
Abstract
We report a case of reactive hemophagocytic syndrome (RHS) in the setting of acute human immunodeficiency virus type 1 infection (AHI). In addition, we review 11 previously reported cases of RHS precipitated by AHI and discuss strategies in the diagnosis and management of these overlapping clinical entities.
Introduction
Hemophagocytic syndrome (HPS) is a life-threatening condition caused by a disproportionate and dysregulated immune response. There are two major forms of HPS: the primary form, hereditary HPS, occurs in infancy and is caused by a variety of genetic abnormalities. The secondary form, reactive hemophagocytic syndrome (RHS), occurs at any age due to infections, malignancies, and rheumatologic conditions. Only a few case reports have detailed the development of RHS in the setting of acute human immunodeficiency virus type 1 infection (AHI). 1 We report one such case and review 11 similar cases reported in the literature.
Case report
A young man in his 20s was admitted with fever, altered mental status, and a diffuse maculopapular rash. Thirteen days earlier, he had been diagnosed with AHI after presenting with a nonspecific febrile illness, a positive HIV antigen/antibody assay, and a negative HIV-1/2 antibody differentiation assay. Since his fever initially resolved, the patient deferred initiation of antiretroviral therapy (ART) until after the results of a pending HIV-1 viral load. However, a few days later, his fever returned, and he became lethargic and developed mild disorientation (to date only), headache, nausea, vomiting, and a syncopal episode that prompted hospitalization. His vital signs were significant for a fever of 41°C and mild tachycardia. He appeared somnolent, tremulous, and had a diffuse, evanescent, erythematous maculopapular rash. Laboratory studies revealed a leukocyte count of 4000 per mcl, hematocrit of 24.9%, platelet count of 56,000 per mcl, aspartate aminotransferase (AST) of 598 IU/l, alanine aminotransferase of 302 IU/l, triglycerides of 559 mg/dl, ferritin of greater than 36,000 ng/ml, and fibrinogen of 271 mg/dl. CD4 cell count was 248 cells/mm3 (48%). HIV-1 viral load was 9.7 million copies per milliliter. Epstein–Barr virus-specific immunoglobulins and mild viremia of 592 copies per ml were consistent with previous infection. Serologic testing for atypical bacteria and opportunistic fungi was negative. Lumbar puncture revealed an elevated cerebrospinal fluid (CSF) protein (135 mg/dl) but no CSF pleocytosis or hypoglycorrhachia. CSF bacterial, fungal, and mycobacterial cultures; herpes and enterovirus virus polymerase chain reaction; West Nile Virus immunoglobulins; Venereal Disease Research Laboratory test; and cryptococcal antigen were negative (Table 1). Magnetic resonance imaging of the brain did not reveal any abnormalities. Computed tomography scan of the chest, abdomen, and pelvis revealed a spleen in the upper limits of normal in size, and prominent subcarinal, axillary, and mediastinal lymph nodes that did not meet radiologic size criteria for lymphadenopathy. The patient was started on dolutegravir and emtricitabine–tenofovir disoproxil fumarate. In addition, a bone marrow biopsy revealed histiocytosis and prominent hemophagocytosis (Figure 1). Due to the suspicion of RHS with neurologic involvement, the patient was started on systemic corticosteroids and etoposide, and intrathecal methotrexate one day after starting ART. The patient defervesced and returned to his baseline mental status by the time of discharge three days later. The patient remained on ART and his HIV-1 viral load became undetectable within four months. He completed treatment for presumed RHS without any adverse effects.
Timeline of diagnostic studies and therapies.
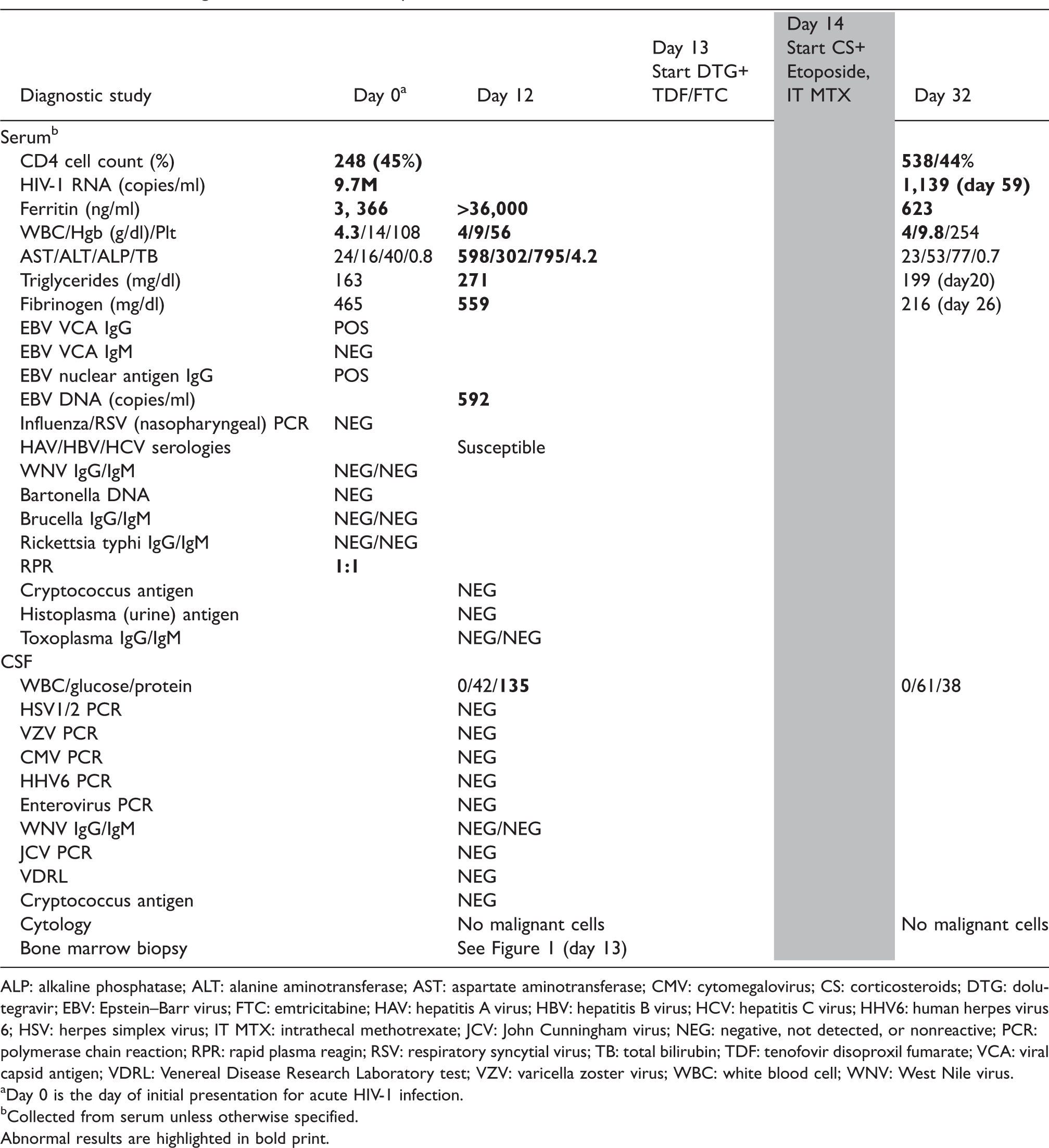
ALP: alkaline phosphatase; ALT: alanine aminotransferase; AST: aspartate aminotransferase; CMV: cytomegalovirus; CS: corticosteroids; DTG: dolutegravir; EBV: Epstein–Barr virus; FTC: emtricitabine; HAV: hepatitis A virus; HBV: hepatitis B virus; HCV: hepatitis C virus; HHV6: human herpes virus 6; HSV: herpes simplex virus; IT MTX: intrathecal methotrexate; JCV: John Cunningham virus; NEG: negative, not detected, or nonreactive; PCR: polymerase chain reaction; RPR: rapid plasma reagin; RSV: respiratory syncytial virus; TB: total bilirubin; TDF: tenofovir disoproxil fumarate; VCA: viral capsid antigen; VDRL: Venereal Disease Research Laboratory test; VZV: varicella zoster virus; WBC: white blood cell; WNV: West Nile virus.
aDay 0 is the day of initial presentation for acute HIV-1 infection.
bCollected from serum unless otherwise specified.
Abnormal results are highlighted in bold print.
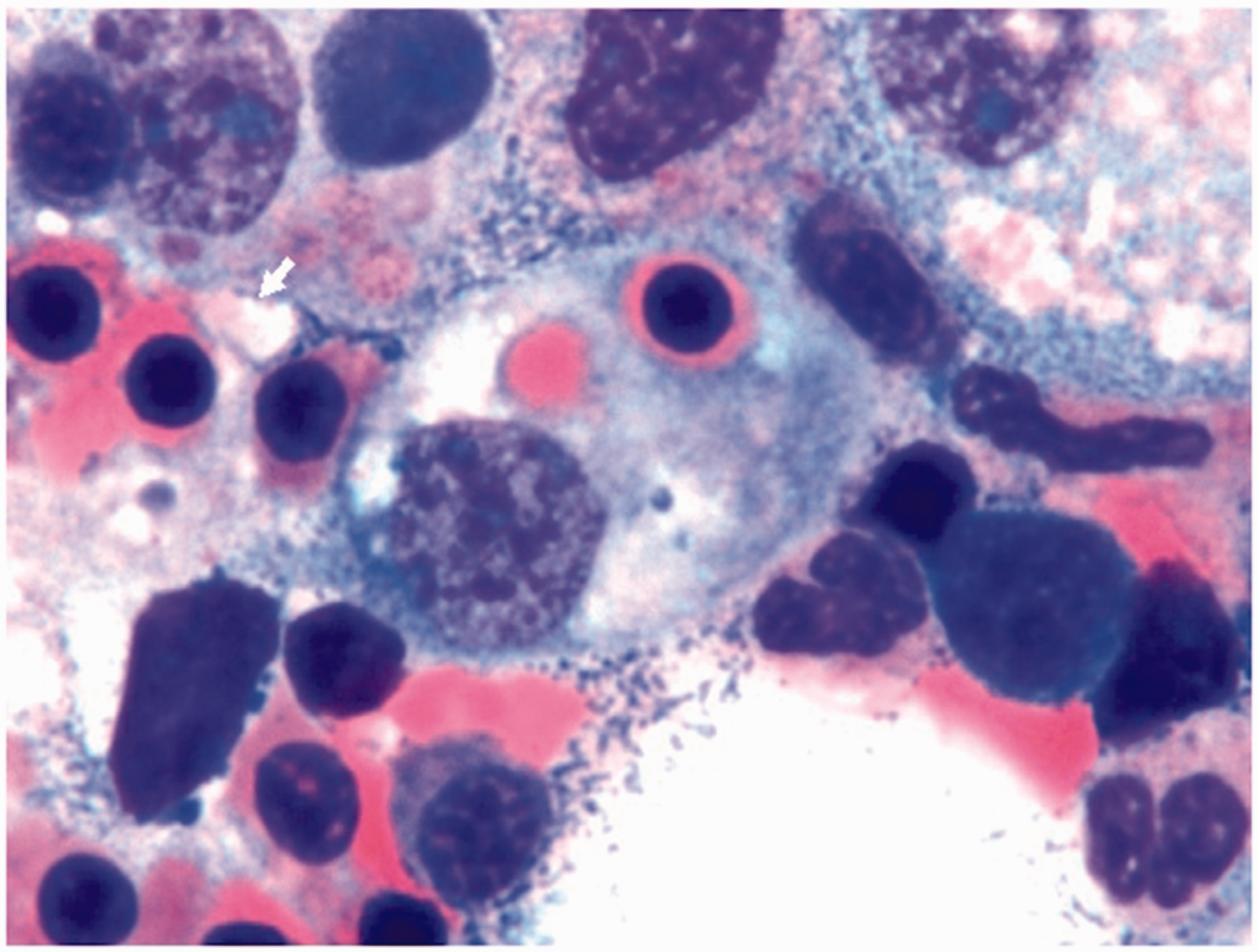
Bone marrow aspirate showing hemophagocyte (arrow) at 100X magnification. Source: Photo courtesy of Hongying Tina Tan, MD, PhD, OVMC-UCLA Pathology Department.
Discussion
Most of our understanding of the pathophysiology of HPS comes from studying the genetic abnormalities responsible for hereditary HPS. These mutations impair the activity of natural killer (NK) cells and cytotoxic T-lymphocytes (CTLs). The dysfunctional NK cells and CTLs are produced in greater numbers and lead to the disproportionate secretion of cytokines and hyperstimulation of macrophages that are responsible for the clinical features of HPS. 1 Interestingly, stimulation of NK cells and CTLs, and precipitation of a cytokine storm by ramp-up viremia are early events in the pathophysiology of HIV-1 infection. 2 The latest iteration of the Histiocyte Society’s diagnostic criteria for HPS assigns a point each for fever ≥38.5°C, splenomegaly, ≥2 cytopenias, ferritin ≥500 ng/ml, triglycerides ≥265 mg/dl, fibrinogen ≤150 mg/dl, and hemophagocytosis. 3 The recently introduced H-score, which was validated specifically for RHS, refines these cutoffs and adds points for underlying immunosuppression, hepatomegaly, and AST ≥30 IU/l. 4 Fever, organomegaly, and increased transaminases are frequently observed in AHI. 2 Ferritin, triglycerides, and fibrinogen are nonspecific acute-phase reactants and are usually abnormal in the setting of inflammation due to any cause although perhaps not to the degree that they are in HPS. Hemophagocytosis is also nonspecific and encountered frequently in HIV-1-infected patients. Our case and the 11 previously reported cases (Table 2) highlight the overlapping symptomatology of these clinical processes and raise important questions regarding the management of patients suspected of being affected by both: Is it appropriate to start ART in this setting? Is immunomodulatory therapy necessary once ART has been started? Several studies have shown that starting ART during AHI may minimize the size and heterogeneity of the latent viral reservoir and optimize the probability of complete immune reconstitution. 14 Furthermore, it appears that a high HIV-1 viral load may be a contributing factor in the pathogenesis of AHI-associated RHS (Table 3). Therefore, rapidly reducing the concentration of circulating virus may interrupt the runaway immune response and symptomatology of AHI-associated RHS. Immunomodulators were used in four of the reported cases (Table 3) but their benefit is unclear at best since all patients survived regardless of immunomodulatory therapy. Treating the precipitant is likely the key step in interrupting the inflammatory cascade. It could be argued that after a certain point, it may be too late to arrest the runaway immune response without immunomodulators but their use in AHI-associated RHS should be limited to cases in which symptoms persist despite prompt initiation of ART. RHS in the setting of AHI is a potentially life-threating phenomenon. Prompt initiation of ART with or without judicious coadministration of immunomodulators in selected cases appears to be a safe and potentially beneficial management strategy.
Clinical features of reported cases.
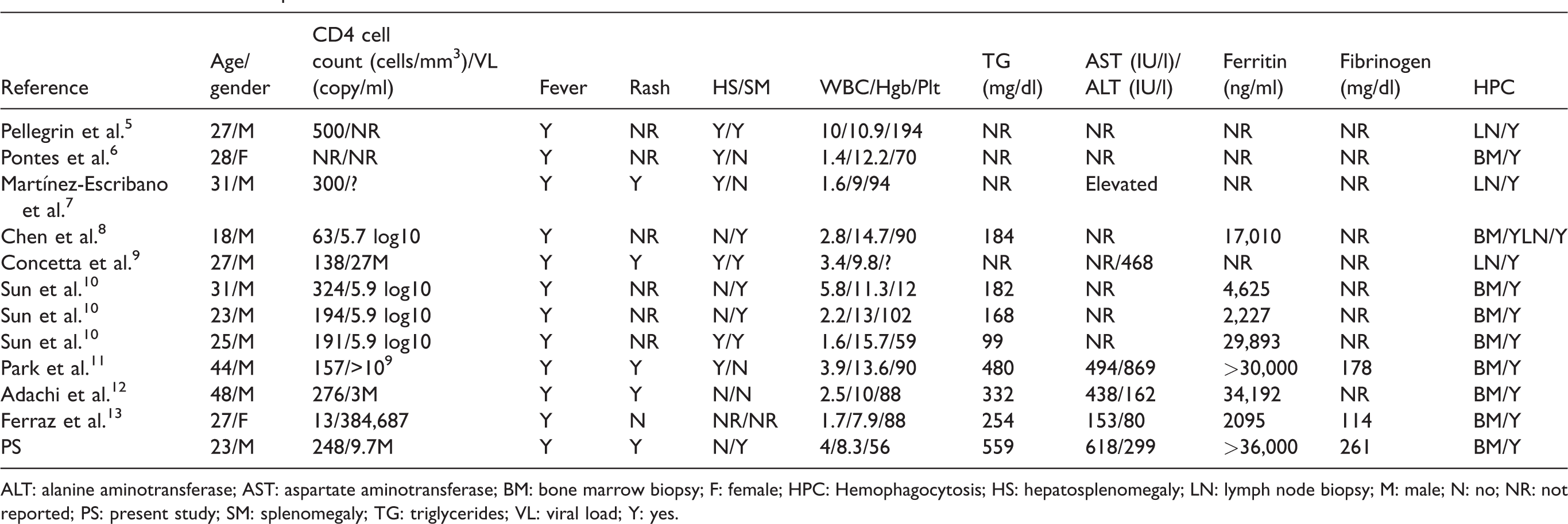
ALT: alanine aminotransferase; AST: aspartate aminotransferase; BM: bone marrow biopsy; F: female; HPC: Hemophagocytosis; HS: hepatosplenomegaly; LN: lymph node biopsy; M: male; N: no; NR: not reported; PS: present study; SM: splenomegaly; TG: triglycerides; VL: viral load; Y: yes.
Treatment and outcome of reported cases.
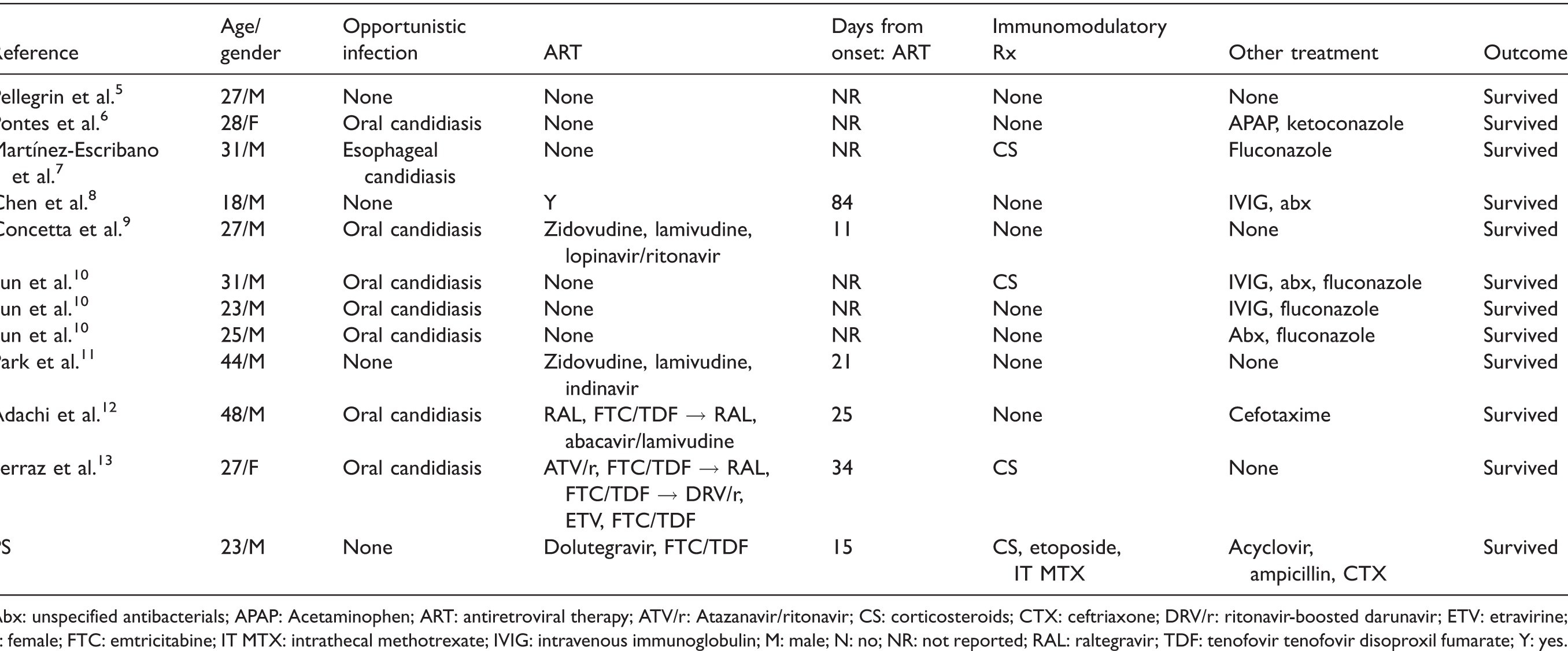
Abx: unspecified antibacterials; APAP: Acetaminophen; ART: antiretroviral therapy; ATV/r: Atazanavir/ritonavir; CS: corticosteroids; CTX: ceftriaxone; DRV/r: ritonavir-boosted darunavir; ETV: etravirine; F: female; FTC: emtricitabine; IT MTX: intrathecal methotrexate; IVIG: intravenous immunoglobulin; M: male; N: no; NR: not reported; RAL: raltegravir; TDF: tenofovir tenofovir disoproxil fumarate; Y: yes.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.