
Abstract
The association between single nucleotide polymorphisms of genes encoding transport proteins involved in the bio-disposition of tenofovir disoproxil fumarate (TDF) and kidney tubular dysfunction (KTD) in HIV-positive patients was examined in this study. Fifty-eight patients who received TDF were screened for KTD using retinol-binding protein (RBP) concentration in urine. We defined KTD as the top quartile of urinary RBP/creatinine ratio (>17 μg/mmol), regardless of estimated glomerular filtration rate (eGFR) or proteinuria. Genotyping of genes encoding transport proteins involved in the disposition of TDF was undertaken using validated Taqman 5′ nuclease assays. Patients with KTD (N = 15) had higher current CD4 cell counts, lower eGFR and were less likely to possess the genotype CC at position 24 of the ABBC2 (MRP2, rs717620) gene. In multivariate analysis, genotype CC at position 24 of the ABBC2 gene was significantly associated with KTD (odds ratio =0.05, 95% confidence interval = 0.003–0.7, P = 0.027). Genotype CC at position 24 of the ABBC2 (MRP2 rs717620) gene was significantly associated with a reduced risk of elevated urinary RBP in HIV-positive patients exposed to TDF.
Background
Since the advent of antiretroviral therapy (ART), there has been a substantial reduction in morbidity and mortality due to HIV infection. 1 While numerous studies have confirmed the efficacy and safety of ART, concern remains about potential toxicity of a number of currently used drugs, including the effects of tenofovir disoproxil fumarate (TDF) on the kidney.2–5 However, the exact phenotype (clinical and laboratory) as well as genetic and non-genetic determinants of TDF-induced kidney injury in HIV-positive patients has remained a matter of debate. 2 Single nucleotide polymorphisms (SNPs) of genes encoding transport proteins involved in the disposition of tenofovir such as ABCC2 (MRP2; rs717620),6–8 ABCC4 4976 (rs1059751), 9 and ABCC10 (MRP7; rs2125739, rs9349256) 10 have recently been associated with kidney tubular dysfunction (KTD) in HIV-positive patients exposed to TDF. While KTD is emerging as one of the clinical phenotypes from recent reports,6,7 various criteria have been applied to define it. In these studies, KTD has been defined by a composite of urinary and serum parameters which highlights the variable clinical phenotype and which may preclude its easy applicability in clinical practice. Conversely, there has been increasing interest in the potential utility of low-molecular weight proteinuria (LMWP) as a more reliable and early marker of kidney tubular injury. These markers include kidney injury molecule 1 (KIM-1), retinol-binding protein (RBP), neutrophil gelatinase-associated lipocali (NGAL), and L-type fatty acid-binding protein amongst others.11–16 RBP is a low-molecular weight (LMW) protein that is excreted in increased amounts in patients with KTD. 15 In a large clinical trial, patients randomised to TDF experienced significant increases in urinary RBP excretion. 14 In a recent cross-sectional study, patients exposed to TDF (when administered with a ritonavir-boosted protease inhibitor) were more likely to have substantially elevated urinary RBP concentrations. 15 Whether KTD, as defined by LMWP, correlates with SNPs of genes encoding transporter proteins involved in the disposition of TDF is unknown. We examined such an association for previously reported SNPs in the ABCC2 (MRP2), ABCC4 (MRP4), ABCC10 (MRP7), SLC22A6 (OAT1), and SLC22A11 (OAT4) genes.
Patients and methods
Study population
The demographic features of the study population have been described previously. 15 Briefly, HIV-positive patients attending King’s College Hospital, London, United Kingdom, were invited to participate in a cross-sectional study to examine the prevalence of kidney disease and its associated factors. Clinical information was obtained, as well as blood and urine samples collected and stored at −70°C until use. RBP was quantified by enzyme-linked immunosorbent assay (ELISA; Immundiagnostik, Bensheim, Germany; reference range 0.01–0.54 mg/l) and expressed as ratio to creatinine concentration (RBPCR). KTD was defined by an RBPCR value in the top quartile (>17 µg/mmol), regardless of estimated glomerular filtration or proteinuria. The study was reviewed and approved by the NHS research ethics committee.
Selection of SNPs and genotyping
Seven SNPs were selected for mutational screening of genes encoding transport proteins involved in the disposition of TDF. All seven SNPs selected in this study have previously been associated or tested for their association with KTD. Evaluated SNPs include ABCC2 (MRP2; rs717620), ABCC4 3463 (MRP4; rs1751034), ABCC4 669 (MRP4; rs899494), SLC22A11 (OAT4; rs11231809), SLC22A6 (OAT1; close to accession number AJ249369), ABCC10 (MRP7; rs9349256, rs2125739). Genomic DNA was extracted from stored serum samples using the QIAamp DNA extraction kit (QIAGEN GmbH.Hilden. Germany). Mutational screening and genotyping were carried out by allelic discrimination with made-to-order primers and probes using Taqman 5′ nuclease genotyping assays with standard protocol (TaqMan SNP Genotyping Assays; Applied Biosystems, 850 Lincoln Centre Drive, Foster City, California 94404, USA).
Statistical analysis
Genotypic frequencies in the study population were compared by Fisher’s exact test. All SNPs were tested for deviation from the Hardy-Weinberg equilibrium (HWE) by Chi square test using Haploview software (Broad Institute, Cambridge, MA, USA). Both bivariate and multivariate analyses were carried out to identify predictor variables. Co-variates with P < 0.1 in univariate analysis were entered into multivariate logistic regression models. P values <0.05 were considered statistically significant. All other data analyses were carried out using StatsDirect version 2.7.9 (StatsDirect Ltd, Altrincham, Cheshire, UK).
Results
Patient characteristics
Eighty-one of the 317 patients in the cross-sectional cohort received TDF at the time of sampling. Of these, 23 had missing RBPCR values and were not included in analyses. Of the remaining 58, 15 (25.9%) had KTD, while the remaining 43 (74.1%) patients served as controls. The median duration of TDF exposure was 583 (IQR: 195, 1035) days. Patients with KTD had higher current CD4 cell counts, lower estimated glomerular filtration rates (eGFRs) and higher albumin to creatinine ratios (Table 1).
Characteristics of the study population (N = 58).
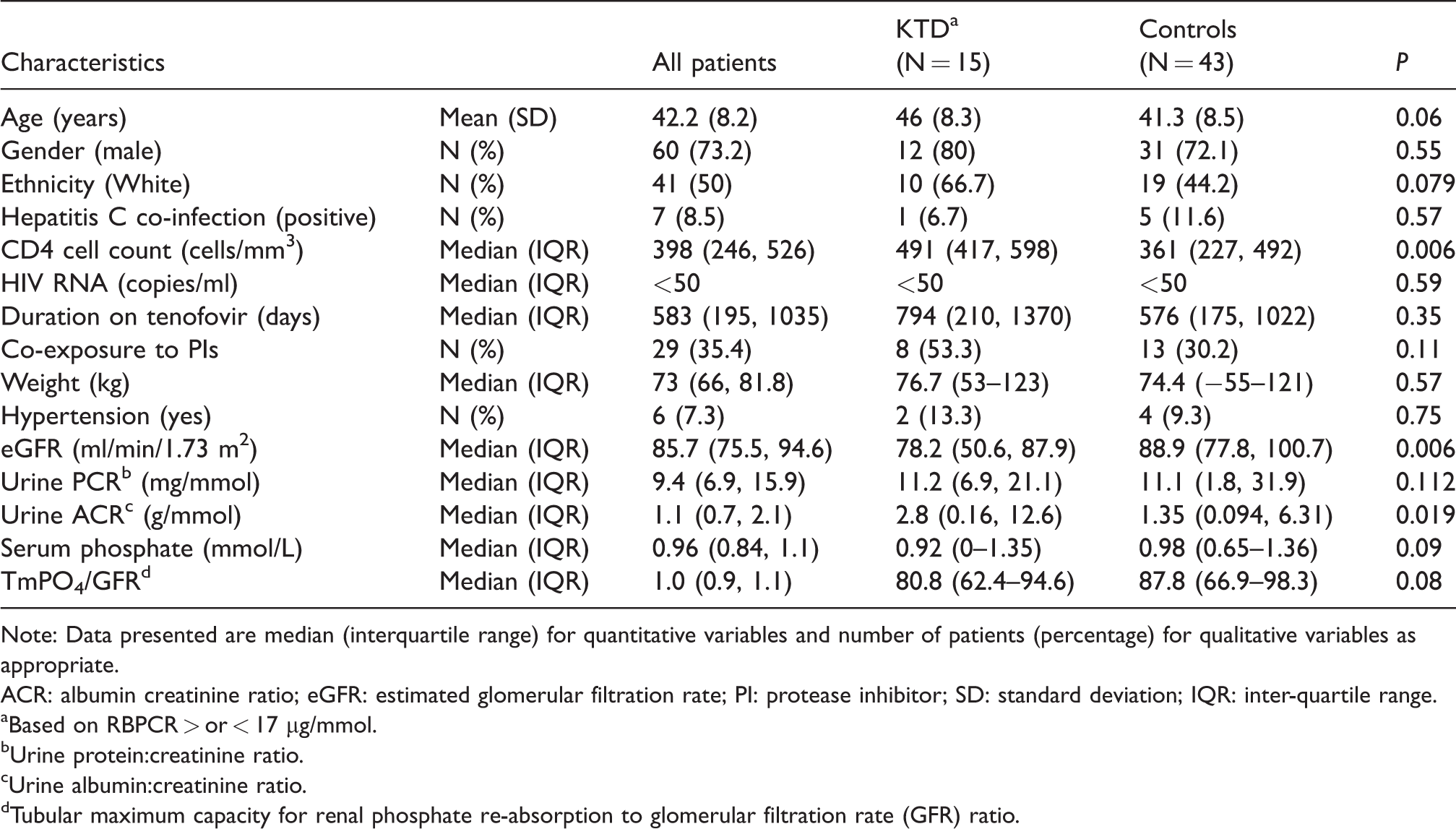
Note: Data presented are median (interquartile range) for quantitative variables and number of patients (percentage) for qualitative variables as appropriate.
ACR: albumin creatinine ratio; eGFR: estimated glomerular filtration rate; PI: protease inhibitor; SD: standard deviation; IQR: inter-quartile range.
Based on RBPCR > or < 17 µg/mmol.
Urine protein:creatinine ratio.
Urine albumin:creatinine ratio.
Tubular maximum capacity for renal phosphate re-absorption to glomerular filtration rate (GFR) ratio.
Association of KTD and SNPs of tenofovir transporter genes
The distributions of genotypes of the studied SNPs are shown in Table 2. There was a lower expression of the genotype CC at position 24 of the ABBC2 (MRP2, rs717620) gene in patients with KTD compared with CT and TT genotypes (odds ratio [OR] 0.29; 95% confidence interval [CI] 0.08–0.96, P = 0.04).
Allelic frequencies in HIV-positive patients exposed to tenofovir with and without KTD.
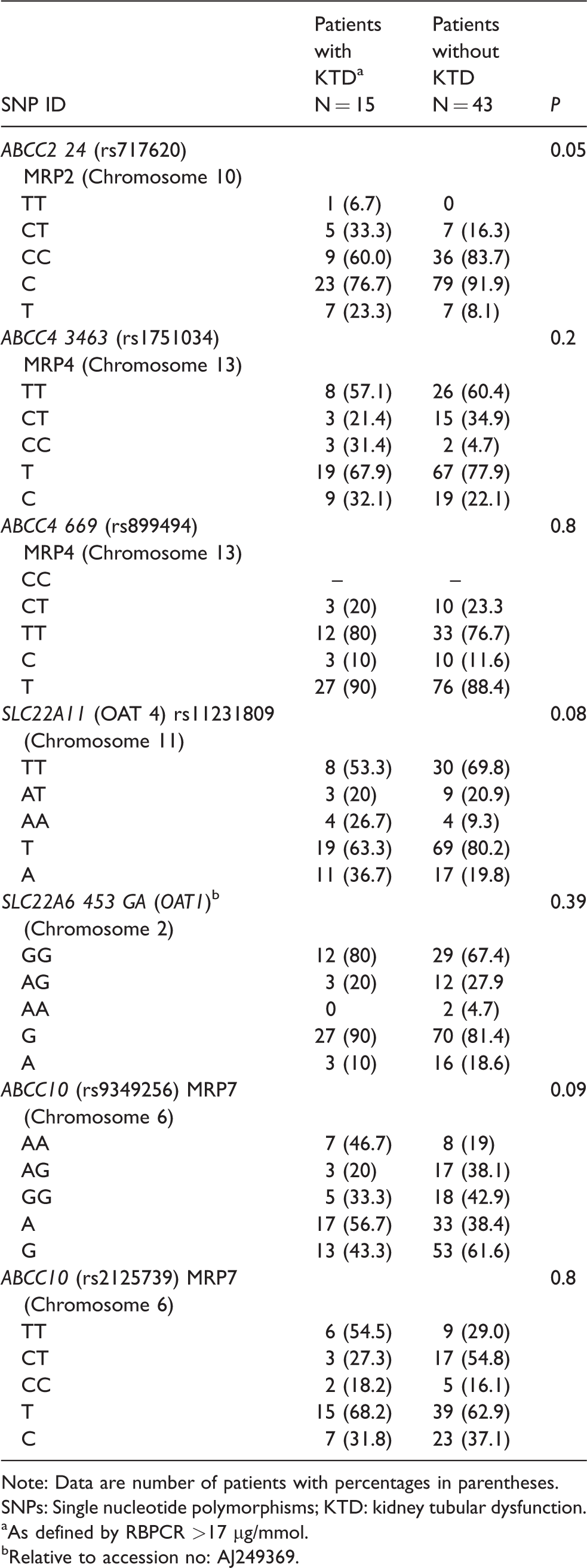
Note: Data are number of patients with percentages in parentheses.
SNPs: Single nucleotide polymorphisms; KTD: kidney tubular dysfunction.
As defined by RBPCR >17 µg/mmol.
Relative to accession no: AJ249369.
Independent predictors of KTD
Table 3 shows factors associated with KTD in HIV-positive patients exposed to TDF. Univariate odds ratios were calculated for each of the SNPs of interest. Possession of the CC genotype at position 24 of the ABCC2 gene (MRP2, rs717620) was the only SNP significantly associated with KTD. This SNP remained significantly associated with KTD after adjustment for age and eGFR (adjusted OR= 0.05; 0.003–0.71, P = 0.027).
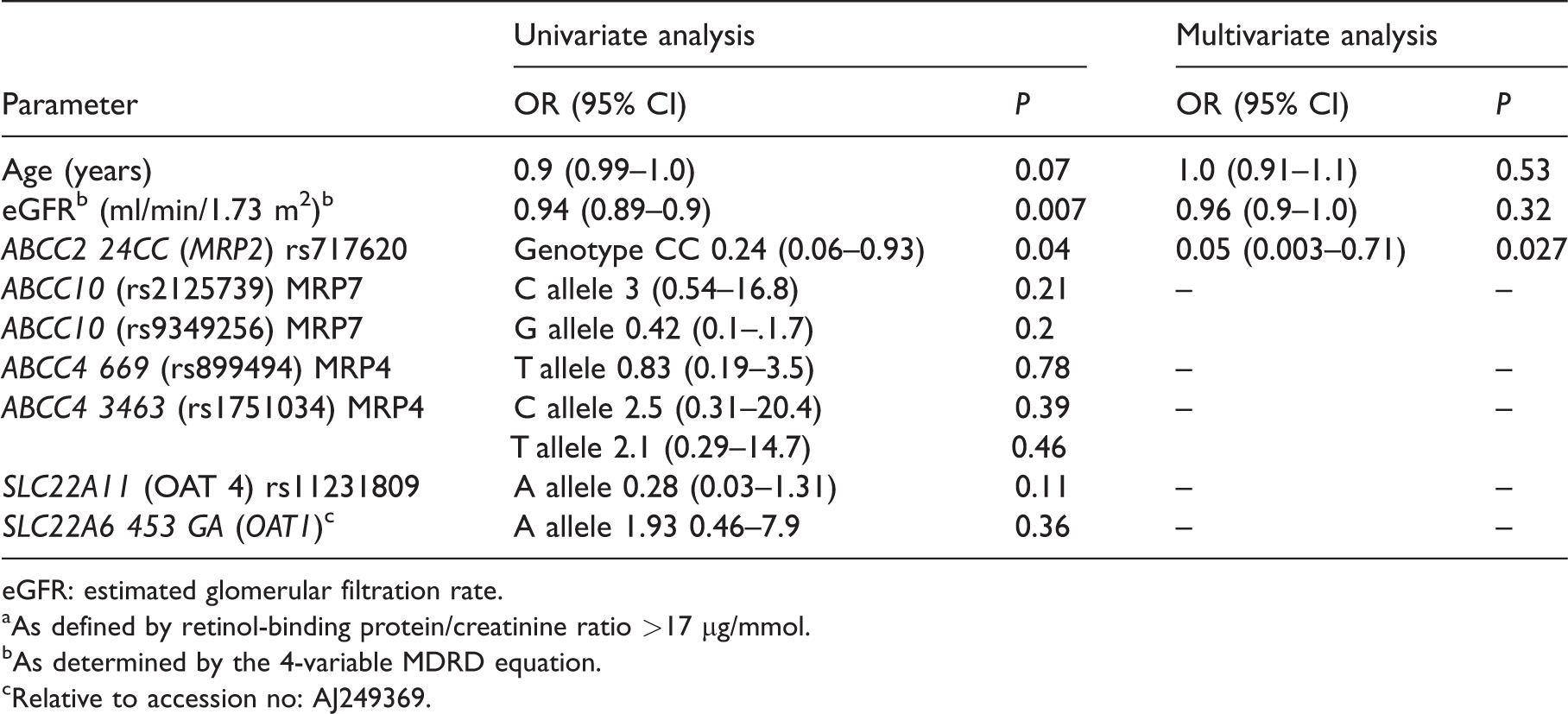
eGFR: estimated glomerular filtration rate.
As defined by retinol-binding protein/creatinine ratio >17 µg/mmol.
As determined by the 4-variable MDRD equation.
Relative to accession no: AJ249369.
Haplotype analyses
We carried out exploratory haplotype analyses of the ABCC2-ABCC4 SNPs; no significant association with KTD was observed.
Discussion
A number of genes encoding transport proteins involved in the disposition of TDF have been known to be polymorphic.6,7,10 This is the first study exploring the potential relationship between SNPs of genes encoding transport proteins involved in the biodisposition of TDF and risk of kidney tubular injury in HIV-infected patients as defined by LMWP (RBPCR). Since its approval in 2001, TDF has found extensive use across a broad range of HIV and hepatitis B patient cohorts, with its efficacy and safety well established by a number of studies.14,17 Nonetheless, a small proportion of patients develop severe renal tubular toxicity (Fanconi syndrome), and about 6–22% of patients reportedly have subclinical KTD.18–20 Previous studies have suggested possession of genotype CC at position 24 of the ABCC2 (MRP2, rs717620) gene,6–8 ABCC10 (MRP7, rs9349256 and rs2125739) 10 including the extended haplotype ABCC10-ABCC2 (GGC-CGTC) 10 in addition to age, and low body weight as potential determinants of KTD in HIV-positive patients exposed to TDF. In these studies, KTD was defined by a composite of serum and urinary parameters, based around estimated glomerular filtration rate, and tubular proteinuria. Another recent study carried out exclusively in a prospective Japanese cohort of HIV-positive patients failed to establish any association between the ABCC2 24CC (rs717620) SNP and risk of KTD. It is noteworthy that this study utilised eGFR (<60 ml/min/1.73 m2) as a diagnostic marker for kidney dysfunction. 21
In contrast, we observed that subjects with elevated urinary RBP were less likely to carry ABCC2 24CC. A number of factors could have accounted for this discrepancy, including the limited size of our study. Most importantly, KTD has previously been defined using different surrogate markers of tubular injury, whereas we elected to utilize urinary RBP ratio (which has potential benefits as a putative tubular biomarker). How the mode of characterisation of KTD explains the difference in outcome between our report and previous studies is uncertain. Mechanistic studies22–24 have established MRP4 (ABCC4) and MRP7 (ABCC10) 10 but not MRP2 (ABCC2) as efflux transporters of TDF. However, previous pharmacogenetic studies including ours have observed associations between ABCC2 (MRP2, rs717620) and not ABBC4 (MRP4) genotypes and KTD in TDF-exposed patients. Suggested explanations for this paradox include the fact that ABCC2 (MRP2) may be in linkage disequilibrium with ABCC4 (MRP4); 7 possession of the ABBC2 24 CC (MRP2) genotype may lead to less efficient tenofovir excretion from tubular cells 7 with the potential for TFV accumulation within kidney tubular cells; possession of ABCC2 24 CC (rs717620) genotype may influence the transport of a yet to be identified factor that impacts on TDF-induced KTD. 7
Recently, Likanonsakul et al. reporting in an exclusive cohort of Thai patients showed significant association between possession of the C allele of the ABCC4 T4976C (rs1059751) SNP and risk of KTD. The novelty of this report includes its utility of a threshold of β-2 microglobulin as a diagnostic marker of KTD, and in classification of patient cohorts into cases and controls. Additionally, this represents the only report to date to demonstrate any significant association between ABCC4 T4976C (rs1059751) SNP and risk of KTD in HIV-positive patients exposed to TDF. 9
Kidney tubular dysfunction comprises a spectrum with Fanconi syndrome representing the most extreme phenotype and its definition to date has relied on a composite of several urine and serum parameters. 7 The use of RBP as a single diagnostic marker may provide a convenient mode of assessing KTD in clinical practice, 14 but this will need exploration by future prospective studies.
As has been the case with recent pharmacogenetic reports, although our study showed significant correlation between other evaluated SNPs of TFV transport proteins and markers of kidney function in this population, we had limited power to demonstrate an independent association with KTD. Additionally, our study is limited by lack of comparison between traditional composite urinary and serum markers of KTD and LMWP in adjudication of our cases and control. Incorporating this in the design of future prospective studies will improve case ascertainment. The quality of DNA extracted from serum rather than whole blood may have affected potential associations between the evaluated SNPs and LMWP. However, there were standard protocols provided by the made-to-order genotyping assay manufacturers with in-built quality control standards, which we strictly adhered to in the course of DNA processing. Owing to these limitations, there will be need for further prospective work in this area to ascertain the exact relationship between these LMWP and KTD, as well as any clinically relevant association with SNPs encoding TFV transporters.
Conclusion
In conclusion, we have demonstrated that possession of genotype CC at position 24 of the ABCC2 (MRP2 rs717620) gene was significantly negatively associated with the risk of elevated urinary RBP in HIV-positive patients exposed to TDF.
Footnotes
Acknowledgements
We are grateful to the staff and HIV patients of Kings College Hospital London for providing samples for this study. We also owe a debt of gratitude to Dr Sudeep Pushpakom, Professor Andrew Owen, and Dr Neil Liptrott with their assistance with DNA analysis.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Professor Khoo has received travel grants, honoraria and study grants from GSK, Roche, Tibotec, ViiV, Gilead, Merck, and Bristol-Myers Squibb.
Frank A Post has received funding to attend conferences or educational meetings, honoraria and/or research funding from Abbvie, Gilead Sciences, Bristol-Myers Squibb, Janssen-Cilag, GlaxoSmithKline/ViiV Healthcare and Merck.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received infrastructural support from the Liverpool Biomedical Centre for microbial diseases.