
Abstract
HIV testing and counselling is crucial in identifying new HIV cases and linking them to treatment. Provider-initiated testing and counselling can help to increase uptake of HIV testing and counselling and HIV case detection. We implemented provider-initiated testing and counselling in 32 health facilities in Ebonyi State, South-East Nigeria in order to achieve both objectives. Provider-initiated testing and counselling was implemented across the 32 facilities from January to June 2016. Provider-initiated testing and counselling data were compared with the preceding six months (July–December 2015) when only voluntary counselling and testing was done. A total of 11,787 out of 22,153 who visited the outpatient clinics within the intervention period (53%) were tested. In the preceding six months, only 3172 clients were tested via voluntary counselling and testing out of 50,898 clients who visited the outpatient clinics (6.2%). This was a 3.72-fold increase over the numbers tested via voluntary counselling and testing, within a similar time frame. Also, 158 new cases were diagnosed during the period from provider-initiated testing and counselling compared to 24 from voluntary counselling and testing in the preceding six months – an increase of 4.65-fold in case detection. Apart from the 11,787 tested through provider-initiated testing and counselling, another 6999 clients were tested through community-based outreaches during the intervention period. Comparison of case detection between both strategies shows that provider-initiated testing and counselling accounted for 158 cases (97%) while outreaches accounted for only five cases (3%). Provider-initiated testing and counselling led to an increase in uptake of HIV testing and counselling services as well as in HIV case detection across the 32 facilities where our programme was implemented.
Keywords
Background
HIV testing and counselling (HTC) is the first crucial step for linkage to HIV treatment and prevention. However, despite the high HIV burden in sub-Saharan Africa, testing coverage is low, particularly among young adults and men. In Nigeria, which has the second highest burden of HIV in the world, 1 only 23% of males and 29% of females reported testing within a 12-month period according to the 2012 National HIV & AIDS and Reproductive Health Survey. 2 As a result, the majority of people living with HIV in Nigeria are unaware of their status.
A lot of extra-facility interventions, such as community-based HTC and outreaches have proven effective in reducing this testing gap.
3
However, guidelines from WHO and other expert bodies have recommended that provider-initiated testing and counselling (PITC) at health facilities is an effective strategy to increase uptake of testing and counseling.4,5 For a country like Nigeria with a generalized epidemic, the summary guidance on PITC recommends that health care providers should recommend HTC to all adults and adolescents seen in all health facilities. This applies to medical and surgical services, public and private facilities, inpatient and outpatient settings and mobile or outreach medical services. HTC should be recommended by the health care provider as part of the normal standard of care provided to the patient, regardless of whether the patient shows signs and symptoms of underlying HIV infection or the patient’s reason for presenting to the health facility.
4
This paper describes findings obtained from a programme which implemented PITC across 32 health facilities in Ebonyi State, South-Eastern Nigeria.
Methods
Setting
Between January 2014 and December 2016, Catholic Relief Services Nigeria implemented a HIV prevention, care and treatment programme in 32 health facilities across seven local government areas (LGAs) in Ebonyi State, South-Eastern Nigeria. The programme was part of the Global Fund Round 9 Phase 2 (January 2014 – June 2015) and New Funding Model (NFM; July 2015 – December 2016) grants superintended by the National Agency for the Control of AIDS (NACA) across Nigeria between July 2015 and June 2016. In these 32 facilities – comprising seven secondary health centres (SHCs) and 25 primary health centres (PHCs) – PITC was previously implemented only in antenatal clinics (ANCs), but not in the outpatient clinics. The SHCs also had HTC units where voluntary counselling and testing (VCT) was offered. The Global Fund NFM HIV grant had very high testing and counselling targets, necessitating the implementation of various strategies to increase testing and counselling uptake. Thus, the programme team introduced PITC at the outpatient units of the 32 facilities. In addition, community-based testing and counselling outreaches were also carried out in the communities surrounding each facility using trained volunteers.
In all instances, rapid test kits (RTKs) were used to carry out the tests, using the serial testing algorithm recommended by the National HTC guidelines. 12 Determine test kits were used for initial screening. If a result was negative, it would be given to the client as HIV-negative. If the result obtained was positive, the blood sample was tested using the Unigold test kit. If the second test was also positive, the result was given to the client as HIV-positive. If the second test, however, was negative, the Stat-Pak test kit was then used as a tiebreaker, and the result, positive or negative, was given to the client as the decisive one. Across the 32 facilities, facility staff were retrained on the use of the RTKs, while HTC standard operating protocols, job aids and the national guidelines were placed on their walls and tables.
The programme team in Ebonyi State started by engaging with facility staff on the proposed PITC implementation, encouraging them to test all clients coming to access health services in their facilities irrespective of presenting complaints. Between July and December 2015, various forums were used for these engagements including LGA programme review meetings known as Cluster Coordination Meetings, data collation meetings as well as routine mentoring visits to the facilities. In most of the SHCs, HTC points were set up at the outpatient clinics, in order to ensure that both testing and counselling were offered in the same location as the consultation. In two SHCs – General Hospital Owutu-Edda and St Vincent’s Hospital Amudo – clients were counselled at the point of service, while the testing was carried out in the hospital laboratory. The PHCs were smaller in size and with fewer staff, so the staff offered the HIV tests at any time they saw clients in their facilities. The programme team mentored the health workers repeatedly to ensure that clients could opt out if they wished. All the 32 facilities also had HIV counselling and testing points set up at their Directly Observed Treatment Short-course (DOTS) centres for TB clients. All these points of testing will be referred to as outpatient clinics. Inpatients were also offered testing at their outpatient or emergency consultations prior to admission.
During the period of engagement and advocacy, there was initial resistance from the health workers, who believed that PITC would increase their workload. However, the team worked with them to define and delegate roles, ensuring that no individual was overburdened. After six months of advocacy, implementation commenced across the 32 supported facilities in January 2016. In addition to the six months of advocacy, the programme team continued providing on-site support and mentoring during the implementation, ensuring that the health workers adhered to the agreed PITC protocol. The team also ensured that RTKs remained available across all the sites, facilitating inter-facility transfers where necessary to ensure that there was no disruption to testing due to stock-outs. It is pertinent to mention here that no other incentives, financial or otherwise, were given.
Data collection
PITC data were to be collected and reviewed between January and June 2016. To ensure that the facilities were indeed implementing PITC, the number of new clients accessing services in the facility was compared monthly with the number of clients tested for HIV within the facility. This was done by reviewing each facility’s outpatient register (including DOTS centres) and HTC register, respectively. To assess the additional impact of PITC implementation on uptake, VCT data were also collected for the six-month period prior to implementation (the advocacy phase) for purposes of comparison.
In addition to PITC, the programme team also organized monthly HTC outreaches in surrounding communities using trained HTC volunteers. The outreaches were a combination of campaign-type testing focusing on community rendezvous points like motor parks and markets, as well as fixed points such as town squares. In both cases secluded booths were always provided for confidentiality during individual counselling and testing. These monthly campaigns were usually preceded by advocacy meetings with community leaders, including leaders of the motor parks and markets. Targeted communities were the towns/villages in the political ward in which the health facility was located, with the outreaches rotated to a different village each time in order to avoid double testing of same individuals as much as possible. Data were collected from these outreaches using client intake forms, which were then collated and analysed by the volunteers and subsequently transferred to the appropriate section on the facilities’ HTC register.
It should be mentioned that clients targeted were adolescents and adults aged above 15 years who had come to seek care of their own accord and were given the opportunity to opt out. This is in line with the National HIV Counselling and Testing Guidelines 12 which allow for mature minors to be able to give consent if seeking care by themselves.
Since PITC was already being implemented in the ANCs, ANC data were excluded from this review.
Results
Utilization and case detection: PITC versus VCT
PITC was well accepted by clients across all the facilities. Of a total of 22,153 non-ANC clients who visited the outpatient clinics across the 32 facilities within the review period, 11,787, or 53%, were tested. The numbers not tested are those who opted out. In the preceding six months, only 3172 clients were tested via VCT out of 50,898 clients who visited the outpatient clinics – a mere 6.2%.
The gross number of clients tested via PITC was 3.72 times more than the gross number of clients tested via VCT, within a similar time frame. Also, 158 new cases were diagnosed during the period from PITC compared to 34 from VCT in the preceding six months. This represented a 4.65-fold increase in cases detected, and a prevalence rate of 1.34 for PITC compared to 1.07 for VCT.
Case detection: Facility testing versus community outreaches
Comparison of HTC utilization and case detection between PITC and VCT.
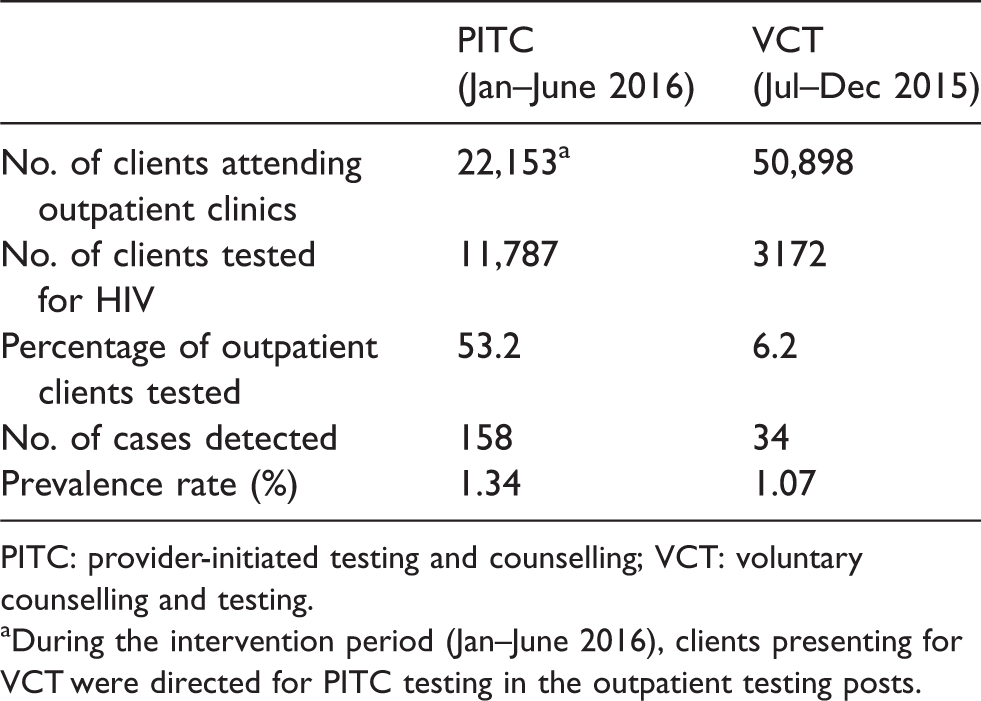
PITC: provider-initiated testing and counselling; VCT: voluntary counselling and testing.
aDuring the intervention period (Jan–June 2016), clients presenting for VCT were directed for PITC testing in the outpatient testing posts.
Prevalence rates obtained from PITC and VCT were higher than those from outreaches.
Uptake and case detection: SHCs versus PHCs
Of the 11,787 clients tested via PITC across the 32 facilities, 4875 (41.4%) were tested in the seven SHCs, while the remaining 6912 (58.6%) were tested in the 25 PHCs. However, 83% of the 158 cases detected (131) were at the SHCs.
Discussion
The effectiveness of PITC as a strategy to increase uptake of HTC is not in doubt. Several studies from around sub-Saharan Africa have shown that resistance by patients to PITC is very low, resulting in high HTC uptake rates.5,8,13–16 Findings from our implementation of PITC across these 32 facilities in Ebonyi State were consistent with this fact, with a 272% increase in number of clients tested in facilities after PITC was introduced.
Perhaps the more significant finding from our implementation of PITC was the higher HIV detection rates from PITC compared to outreaches. PITC accounted for 62.7% of those tested within the period and 97% of new HIV cases detected. This suggests therefore that PITC is indeed a more effective strategy to detect new HIV infections. This finding is also consistent with other studies from other African countries such as Uganda, South Africa, Zambia and Zimbabwe.17–22 An associated finding was that while VCT was not as effective as PITC in detecting new cases because of its lower HTC uptake, it still proved to be more effective than community testing. This appears to demonstrate that facility testing of any kind will yield more new cases than community-based testing.
PITC is also more cost effective and less time consuming than community outreaches. 17 The programme invested significant financial resources on the outreaches, incurring costs on volunteer stipends, transportation and community mobilization. On the other hand, apart from the RTKs and consumables used by the health workers, PITC had no extra costs. In the light of resource constraints within the public health space in Nigeria, especially reduced funding from donors for HIV/AIDS, PITC presents a cost-effective opportunity for increasing HTC uptake and detecting new HIV infections. With its focus on health facilities, it also helps to facilitate on-site linkage to care and treatment for the newly diagnosed cases.
Limitations
This paper has some potential limitations. First is that during the intervention period, clients requesting VCT services were subsumed under the new PITC protocol and were thus tested at the outpatient service points. Continuing VCT services alongside PITC may have helped to segregate the impact of counselling and testing offered by providers as against those sought by clients themselves. Second, only 53% of clients offered PITC accepted to be tested and were subsequently tested. Our review was not able to profile the demographics of those who accepted and those who rejected PITC. It is also possible that there may have been some missed opportunities caused by providers forgetting to offer HTC. Also, the overall data are not segregated by gender or by geographical characteristics such as rural versus urban areas. The positivity rate specifically for TB patients tested for HIV at the DOTS centres was also not isolated, as TB/HIV was not the focus of the paper. Finally, it appeared that a significantly higher number of clients sought care at the outpatient units of the facilities in the pre-intervention period compared to the intervention period (50,898 as against 22,153). One possible explanation here is that while there was stringent data supervision by the programme team during the PITC phase, with the health workers well mentored on not double counting clients revisiting the facilities, there may have been double counting of revisiting clients during the VCT phase.
Strengths
Comparison of HIV detection rates between facility testing and outreaches.

PITC: provider-initiated testing and counselling; VCT: voluntary counselling and testing.
Conclusion
PITC led to an increase in uptake of HTC services as well as in HIV case detection across the 32 facilities where our programme was implemented. With respect to these two parameters – uptake and case finding – PITC cost a lot less than community-based testing, but produced better results.
Footnotes
Authors’ contributions
RN was programme team lead and lead writer for this paper. GU and CA oversaw implementation at the facilities and contributed to the writing of the paper. MO and IO were responsible for data collection, collation and analysis. EP contributed to the writing process.
Acknowledgements
We are grateful to the Global Fund, under whose NFM Grant our programme was implemented. We also thank the NACA, the Ebonyi State Ministry of Health and the Ebonyi State Agency for the Control of AIDS for their support and oversight during the programme implementation. We truly appreciate the efforts of the hardworking health workers at the 32 health facilities, without whom the programme would have been impossible. Data collated and analysed for this paper were extracted from the quarterly M&E reporting tools designed for the Global Fund NFM HIV/AIDS programme by the NACA Abuja. These reports are available both in the records of NACA and Catholic Relief Services, Nigeria. However, the findings and conclusions in this paper are the responsibility of the authors and do not necessarily represent the views of the Global Fund, NACA or Catholic Relief Services.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.