
Abstract
Routine infectious diseases screening of Sudanese pregnant women has been patchy due to scarcity of healthcare resources and social stigma. We sought to determine the seroprevalence of HIV, hepatitis B, and syphilis among pregnant women attending antenatal care (ANC) at El Obeid Maternity Hospital in western Sudan. We also explored the association between these infections and a set of socio-demographic and maternal variables. Unlinked anonymous testing for HIV-1/2 antibodies, hepatitis B surface antigen, and Treponema pallidum antibodies was performed on residual blood samples collected during routine ANC (August 2016–March 2017). Seroprevalence of HIV was 1.13% (5/444; 95% CI 0.37–2.61%), hepatitis B 2.93% (13/444; 95% CI 1.57–4.95%), and syphilis 7.43% (33/444; 95% CI 5.17–10.28%). On bivariate analysis, there were no statistically significant associations between hepatitis B, syphilis, or a composite outcome including any of the three infections and age, stage of pregnancy, gravidity, parity, previous mode of delivery, history of blood transfusion, or husband polygamy. Urgent action is needed to scale up routine maternal screening for HIV, hepatitis B, and syphilis on an opt-out basis. Further research into the socio-demographic and behavioural determinants of these infections as well as their clinical outcomes is needed.
Introduction
Precise data on the incidence and prevalence of sexually transmitted infections (STIs) in Sudan, especially among pregnant women, remain elusive. Social stigma, scarce resources, poor public health infrastructure, red tape practices preventing access to vital information stored in non-indexed governmental reports, sparse scientific research output, and overreliance on donor-driven sentinel surveillance exercises are examples of the difficulties impeding better understanding of the situation in Sudan. 1
There are major disparities in access and utilisation of antenatal care (ANC) in Sudan leading to patchy and unsatisfactory testing and treatment of STIs during pregnancy. 2 This situation is further compounded by social stigma attached to STIs and the prohibitive cost of investigations and treatment that patients must shoulder using their own limited resources.
Despite an estimated low prevalence of HIV of 0.2% among people aged 15–49 years, Sudan has witnessed an alarming increase in the burden of new HIV infections as well as AIDS-related deaths in the period from 2005 to 2013. 3 Sudan accounted for 20.8% of all new HIV infections and 20.7% of all AIDS-related deaths reported in the Middle East and North Africa (MENA) region during that period. 3 Overall, Sudan accounts for 21.3% of adults and children living with HIV in the MENA region and this makes it the second worst-affected country in the region. The burden of hepatitis B in the general Sudanese population is estimated to be more than 8%, making it the worst-affected country in the Arab world. 4 Despite earlier reports indicating endemicity of syphilis and yaws in Sudan, 5 no accurate data currently exist on their burden in the general population. Of note, the prevalence of syphilis in the MENA region in selected demographic groups has been estimated to be 0–3% in blood donors and 0–19% in ANC attendees. 6
North Kordofan state is situated in western Sudan and has been affected by a large-scale conflict-induced population displacement from neighbouring South Kordofan and Darfur regions. 7 In this study, we sought to determine the seroprevalence of HIV, hepatitis B, and syphilis among pregnant women attending routine ANC in a major maternity hospital in North Kordofan and explore potential risk factors that might be associated with these infections. We hypothesised that the prevalence of maternal HIV, hepatitis B and syphilis would be high.
Methods
Setting
El Obeid is the capital city of North Kordofan state and its maternity teaching hospital is by far the largest centre for antenatal and postnatal services in North Kordofan. According to the 2008 population census, women of child-bearing age (15–44 years) accounted for 22.4% (653,900/2,920,992) of the population living in North Kordofan State. 8
Objectives
We sought to determine the seroprevalence of HIV, hepatitis B and syphilis among pregnant women attending ANC at El Obeid Maternity Hospital in North Kordofan and explore their potential association with a predefined set of socio-demographic and maternal risk factors.
Study design
A cross-sectional study design using unlinked anonymous testing (UAT) strategy for HIV, hepatitis B and syphilis was implemented. 9 In the period from 1 August 2016 to 1 March 2017, consecutive residues of routinely collected antenatal blood samples were aliquoted into new tubes and anonymised using unique numerical codes. A limited set of socio-demographic and maternal information (age, stage of pregnancy, gravidity, parity, previous mode of delivery, history of blood transfusion, and husband polygamy) was abstracted from ANC cards onto numerically-coded data collections forms that were devoid of any personal identifiers. Irrevocably-unlinked data collection forms and anonymised blood samples were then matched by their unique numerical codes and analysed. Results were recorded in a laboratory ledger but none of these test results could be traced back to any pregnant woman.
To ensure that each pregnant woman contributed a single blood sample to the study irrespective of the number of ANC visits, ANC cards were colour coded with a felt-tip pen to indicate participation in the study and to preclude any further collection of blood residues or data.
Diagnostic methods
Rapid commercial test kits were used according to their manufacturers’ instructions to determine the presence of hepatitis B surface antigen (HBsAg), HIV-1/2 antibodies, and Treponema pallidum antibodies.
The OnSite™ HBsAg Combo Rapid Test (CTK Biotech, San Diego, CA, USA), a lateral flow chromatographic immunoassay, was used to screen for HBsAg. Reactive specimens were confirmed using the Elecsys® HBsAg II assay (Elecsys 2010, Roche Diagnostics GmbH, Mannheim, Germany).
Due to logistical supply problems affecting kits' availability, several rapid immunochromatographic test kits were used to screen for the presence of total antibodies to HIV-1/2. These were Alere Determine™ HIV–1/2 (Alere, Galway, Ireland), OnSite™ HIV 1/2 Ab Plus Combo Rapid Test (CTK Biotech, San Diego, CA, USA), INSTI™ HIV–1/HIV–2 Antibody Test (BioLytical Laboratories Inc., Richmond, Canada), and Uni-Gold™ HIV Rapid Test (Trinity Biotech, Bray, Ireland). The Elecsys® HIV combi PT assay (Elecsys 2010, Roche Diagnostics GmbH, Mannheim, Germany) was used to confirm reactive specimens by detecting total antibodies to HIV-1/2 and/or p24 antigen.
In accordance with the World Health Organization’s recommendations for resource-poor settings, a single-test strategy for syphilis testing was adopted. 10 Depending on local availability, detection of T. pallidum antibodies was performed by using either of three rapid lateral flow devices: ABON™ Syphilis Ultra Rapid Test (Inverness Medical Innovations Hong Kong Ltd, Hangzhou, China), BioTracer™ Syphilis rapid test (NanoEnTek Inc., Seoul, Korea), or Healgen Syphilis Rapid Test (Healgen Scientific LLC, Bellaire, TX, USA).
Statistical analysis
The prevalence of HIV, hepatitis B and syphilis was estimated by the proportion of pregnant women whose residual blood samples were positive for HIV-1/2 antibodies, HBsAg or T. pallidum antibody, respectively, and was calculated with 95% exact binomial two-sided confidence intervals (CIs).
Sample size calculation focused on estimating HIV prevalence because it was anticipated to have far lower prevalence than hepatitis B and syphilis. Although HIV prevalence among Sudanese women aged 15–49 years had been reported to be 0.2%, 11 we believed this was an underestimate of the true prevalence because most neighbouring countries had higher prevalence estimates. For example, the reported HIV prevalence in women aged 15–49 years was 3.2% in South Sudan, 1.6% in Chad, 4.7% in Central African Republic, 1.3% in Ethiopia, and 0.8% in Eritrea. 11 We calculated that a sample size of 440 pregnant women would be required to provide 90% power for the two-sided 95% CI for an HIV prevalence of 0.2% to be excluded if the true prevalence was 1.5%. The power would be 80% if the true prevalence was 1.25%.
The median and interquartile range (IQR) were used to summarise continuous variables whereas frequencies and percentages were used to summarise categorical variables. Depending on the number of prevalent cases, logistic regression would be considered to explore the association between HIV, hepatitis B, syphilis, or a composite outcome including any of the three infections and a predefined set of socio-demographic and maternal characteristics. All tests were two-sided and p-value <0.05 was considered statistically significant with no adjustment for multiple testing. Statistical analyses were performed using Stata 14.2 (StataCorp, TX, USA).
Ethics statement
The study received the approval of the Ethics Committee of the University of Kordofan (reference no. I/A/7).
Results
A total of 444 residual blood samples were collected and serologically tested for HIV, hepatitis B and syphilis. The median age of pregnant women was 26 years (IQR 21–30). Multigravidae accounted for 77.48% (344/444). Information on the current stage of pregnancy was available on 422 women: 15.64% (66/422) were in their first trimester, 22.99% (97/422) in their second trimester, and 61.37% (259/422) in their third trimester. Information on parity was available for 343 women: 76.38% (262/343) had 1–4 previous deliveries whereas 23.62% (81/343) had ≥5 deliveries. Previous modes of delivery for pregnant women included normal vaginal delivery in 72.51% (248/342), instrumental vaginal delivery in 0.58% (2/342), and caesarean section in 33.92% (116/342). History of blood transfusion was reported by 8.82% (39/442) of pregnant women whereas polygamous activity of husbands, defined as having >1 wife, was reported by 14.93% (66/442).
Table 1 summarises the baseline characteristics of pregnant women and their corresponding outcomes of serological testing for HIV, hepatitis B and syphilis. HIV-1/2 antibodies were detected in 1.13% (5/444; 95% CI 0.37–2.61%), HBsAg was detected in 2.93% (13/444; 95% CI 1.57–4.95%) and syphilis total antibodies were detected in 7.43% (33/444; 95% CI 5.17–10.28%).
Baseline characteristics of pregnant women undergoing anonymous unlinked testing for the human immunodeficiency virus (HIV), hepatitis B, and syphilis, El Obeid Maternity Hospital, North Kordofan state, Sudan (August 2016–March 2017).
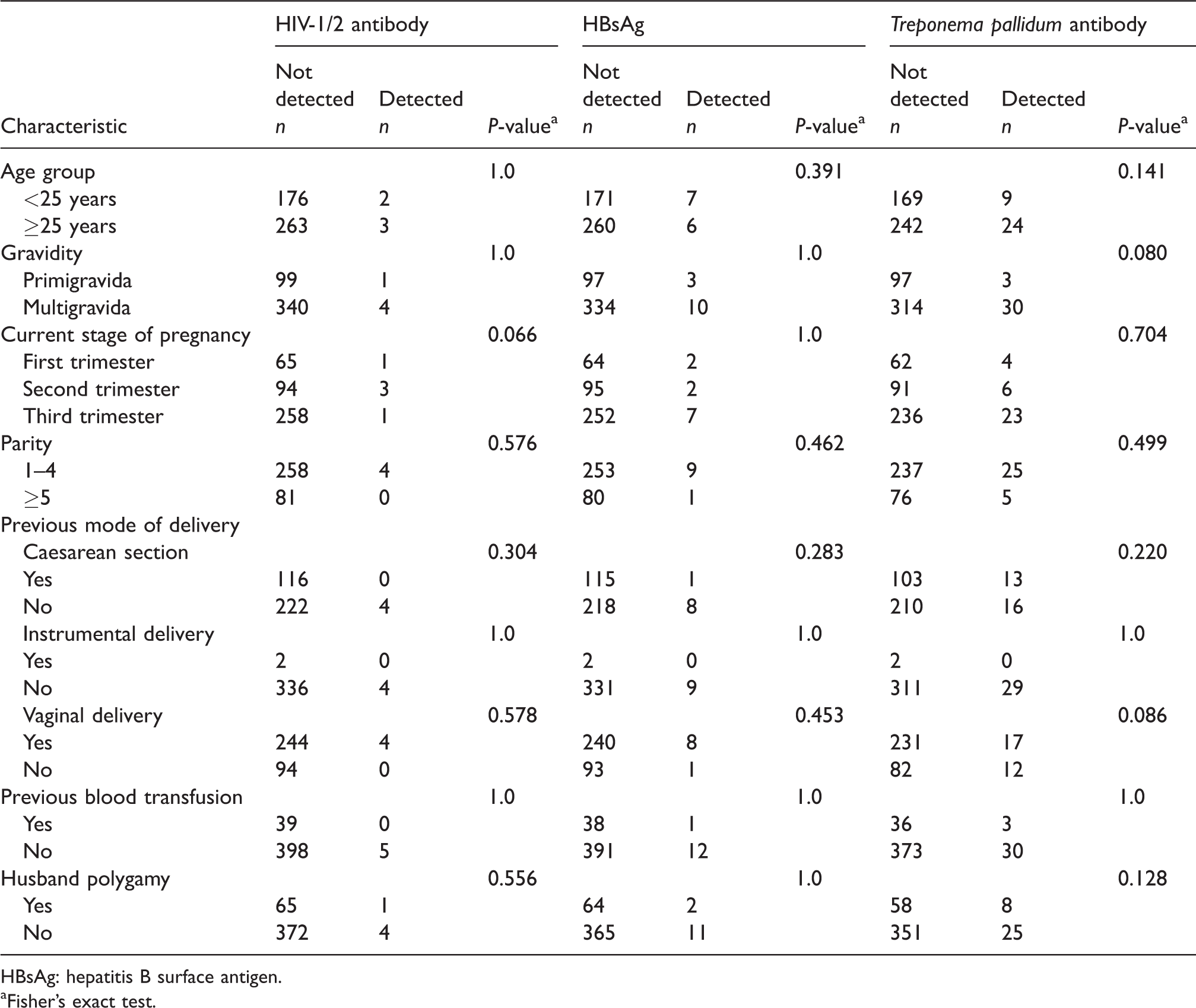
HBsAg: hepatitis B surface antigen.
aFisher’s exact test.
As only five prevalent HIV cases were detected in this study, bivariate analyses were restricted to assessing the association between hepatitis B, syphilis, or a composite outcome including any of the three infections and a predefined set of socio-demographic and maternal factors. No statistically significant associations were found on bivariate analyses between hepatitis B, syphilis, or a composite outcome including any of the three infections and age, stage of pregnancy, gravidity, parity, previous mode of delivery, history of blood transfusion, or husband polygamy (Table 2).
Risk factors for hepatitis B, syphilis, and a composite outcome including any infection with hepatitis B, syphilis, or the human immunodeficiency virus (HIV).
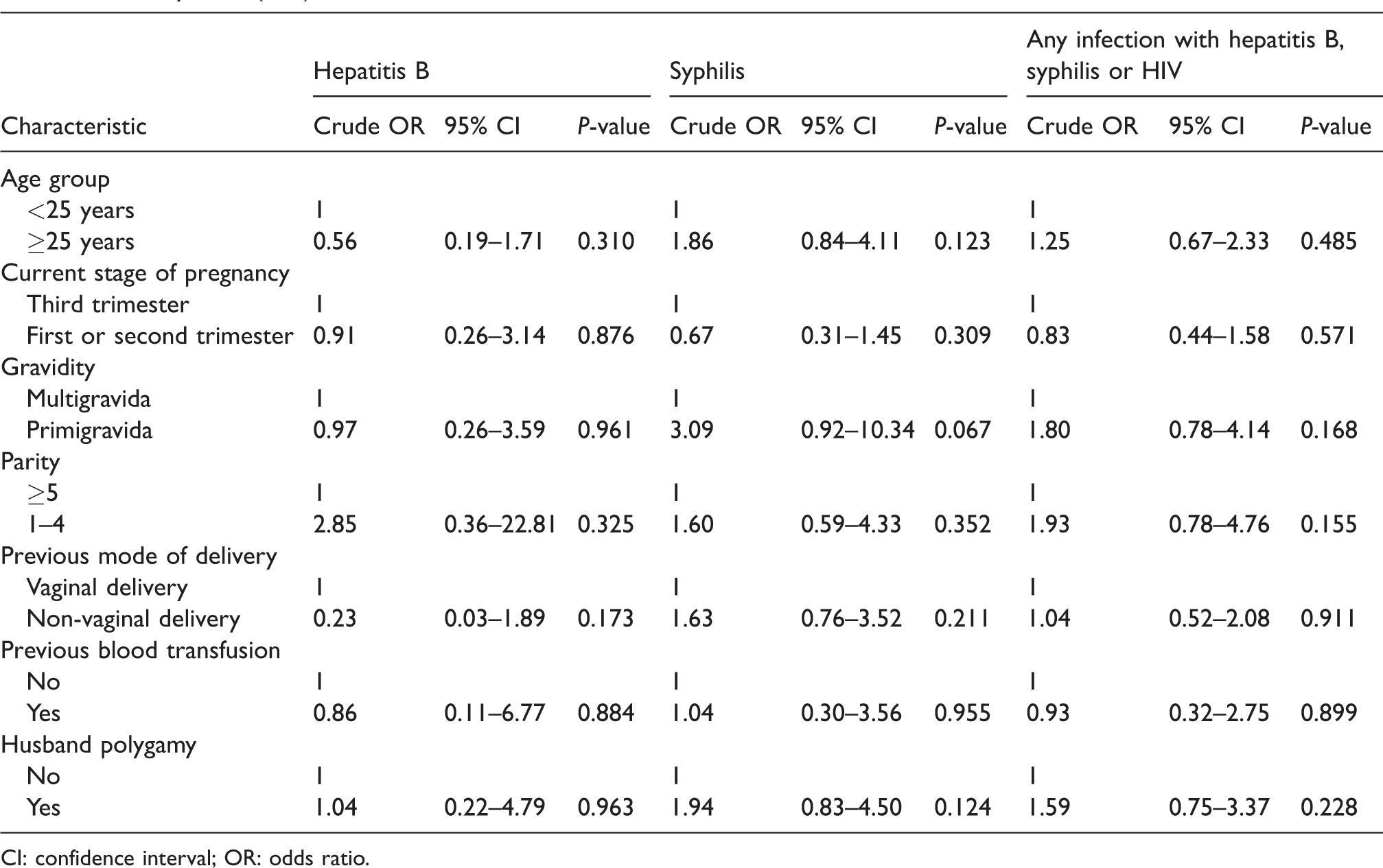
CI: confidence interval; OR: odds ratio.
Discussion
This study provides additional data that can help inform local health policymaking on universal antenatal screening for infectious diseases in North Kordofan, Sudan. Our results indicated a significant prevalence of maternal syphilis, hepatitis B and HIV infections. We did not find any statistically significant associations between HIV, hepatitis B, or syphilis and any of the potential maternal or socio-demographic risk factors examined in this study.
Mohammed et al. 12 used an UAT strategy in 430 pregnant women in eastern Sudan and reported a low HIV prevalence of 0.23% (95% CI 0.01–1.29%). In contrast, Gassmelseed et al. 13 offered provider-initiated HIV testing to 1138 pregnant women in central Sudan and reported a refusal rate of 73% (833/1138) and an HIV prevalence rate of 0.98% (3/305) (95% CI 0.20–2.85%) amongst those who agreed to be tested. Ortashi et al. 14 2004 did not detect any HIV infections in 151 pregnant women in central Sudan but reported prevalence rates of 19.9% for Chlamydia trachomatis, 7.3% for syphilis, 7.3% for Trichomonas vaginalis, 2% for Neisseria gonorrhoeae, and 7.3% for having multiple STIs during pregnancy. A more recent study on 406 out of 1400 pregnant women of low socio-economic status attending ANC in a women’s prison, displaced camps, and several primary care centres in central Sudan did not find any cases of HIV or gonorrhoea but reported prevalence rates of 7.8% for T. vaginalis, 4.9% for C. trachomatis, and 5% for syphilis. 15 However, the risk of selection bias in that study cannot be ignored as 7.1% of pregnant women refused blood sampling for HIV and syphilis testing, 13.8% refused cervical swabbing for gonorrhoea and Chlamydia testing, and 11.6% refused vaginal swabbing for trichomoniasis testing.
Results of the 2009 national ANC sentinel survey, which used UAT and covered all the 15 northern states of pre-secession Sudan, indicated a seroprevalence of 0.16% for HIV and 1.31% for syphilis. 16 Specific data on North Kordofan state indicated maternal prevalence rates of 0% for HIV and 2.58% for syphilis. At 6.28% prevalence, the neighbouring South Kordofan state was found to have the highest burden of maternal syphilis in Sudan in 2009. Furthermore, data on pregnant women living in internally displaced people camps in West Darfur state (western Sudan) in 2007 indicated an HIV prevalence of 0.27%. 17 Of note, the states of Darfur and South Kordofan have witnessed waves of sexual violence against women during the recent civil strife in these regions. 7
The Sudan household survey (2010) showed that only 1% of women and men aged 15–49 years were tested and informed of their HIV test result in the 12 months prior to the survey. 17 Data from the integrated bio-behavioural survey among key populations (2011), the ANC surveillance rounds (2010), and routine reports from voluntary counselling and testing as well as prevention of mother-to-child transmission centres indicated a concentrated HIV and STIs epidemic among female sex workers and men who have sex with men and showed geographical clustering of HIV in eastern and south eastern regions of Sudan.17,18 However, the present study from western Sudan casts doubt on these findings as our recorded maternal HIV prevalence has exceeded the 1% threshold, which if consistently reproduced by other studies would be indicative of a generalised epidemic. 19 An earlier study from central Sudan reported a worryingly high HIV prevalence of 5.7% among hospitalised sick children aged 1.5–14 years and called for more studies to determine the true prevalence of paediatric and maternal HIV. 20
Management of HIV during pregnancy remains unsatisfactory in Sudan. In 2013, the UNAIDS estimated the number of pregnant women living with HIV in Sudan to be 2500 (1600–3500). 3 However, only 74 pregnant women had access to antiretroviral therapy (ART) giving rise to an estimated coverage of 3% (2–5%). Similarly, it is estimated that 1000 new HIV infections occurred in children aged 0–14 years in the period from 2009 to 2013 but only 5% of them had access to ART and none of them had HIV viral load measurements.3,17
There is dearth of information on the current burden of maternal hepatitis B in Sudan. A previous study conducted in the 1980s in central Sudan found that 70% of HBsAg-positive women of child-bearing age were e antigen-positive, which is a marker for high infectivity. 21 More recently, Elsheikh et al. 22 and Abuelgasim and Baraka 23 reported HBsAg seroprevalence rates of 5.6 and 7.5%, respectively, among pregnant women in central Sudan. Furthermore, a small prospective study conducted in central Sudan on acute hepatitis in pregnancy showed that hepatitis B accounted for a third of cases and that it led to poor maternal and foetal outcomes. 24 These findings, coupled with the potential impact of the now established routine childhood immunisation against hepatitis B, warrant further research into the current epidemiology of maternal hepatitis B in various regions of Sudan.
Although the coverage for the third dose of routine childhood hepatitis B immunisation in Sudan has been consistently above 90% over the past few years, no data exist on its coverage at birth – a key intervention to reduce vertical transmission. 25 Of note, hepatitis B immunoglobulin is not readily available in Sudan due to the prohibitive cost as well as various supply chain and storage problems.
Our use of an UAT strategy, which complied with the ethical and legal framework required for such studies,9,26 enabled us to obtain unbiased estimates of the maternal prevalence of HIV, hepatitis B, and syphilis. Although we managed to collect information on a set of maternal and socio-demographic variables, we were not able to complement this with potentially useful behavioural and clinical information or test for additional STIs due to study design limitations.
In this study, the cross-reactivity between venereal and non-venereal treponemal antibodies in endemic settings might have overestimated our reported syphilis seroprevalence. Further testing on HBsAg-positive blood samples to check for hepatitis D co-infection was not performed due to logistical constraints. Similarly, we did not test for other hepatitis B serological markers to find out whether hepatitis B infection was recent or chronic.
We relied solely on the combined detection of HIV-1/2 antibodies for HIV screening and, therefore, we might have missed pregnant women passing through a seroconversion window. HIV typing was not performed because of resource constraints. Although several commercial diagnostic assays were used in our study to determine HIV and syphilis serostatus, we do not believe these have adversely affected the validity of our results as all these assays conform to international regulatory requirements and have similar and excellent performance characteristics. The small number of prevalent HIV cases in this study meant that the power would be too small to provide informative assessment on the association between HIV and our predefined maternal and socio-demographic factors.
Previously published studies from Sudan on HIV, hepatitis B and syphilis used different methods for patient recruitment and followed different diagnostic procedures.12–15,21–24 Such inconsistencies made it difficult to compare reported outcomes, e.g. prevalence rates. Furthermore, no deeper insights were gained into the socio-behavioural determinants of these infections due to the lack of complementary qualitative data.
Our study raises concern over the burden of HIV, hepatitis B and syphilis among pregnant women in North Kordofan and calls for immediate corrective action to educate the public and to bolster the existing healthcare system. Our findings reiterate the need for further research to accurately estimate the burden of maternal HIV, hepatitis B, and syphilis and to explore the socio-demographic and behavioural determinants of these infections as well as their clinical outcomes. We look forward to the day in which pregnant women in North Kordofan are offered universal antenatal screening and treatment for STIs to protect them, their partners, and offspring.
Footnotes
Authors’ contributions
EAMH, AAAE, and FEA conceived the study. SME, SKE, and MAB collected the data and supervised laboratory testing. AGB and ZOEB analysed and interpreted the data. ZOEB wrote the draft manuscript. All authors critically reviewed and approved the final version of the manuscript.
Acknowledgements
We would like to extend our thanks to the laboratory and clinical staff at El Obeid maternity teaching hospital.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The University of Kordofan provided funds to purchase commercial rapid test kits for the diagnosis of HIV, hepatitis B, and syphilis. AGB was supported by the Medical Research Council (MRC_UU_12023/23).