences of testing HIV-positive, such as being stigmatised, and when people perceive few benefits from testing.7–9 The adverse social consequences of testing HIV-positive can be substantial, especially in groups in which stigma related to HIV and risk practices, notably sex between men, is high.10–13 Introducing testing opportunities that are initiated by providers, with as few as possible practical and social barriers, could prove vital to promote and normalise HIV testing.
Several provider-initiated approaches to HIV testing are in place in the Netherlands. For example, GPs are encouraged to offer HIV testing to people with symptoms possibly reflective of HIV indicator conditions.14,15 A study among six GP practices in the Amsterdam District Southeast showed that in the year prior to their HIV diagnosis, most people newly infected had consulted a GP, and more than half presented with an HIV indicator condition in the five years preceding diagnosis. 14 Moreover, pregnant women and people who donate blood are routinely screened for HIV infection.
The World Health Organisation recommends scaling up provider-initiated testing, as it presents an opportunity to ensure that HIV is more systematically diagnosed in health care facilities. 16 In the Netherlands, any scale up in testing opportunities needs to include MSM. Notably, the HIV epidemic in the Netherlands is concentrated among MSM. 4 MSM account for 68% of new HIV infections in the Netherlands and about one-third of MSM with HIV is diagnosed late. MSM are encouraged to test repeatedly, at least once every six months. 17 However, an 18 months monitoring study at all STI clinics in the Netherlands showed that less than one-fifth (18.9%) of MSM clients test for HIV every six months. 18
The HIV epidemic in the Netherlands also disproportionately affects people who migrated from high HIV prevalence countries. 4 In some communities of people with a non-western migration background, more than 40% of people with HIV is believed to be unaware of their HIV infection, 3 and MSM with a migration background and heterosexual women who migrated from sub-Saharan Africa are particularly likely to enter care late. 19 A recent review of possible barriers related to HIV testing among people with a migration background from low- and middle-income countries living in high-income countries identified several reasons for not testing for HIV, including a lack of knowledge of HIV, feeling healthy, low self-perceived risk of HIV infection, and concerns regarding confidentiality. 20 A study from Belgium further showed that when HIV testing was initiated by someone else, this facilitated uptake among people who migrated from sub-Saharan Africa. 21 This suggests that provider-initiated testing interventions may contribute to address at least some of the barriers to HIV testing experienced by people with a non-western migration background.
HIV Testing Week (HTW) initiatives, as part of provider-initiated approaches, have the potential to contribute to scaling up HIV testing during a specific period of time, in specific areas and possibly for specific populations. In 2016, the ‘HIV Transmission Elimination AMsterdam’ (H-TEAM) organised, for the second time, the Amsterdam HTW, which overlapped with international HIV Awareness Week (28 November–4 December 2016). During Amsterdam HTW 2016, free and anonymous rapid HIV testing was offered. Amsterdam HTW 2016 was supported by a multimedia promotion campaign, including a website (www.HIVtestweek.nl), in the weeks preceding and during Amsterdam HTW 2016. Amsterdam HTW 2016 is similar to the European HIV-Hepatitis testing week, 22 in that both aim to increase awareness of the benefits of HIV (and hepatitis) testing among key populations and to contribute to an increase in people aware of their HIV (and hepatitis) status. However, Amsterdam HTW 2016 took place a week after the European HIV-Hepatitis testing week and did not use any of its promotion materials. HIV Prevention England similarly organised an HTW. 23
Public Health England guidelines advise offering HIV testing proactively in areas where diagnosed HIV prevalence is between two and five per 1000 in the population aged 15–59 years. 24 Most districts of Amsterdam fulfil this criterion, supporting the city-wide approach of Amsterdam HTW 2016. Promotion of Amsterdam HTW 2016 and outreach activities were intensified in District Centre, District East and District Southeast, where HIV prevalence is over 15 per 1000 in the population aged 15–59 years. 25 Furthermore, Amsterdam HTW 2016 aimed to specifically reach the two key populations most affected by HIV in the Netherlands, MSM and people with non-western migration backgrounds, in line with guidelines recommending proactive testing among high-risk groups.26,27 The intensified focus districts are home to large communities of MSM and people with non-western migration backgrounds living in Amsterdam.
The present study aimed to evaluate whether Amsterdam HTW 2016 reached its goals of raising awareness of HIV testing and prompting HIV testing, especially among MSM and people with a non-western migration background. Diagnosing new HIV infections was not a primary goal of Amsterdam HTW 2016. To assess whether Amsterdam HTW 2016 prompted HIV testing among key populations, people testing for HIV in participating settings during Amsterdam HTW 2016 filled out a self-report questionnaire. To assess awareness of Amsterdam HTW 2016 and HIV testing attitudes and intentions, we performed a community quick scan in a sample recruited separately four weeks after the start of Amsterdam HTW 2016.
Methods
Amsterdam HTW 2016
Amsterdam HTW 2016 took place during international HIV Awareness Week, 2016 (28 November–4 December 2016). Reflecting an inclusive, non-stigmatising approach all interested people could test for free and anonymously during Amsterdam HTW 2016, using rapid HIV testing technology, with a specific focus on reaching the key populations of MSM and people with non-western migration backgrounds. The slogan of Amsterdam HTW 2016 was ‘Are you doing it too?’, which aimed to contribute to normalising HIV testing. A promotion campaign was disseminated through various types of media, including clean graffiti, social media, and 320 advertisements placed in Amsterdam subway stations and throughout the centre and Eastern regions of Amsterdam, and included a reference to the Amsterdam HTW 2016 website. The website (www.HIVtestweek.nl) provided more detailed information about Amsterdam HTW 2016 and included contact information of all participating HIV testing services. At these services, free and anonymous rapid HIV testing was offered.
Services that offered testing as part of Amsterdam HTW 2016 included four hospital clinics, 14 GP clinics, the STI clinic of the Amsterdam Public Health Service, and a community-based organisation (AIDS Healthcare Foundation [AHF]). Outreach testing took place in District East and District Southeast. Most services used the INSTI HIV1/HIV2 Rapid Antibody test (Biolytical TM, Laboratories Inc., Richmond, BC, Canada), which uses blood from a finger prick and provides a result within 60 s. 28 Two services (two hospital clinics) used the Determine™ HIV-1/2 Ag/Ab Combo test (Alere Inc., San Diego, CA, USA), which gives a result within 20 min, and which was routinely used at these services.
Survey of people testing for HIV
During Amsterdam HTW 2016, health care workers used a registration form provided to record informed consent, testing date and test result. The number of people who tested at participating services during Amsterdam HTW 2016 was calculated as the total number of unique registration forms lodged. All people who tested during Amsterdam HTW 2016 were asked to fill out a self-completed questionnaire adapted from Bartelsman et al., 28 which was available in Dutch and English. This included questions about sociodemographic characteristics (age, gender, country of birth of themselves, their mother and their father, and sexual preference) and HIV testing history (when and where). We added three questions on beliefs related to HIV and HIV testing, notably regarding perceived risk of HIV infection (‘The likelihood is high that I am HIV positive’ and ‘The likelihood I become HIV positive in the future is high’; response options: ‘certainly not’, ‘certainly’, and ‘I don’t know’) and perceived severity of HIV (‘I would really mind having HIV’; response options: ‘certainly not’, ‘certainly’, and ‘I don’t know’). We also added three questions about perceived social norms regarding HIV testing (‘What do people who are important to you think about you testing for HIV’) and people with HIV (‘How do people in your environment view people with HIV’ and ‘How would people who are important to you react if you were found to be HIV positive’; response options: ‘negative’, ‘neutral’, ‘positive’, and ‘I don’t know’; the additional response option ‘I would not tell any’ was added for the question about important others’ reaction to the participant being found HIV-positive). Furthermore, we added one question assessing participants’ intention to regularly test for HIV (e.g. every six months) in the future (response options: ‘certainly not’, ‘certainly’, and ‘I don’t know’).
Community quick scan
A community quick scan among MSM was performed three weeks after the start of Amsterdam HTW 2016, from 12 to 23 December 2016. We recruited participants from same-sex attracted men enrolled in Amsterdam PinkPanel, consisting of people willing to participate in research regarding LGBT community issues. Amsterdam HTW 2016 was not promoted through Amsterdam Pink Panel, which was only used to recruit MSM for the community quick scan. The community quick scan was also promoted though social media of STI AIDS Netherlands. Participants in the community quick scan completed a self-report questionnaire encompassing questions regarding sociodemographic characteristics, HIV testing history, intentions regarding future HIV testing, and beliefs and social norms related to HIV testing and living with HIV also included in the survey of people who tested for HIV. In addition, we asked whether participants had heard of the Amsterdam HTW in general and the Amsterdam HTW 2016 in particular (yes–no), and whether the Amsterdam HTW 2016 multimedia promotion campaign had contributed to conversations on HIV and HIV testing (yes–no). We also added four questions on attitudes (perceived importance, threat, difficulty, and embarrassment of HIV testing) and included two rather than one question on intentions regarding HIV testing (‘Do you intend to test for HIV in the next 6 months’ and ‘Do you intend to regularly test for HIV in the future’). Responses to questions asking about beliefs, social norms, attitudes, and intentions were given on 5-point scale, rather than on 3-point scale used in the survey of people who tested for HIV.
Data analysis
Data entry of participant responses to questionnaires was undertaken by a research assistant and checked by the first author. Descriptive statistics were calculated to assess baseline characteristics. The Pearson’s Chi square test was used to assess differences in HIV testing history, perceived risk of HIV, perceived severity of HIV, and social norms regarding HIV and HIV testing between MSM and heterosexual men and women, and between Dutch people and people with a migration background from non-western countries, either first or second generation. The classification of migration background was based on guidance provided by Statistics Netherlands.28,29 Sexual preference was self-reported and recoded into heterosexual or same-sex attracted. Analyses were performed with SPSS (IBM, version 24); a p-value of <0.05 was considered statistically significant.
Results
Survey of people testing for HIV
Sample characteristics
The number of people tested for HIV was 806; 29.0% (234/806) were tested at a hospital clinic, 17.1% (138/806) at the STI clinic of the Amsterdam Public Health Service, 41.6% (335/806) at a GP, 10.4% via AHF (84/806), and 1.9% (15/806) during outreach by the Amsterdam Public Health Service. None of the tests were positive. People who tested at AHF did not fill out the questionnaire for this study and could therefore not be included in further analyses, resulting in 722 eligible participants. In total, 94.0% (679/722) of these participants consented to filling out the questionnaire; see Table 1 for participant characteristics.
Characteristics of the participants in the participants’ survey and community quick scan (N = 679 and N = 143).
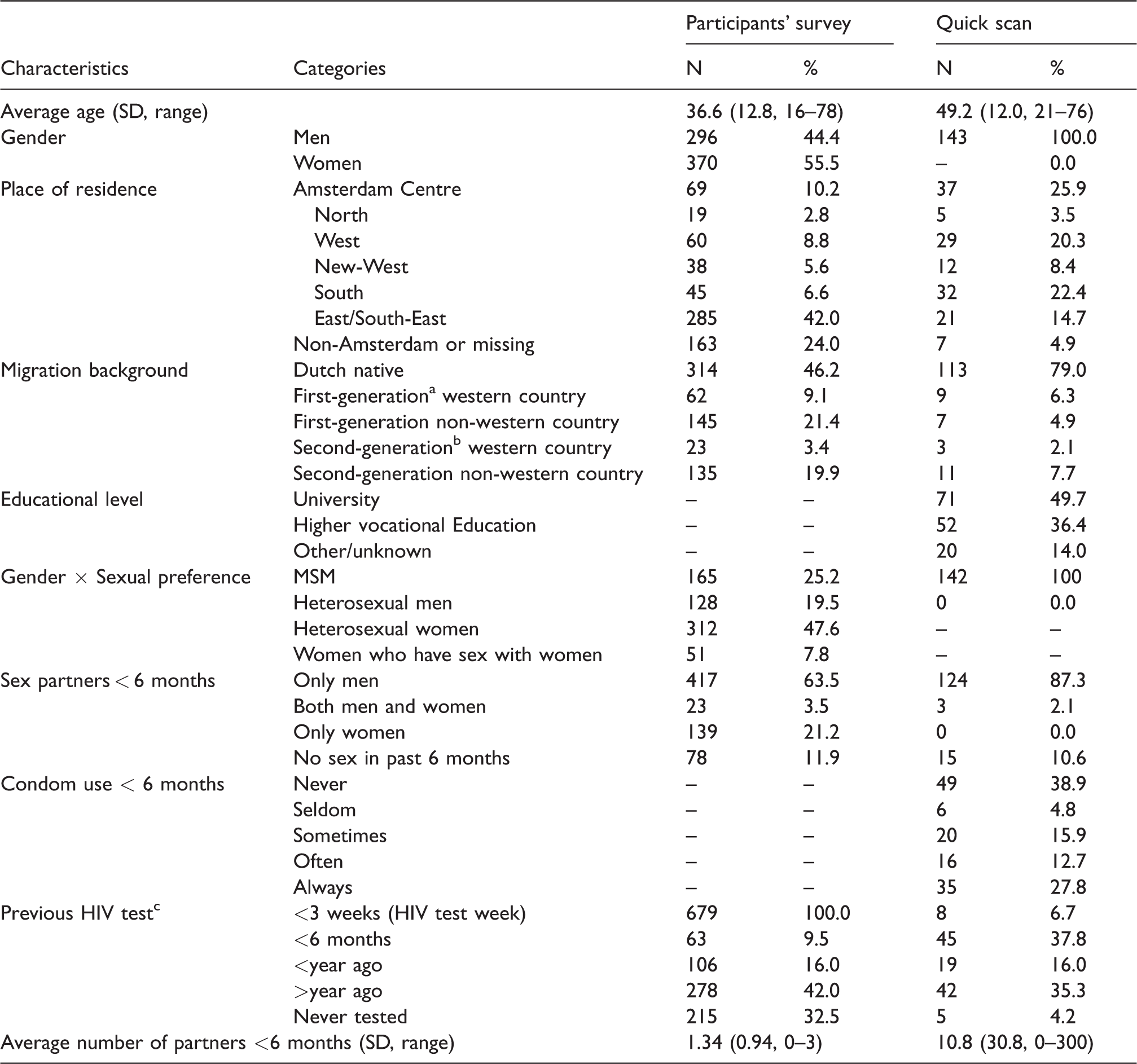
MSM: men who have sex with men; SD: standard deviation.
aFirst-generation migrant = participant is born in a country other than the Netherlands.
bSecond-generation migrant = at least one of the parents of the participant is born in a country other than the Netherlands.
cFor the participants’ survey we show the last and second to last HIV test.
Of the people who tested for HIV and completed the questionnaire, 59.6% (405/679) belonged to one of the two key populations. More than half of the men who tested identified as MSM (56.3%, 165/293; 24.3%, 165/679 of all testers). The majority of testers were born in the Netherlands (69.5%, 472/679), and 41.3% (280/679) had a first- or second-generation non-western migration background. In total 32.5% (215/662) of the participants had never tested for HIV before Amsterdam HTW 2016.
People could indicate multiple reasons for testing during Amsterdam HTW 2016. The most frequently endorsed reason was because of the opportunity provided by Amsterdam HTW 2016 (58.0%, 386/665). Rapidly receiving the test result was also an important reason for testing during Amsterdam HTW 2016 (33.6%, 224/667). Some people indicated that a reason for testing during Amsterdam HTW 2016 was that testing was free of charge (32.6%, 217/666). Also, some people indicated to have tested during Amsterdam HTW 2016 because they did not have to make an appointment (21.2%, 141/666).
Testing history and beliefs regarding HIV and HIV testing – all participants
Four out of ten participants (40.0%, 259/647) acknowledged they might be HIV infected or could become HIV infected in the future (38.1%, 248/651). Almost all participants (91.0%, 593/652) indicated that they considered HIV infection to be very severe. Regarding social norms, half of participants reported that people important to them would support their testing for HIV (52.2%, 339/649). Almost half viewed their environment as supportive of PLHIV in general (45.0%, 291/646), while perceived personal support was less if they would test positive (26.9%, 173/644). A third of participants indicated they intended to test regularly for HIV (37.6%, 245/652).
Testing history and beliefs regarding HIV and HIV testing – MSM
MSM were more likely (22.4%) to have tested in the last six months than heterosexual men and women (7.0 and 4.4%, respectively), χ2(6) = 65.42, p<.001. MSM were also more likely to perceive a risk to contract HIV now or in the future (48.8 and 46.9%, respectively) compared to heterosexual men and women. Fewer MSM felt people in their social environment had negative attitudes (39.6%) towards people with HIV as opposed to positive and neutral attitudes (60.4%). Most MSM intended to test regularly in the future (63.1%).
Testing history and barriers for HIV testing – people with a non-western migration background
People with a non-western migration background did not differ from Dutch people in previous HIV testing history (p = .41). Few people with a non-western migration background indicated that they expected that people important to them would support them if their HIV test would be positive (19.0%). They mostly expected that people in their social environment had negative attitudes towards people with living HIV (62.2%). Intentions to test regularly in the future were moderately high among people with a non-western migration background (43.0%).
Community quick scan
A total of 143 MSM participated in the community quick scan (see Table 1). Although some participants had a migration background, those who were born outside of the Netherlands had been living in the Netherlands for an average of 28.7 years (SD = 17.6, range 0.5–57). More than half of participants were familiar with Amsterdam HTW in general (54.6%, 77/141), of whom 85.7% (66/77) also knew of Amsterdam HTW 2016 in particular. Of the participants aware of Amsterdam HTW 2016, 78.5% (51/65) correctly identified the dates during which this was held. In addition, 53.3% (24/45) correctly indicated that the HIV test result was given within minutes, and 57.8% (26/45) correctly identified a finger prick test was used. Furthermore, while 15.4% (10/65) said to remember the slogan (of whom 30.0%, 3/10 remembered this correctly), 84.6% (55/65) did not remember the slogan (of whom 54.5%, 30/55 participants, nevertheless correctly identified it). Participants were neutral about the multimedia campaign to promote HTW (mean = 3.0, SD .91). Most did not talk about Amsterdam HTW 2016 with other people (86.7%, 39/45), nor about testing for HIV themselves because of Amsterdam HTW 2016 (91.1%, 41/45). A third of the participants found Amsterdam HTW 2016 beneficial (32.8%, 39/119).
Participant characteristics in terms of age, gender, place of residence, migration background, educational level, number of sex partners, and condom use were not associated with awareness of Amsterdam HTW in general or Amsterdam HTW 2016 specifically, apart from sexual preference and previous HIV testing. Men who had heard of Amsterdam HTW 2016 were less likely to also be sexually attracted to women, χ2(2) = 7.149, p = .028. In addition, men who tested regularly, or were HIV-positive, were more likely to be aware of Amsterdam HTW in general (χ2(1) = 5.09, p = 0.03), and Amsterdam HTW 2016 in particular (χ2(1) = 3.94, p = 0.057). Overall, MSM had favourable attitudes towards HIV testing (mean = 3.80, SD = 0.98), and most MSM had moderately high intentions to test for HIV (mean = 3.40, SD = 1.51). Attitudes regarding HIV testing and intention to test did not differ between participants who were or were not aware of the HTW 2016.
Discussion
Amsterdam HTW 2016 reached 806 people who tested at participating services; no HIV infections were detected. Feedback from participating health care professionals indicated that more people tested during this week than other weeks. Almost 60% of people tested belonged to the key populations targeted, MSM and people with a non-western migration background. Amsterdam HTW 2016 also reached people who are not or not adequately reached via traditional testing approaches. Most people tested during Amsterdam HTW 2016 had either never tested before (32.5%) or had tested longer than a year ago (42%). This inclusive approach represents an important extension of the focus on the two targeted key populations, encompassing people who likely had a personal reason to test for HIV and may be at increased risk of infection. Reported reasons for testing during Amsterdam HTW 2016 were related to the opportunity created by Amsterdam HTW 2016, providing further indication that Amsterdam HTW 2016 encouraged HIV testing.
The aim of Amsterdam HTW 2016 was to increase awareness and prompt HIV testing in MSM and people with a non-western migration background. As people who tested at participating sites during Amsterdam HTW 2016 by necessity were or became aware of Amsterdam HTW 2016, the community quick scan was undertaken to provide insight into awareness of Amsterdam HTW and intention to test for HIV in the future among MSM. This showed that awareness of Amsterdam HTW 2016 was moderate among MSM; men who had tested for HIV in the last six months and men who were HIV-positive were most likely to be aware of the HTW. Hence, the Amsterdam HTW might have attracted attention in groups that do not necessarily need an HTW to prompt them to test for HIV.
Comparing findings regarding people who tested during Amsterdam HTW in 2016 and 2015 28 showed that the total number of people tested was lower in 2016 when 806 people tested, compared to 1.231 in 2015. The proportion of people who belonged to one of the target groups was comparable (59.6 and 56.7% in 2016 and 2015, respectively). This difference in number of people tested in 2015 and 2016 may partly be explained by changes in implementation of Amsterdam HTW, with fewer outreach opportunities and one HIV testing service not participating in 2016. 28 The multimedia promotion campaign was also less extensively covered in the press in 2016 than in 2015. It is possible that people who do not test via the regular testing opportunities are also not persuaded by the Amsterdam HTW approach. Nevertheless, each additional person recently tested among the 806 individuals tested during Amsterdam HTW 2016 contributes to reaching the goal of 90% of people being aware of their HIV infection in 2020. 30
The community quick scan found that MSM were neutral in their evaluation of the multimedia campaign promoting Amsterdam HTW 2016. To improve the evaluation of the campaign and strengthen its impact on raising awareness and prompting of HIV testing in possible future iterations of Amsterdam HTW, involvement of the targeted key populations in the creation of the campaign could be strengthened. HIV testing and communication experts are advised to facilitate a process of co-creation involving MSM, people with a non-western migration backgrounds, as well as health care workers to better meet Amsterdam HTW aims.
A strength of the survey of people who tested for HIV during Amsterdam HTW 2016 is that it is known how many people tested during the HTW at the participating locations, albeit no data are available to assess the reach of HTW by comparing number of people tested with a similar normal week. Importantly, 94% of eligible people participated in the survey. A limitation is that there were differences in how participating services organised Amsterdam HTW 2016. At some services, people wanting to test for HIV had to make an appointment, whereas at other services people could walk-in; several services offered a combination of these options. Also, most services used the INSTI test, whereas some (i.e. two hospitals) used their usual, different test. While this should not have affected detection of HIV infections, HIV testing experiences may have differed. A limitation of the community quick scan is the small sample size. Furthermore, the sample was recruited from only one of the two targeted key populations (i.e. MSM) and included few MSM with a non-western migration background. MSM participating in the community quick scan are not representative of the broader community of MSM in Amsterdam and likely more motivated to participate in research and more interested in issues related to sexuality, HIV, and HIV testing. Awareness of Amsterdam HTW as found in the sample may hence be lower in the broader MSM community in Amsterdam.
Conclusion
Although no new HIV infections were detected, Amsterdam HTW 2016 likely contributed to promoting HIV testing, and reaching key populations (i.e. MSM and people with a non-western migration background) as well as other people who may experience a risk of HIV and have not tested before or have not recently tested. Reasons indicated for testing underscore the opportunity created by Amsterdam HTW 2016 and the multimedia promotion campaign, further suggesting that Amsterdam HTW 2016 encouraged HIV testing. Awareness of Amsterdam HTW 2016 was moderate among MSM, and intentions to test for HIV in the future were not related to this awareness. Co-creation with MSM, people with a non-western migration background, and HIV testing providers may strengthen the impact of future Amsterdam HTW on gaining awareness and prompting HIV testing in key populations.
Footnotes
Acknowledgements
The authors would like to thank all partners of the ‘HIV Transmission Elimination AMsterdam’ (H-TEAM) initiative who were involved in the organisation of the HTW, especially the partners involved in Work Package 2. The H-TEAM is a unique collaboration in Amsterdam, the Netherlands. By combining education, prevention, testing, and treatment, the H-TEAM can stop the spread of HIV and keep PLHIV in good health. We would also like to thank participating health care professionals at all the HTW testing locations and all participants in the study.
H-TEAM initiative
H-TEAM Steering Committee: J.E.A.M. van Bergen6,4,5,30, G.J. de Bree1,2, P. Brokx8, F. Deug6, M. Heidenrijk1, M. Prins3,2, P. Reiss1,7 (chair), M. van der Valk2
H-TEAM Core Project Group: J.E.A.M. van Bergen6,4,5,30, G.J. de Bree1,2 (chair), P. Brokx8, U. Davidovich3, S.E. Geerlings2, E. Hoornenborg3, A. Oomen6, A. van Sighem7, W. Zuilhof6
H-TEAM Project Management: M.L. Groot Bruinderink1
H-TEAM additional collaborators: R.C.A. Achterbergh3, M. van Agtmael24, J. Ananworanich22, D. Van de Beek17, G.E.L. van den Berk11, D. Bezemer7, A. van Bijnen6, W.L. Blok11, M. Bomers24, C.A.B. Boucher13, W. Brokking26, D. Burger20, K. Brinkman11, N. Brinkman33, M. de Bruin12, S. Bruisten3, R. van Crevel29, L. Dellemann6, M. Dijkstra3, Y.T. van Duijnhoven3, A. van Eeden26, L. Elsenburg26, C. Ester7, P.H.J. Frissen11, T.B.H. Geijtenbeek18, M.H. Godfried2, J. van Gool3, A. Goorhuis2, M. Groot26, C.A. Hankins1, A. Heijnen31,32, M.M.J Hillebregt7, A. Hogewoning3, J.W. Hovius2, K. de Jong3, R. Kemp33, N.A. Kootstra19, R.A. Koup21, M. Kroone3, F.P. Kroon16, F. Lauw25, K. Lettinga27, I. Linde3, L. May3, E. Meddens6, J.T. van der Meer2, S. van Meeteren3, T. Mouhebati6, J. Mulder25, F.J. Nellen2, A. Nijsters6, H. Nobel2, P. Oostvogel3, E.L.M. Op de Coul5, E. Peters24, I.S. Peters3, T. van der Poll2, O. Ratmann28, C. Rokx14, M.S. van Rooijen3, M.F. Schim van der Loeff3,10, W.E.M. Schoute11, G.J. Sonder3, J. Veenstra27, A. Verbon14, F. Verdult8, G.R. Visser7, J. de Vocht24, H.J. de Vries3,9,10, S. Vrouenraets25, M. van Vugt2, W.J. Wiersinga2, F.W. Wit2, L.R. Woittiez2, S. Zaheri7, P. Zantkuijl6, M.C. van Zelm23, A. Żakowicz15, F.R. Zuure3.
Department of Global Health, Academic Medical Center, and Amsterdam Institute for Global Health and Development, Amsterdam, the Netherlands Department of Internal Medicine, Division of Infectious Diseases, Academic Medical Center, Amsterdam, the Netherlands Department of Infectious Diseases, Public Health Service of Amsterdam, Amsterdam, the Netherlands Department of General Practice, Academic Medical Center, University of Amsterdam, Amsterdam, the Netherlands Epidemiology and Surveillance Unit, Centre for Infectious Disease Control, National Institute of Public Health and the Environment, Bilthoven, the Netherlands STI AIDS Netherlands, Amsterdam, the Netherlands Stichting HIV Monitoring, Amsterdam, the Netherlands Dutch Association of PLHIV, Amsterdam, the Netherlands Department of Dermatology, Academic Medical Center (AMC), University of Amsterdam, Amsterdam, the Netherlands Center for Infection and Immunology, Amsterdam (CINIMA), Academic Medical Center (AMC), University of Amsterdam, Amsterdam, the Netherlands Department of internal medicine, Onze Lieve Vrouwe Gasthuis, Amsterdam, the Netherlands Aberdeen Health Psychology Group, Institute of Applied Health Sciences, University of Aberdeen, Aberdeen, UK. Department of Viro-science, Erasmus Medical Center, Rotterdam, the Netherlands Department of Internal Medicine and Infectious Diseases, Erasmus University Medical Center, Rotterdam, the Netherlands AIDS Healthcare Foundation, Amsterdam, the Netherlands. Department of Infectious Diseases, Leiden University Medical Centre, Leiden, the Netherlands Center of Infection and Immunity Amsterdam (CINIMA), Department of Neurology, Academic Medical Center, Amsterdam, the Netherlands Laboratory of Experimental Immunology, Academic Medical Center, Amsterdam, the Netherlands Laboratory for Viral Immune Pathogenesis, Academic Medical Center, Amsterdam, the Netherlands Department of Pharmacy, Radboud University Nijmegen Medical Center, Nijmegen, the Netherlands Immunology Laboratory, Vaccine Research Center, NIAID, National Institutes of Health US Military HIV Research Program and the Henry M. Jackson Foundation for the Advancement of Military Medicine, Bethesda, United States Department of Virology, Erasmus Medical Center, Rotterdam, the Netherlands Department of Internal Medicine, Free University Medical Center, Amsterdam, the Netherlands Department of Internal Medicine, Slotervaart Hospital Amsterdam, the Netherlands DC Clinics, Amsterdam, the Netherlands Department of Internal Medicine, Lukas Andreas Hospital, Amsterdam, the Netherlands School of Public Health, Faculty of Medicine, Imperial College London, London, United Kingdom Department of Internal Medicine, Radboud University Nijmegen Medical Center, Nijmegen, the Netherlands Health Centre Venserpolder, Amsterdam, the Netherlands Sexology Centre Amsterdam, Amsterdam, the Netherlands GP practice Heijnen & de Meij, Amsterdam, the Netherlands 1ste Lijn Amsterdam, Amsterdam, the Netherlands
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The H-TEAM initiative is being supported by Aids Fonds (grant number: 2013169), Stichting AmsterdamDiner Foundation, Bristol-Myers Squibb International Corp. (study number: AI424-541), Gilead Sciences Europe Ltd (grant number: PA-HIV-PREP-16-0024), Gilead Sciences (protocol numbers: CO-NL-276-4222, CO-US-276-1712), Janssen Pharmaceutica (reference number: PHNL/JAN/0714/0005b/1912fde), M.A.C AIDS Fund, ViiV Healthcare (PO numbers: 3000268822, 3000747780), and ZonMw (grant number: 522002003).