
Abstract
This national audit of 142 clinics demonstrated that the majority of clinics surveyed had policies and agreed clinical practice for alcohol and recreational drug enquiry, as well as documentation of HIV test refusal, although this was not the case in 24% of clinics as regards alcohol usage, 21% of clinics as regards recreational drugs use and 43% of clinics as regards chemsex usage. Regarding management of HIV test refusal, there was no policy or agreed practice in 13% of clinics with respect to men having sex with men (MSM) attenders, and in 18% of clinics for heterosexual attenders. Seventy percent of clinics had HIV point of care tests (POCT) available. Recommendations include: all clinics should have a policy of routine enquiry about alcohol, recreational drugs and chemsex, all clinics should record reasons for HIV test refusal and all clinics should provide testing alternatives to improve uptake, e.g. point of care testing or home sampling.
Introduction
The British Association for Sexual Health and HIV (BASHH) and the Medical Foundation for HIV & Sexual Health (MedFASH) Standards for the Management of Sexually Transmitted Infections recommend that patients attending sexual health clinics be offered screening for sexually transmitted infections (STIs) including HIV. 1 In addition, BASHH guidelines recommend obtaining a history of alcohol and recreational drug use from patients attending for an STI screen. 2 Currently there is no specific guidance on history taking for chemsex, although this is associated with high-risk sexual practices and STIs, including HIV acquisition. 3
The UK National Guidelines for HIV testing recommend that the reasons for test refusal should be documented. 4 Specific recommendations are limited to test re-offer for pregnant women and point-of-care testing when venepuncture is refused. Of note, 14% of men who have sex with men (MSM) attending UK genitourinary medicine (GUMed) clinics in 2013 were not tested for HIV. 5 Nearly one in ten MSM diagnosed with late stage HIV infection (CD4 cell count <200 cells/μL) in GUMed clinics in the UK before April 2014 had a prior clinic attendance where they were not tested for HIV, representing possible missed opportunities for earlier diagnosis. 6
This paper reports the findings of the clinic policy review part of the BASHH National Audit of HIV testing, with the accompanying paper reporting the results of the related case note audit. 7
Objective and goal
The objective was to measure clinics’ policy concordance with Specialty guidance for the offer of HIV testing, as well as risk assessment with regard to alcohol and recreational drug use. Additionally, information was sought on two areas not yet covered by Specialty guidance: recording the reasons for non-uptake of HIV test offer and subsequent action taken, and history taking in relation to chemsex. The aim was to investigate the coverage of relevant policies and whether this influenced clinical practice and adherence to national guidelines, highlight areas of good practice and areas for improvement to support future improvements in performance, and, in particular, to contribute to reduction in late presentation of HIV infection, in line with national guidance.4,8,9
Methods
The detailed audit methodology is described in detail in the accompanying paper on the case note review. 7 In short, all GUMed clinics in the UK were invited to complete an online questionnaire on clinic HIV-testing policies that existed at the time of the audit start date (26 February 2016). The audit period was between 26 February 2016 and 30 April 2016. The BASHH National Audit Group (NAG) developed the Audit questionnaires by piloting questions with practising clinicians, and agreeing final versions through re-iteration. Eligible services for participation were level 3 GUMed clinics in the UK. The subject areas covered were alcohol and substance misuse and associated care pathways, management of HIV test refusal and HIV test modalities available; and whether these were in the form of formal policy, routine practice or neither. The Audit questions were presented using the online LimeSurvey 10 tool, for completion by clinic staff, and allowing the return of pseudoanonymised data. Responses to clinic policy questions were collated into a national aggregate to allow comparisons between clinic policies, and with regard to particular risk groups. Regional data (based on BASHH regions) and individual clinic performance data have been disseminated to relevant clinics.
Results
One hundred and forty-two clinics participated, of which 88 (62%) described themselves as providing level 3 sexual health care, and 54 (38%) as providing both levels 3 and 2 (integrated sexual health care).
Clinic responses regarding their policy on routine enquiry about alcohol, recreational drugs and chemsex for both MSM and for heterosexual men and women are shown in Table 1. The figures in the table represent both the average response, taking into account all clinic replies, as well as the range of responses from individual clinics (BASHH Branch range). It is particularly noteworthy that 43% of clinics do not routinely ask about chemsex in MSM attenders.
Clinic policy on obtaining alcohol, recreational drug and chemsex histories.
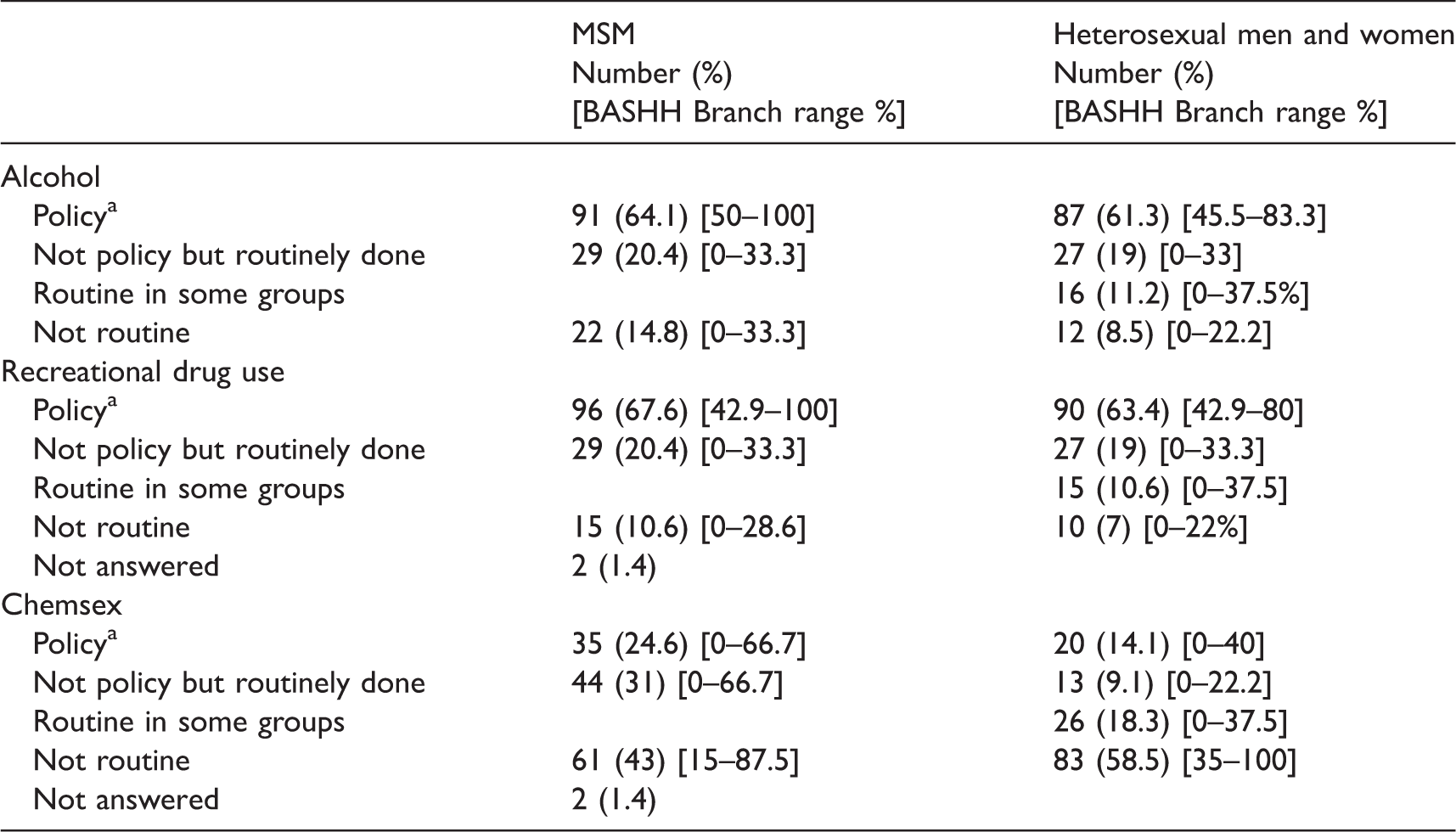
aSome clinics stated this was a routine question in some groups.
Eighty-eight of 142 clinics (62%) did not use any tool for alcohol assessment, although 109 (76%) did have an agreed pathway in place should a history of potential misuse be obtained. One hundred and fifteen (81%) did not use a tool for recreational drug use assessment, although an agreed care pathway was available for potential misuse in 100 (70%) clinics. One hundred and twenty-six clinics (82%) did not use a tool for assessment of chemsex, but an agreed care pathway was available in 57 (40%) clinics.
Clinic policies for managing HIV test refusal were as shown in Table 2. Of note, 19 (13%) of clinics had neither a written policy nor agreed common practice as regards the action to be taken if an MSM patient declined an HIV test offer. The equivalent figure for heterosexual patients was 26 clinics (18%).
Clinic policy on HIV test refusal, according to risk group.

Furthermore, 99 (70%) clinics had a policy of offering alternatives to venepuncture. In 87 cases, this was a finger prick point of care test (POCT), and in 12 this was an oral fluid test.
Discussion
The majority of clinics surveyed had policies and agreed clinical practice for alcohol and recreational drug enquiry, as well as documentation of HIV test refusal. The results of this Audit should be interpreted in light of the following limitations. No specific validation process of the questions used was carried out because of limited resource. However, this lack of validation may have had limited effect since the questions asked were all relatively simple. Very little feedback as regards difficulty answering questions was received by the audit organisers. Opportunities for feedback from clinicians completing the survey were available throughout the audit period.
Our findings highlight the lack of routine policy or agreed clinical practice of taking a history of alcohol and recreational drug use in 24% and 21% of clinics, respectively. Alcohol intake is a well-recognised risk factor for sexual ill health and risk taking; a systematic review reported that eight of 11 studies using specific measures of problem drinking found a significant association between alcohol consumption and at least one STI. This finding was independent of gender or pattern of alcohol consumption assessed. 11 In addition, despite evidence of increased risk-taking behaviour with chemsex, 3 43% of clinics do not have a policy of routine enquiry about this.
Regarding management of HIV test refusal, there was no policy or agreed practice in 13% of clinics with respect to MSM attenders, and in 18% of clinics for heterosexual attenders. Identifying the reasons for refusal may allow concerns and barriers to be addressed, and thereby increase testing rates especially in those most at risk, e.g. MSM. The BASHH/BHIVA UK National Guidelines for HIV Testing, 2008 recommends offering HIV POCT testing to those refusing venepuncture, although few data are available on the acceptability of POCT in this setting. However, we found only 70% of clinics had POCT available. Recently published NICE guidelines have reiterated criteria for HIV testing uptake in both primary and secondary care, as well as in community settings. Furthermore these guidelines cover opportunities for increased HIV testing, including the use of POCT, self-sampling and repeat testing. 12 Future specialty HIV testing recommendations should consider these guidelines as well as other interventions that might increase HIV testing uptake, including home/self-testing, postal testing, offer of another opportunity for testing in a clinic, or information about testing at other sites (including that provided by voluntary services), or the provision of oral fluid testing. 13
Recommendations
To improve practice the BASHH NAG recommend:
Clinics should introduce a policy of routinely enquiring about alcohol, recreational drugs and chemsex. Clinics should record reasons for HIV test refusal. Clinics should provide testing alternatives to improve uptake (e.g. POCT, home sampling, etc.)
Footnotes
Acknowledgements
We would like to acknowledge the contributions of all NHS GU clinic staff who submitted data and supported the audit. Membership of the National Audit Group (July 2016): Ann Sullivan (Chair), Hugo McClean (Vice chair), David Daniels, Vanessa Apea (Hon sec and Thames North), Christopher Carne (Hon Vice Chair) Anatole Menon-Johansson (Director of Development); Amelia Hughes (Thames South East), Andrew De Burgh-Thomas (South West), Andy Williams (Thames North), Cara Saxon (N West), Ciara Cunningham (Scotland), Emma Street (Yorkshire), Erna Buitendem (NCSP), Gurmit Jagjit Singh (Training grades), Helen Wiggins (Trainees’ Collaborative for Research, Audit and Quality Improvement), Huw Price (Essex), John Saunders (NCSP), Kanchana Seneviratne (Training grades), Liz Anderson (Merseyside), Manjula Pammi (Trent), Meena Sethupathi (Wales), Sara Scofield (Wessex), Sarup Tayal (Northern), Say Quah (Northern Ireland), Serish Basavaraj (Anglia), Sophie Brady (CGC), Steven Estreich (Thames South West), Sumit Bhaduri (West Midlands), Nisha Pal (Oxford).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.