
Abstract
Human papillomavirus (HPV) prevalence varies by population. This study investigated anal HPV type detection risk by country in a population of men who have sex with men (MSM) and transgender women (TW) at risk of HIV. Sexually active HIV-1-uninfected MSM and TW were enrolled at eight sites: four in the United States (US), two in Thailand, one in Peru, and one in South Africa. Baseline anal HPV swabs were collected, and DNA typing was performed. One hundred and ninety-five participants, 76 (42%) from the US, had a mean age of 30.9 years (range 18–64). In 182 participants with results available, anal HPV infection was common with 169 (93%) with ≥1 type, 132 (73%) with ≥1 nine-valent vaccine types, and 66 (36%) with HPV 16. Participants in the US had a higher prevalence of HPV 16 (56%, p = 0.004) and HPV 6 (69%, p < 0.001) compared to the other regions. Stimulant drug use was significantly associated with HPV 6 detection. Anal HPV is highly prevalent in this population of MSM and TW sampled from four countries, with HPV 16 the most commonly detected type. The nine-valent HPV vaccine has the potential to provide significant protection if given prior to exposure.
Summary
Anal HPV detection, predominantly with HPV 16, is common in HIV-uninfected MSM and TW. Vaccinating this at-risk population should be encouraged.
Introduction
Men who have sex with men (MSM) and transgender women (TW) are at increased risk of HIV infection1–3 and are frequently coinfected with anal human papillomavirus (HPV).4,5 It is recommended that the prophylactic HPV vaccine be administered prior to potential exposure to HPV. 6
Following anogenital HPV infection, clinical sequelae can include the development of warts, dysplasia, and squamous cell cancer. The worldwide incidence of HPV-associated anal cancer is increasing in both men and women with current rates in the United States (US) approximating 2/100,000. 7 In MSM, the reported overall incidence of 35/100,000 is similar to that of cervical cancer prior to the introduction of cervical cytology screening, with rates approximately 2–3 times higher currently seen in HIV-infected MSM.8,9 Additionally, prevalent HPV has been identified as a risk factor for incident HIV infection in the anal canal in men 10 and uterine cervix in women, 11 while persistent or resolving penile HPV infection has also been shown to increase HIV risk in men. 12
Approximately 40 HPV types infect the anogenital area and these can be broadly differentiated into high-risk (HR) and low-risk (LR) types based on their historical association with cervical cancer. 13 Over 80% of all anal cancers are related to persistent infection with HR HPV infection, with HPV 16 being the most commonly associated type. 14 Anal HPV-associated disease due to HPV types 6, 11 (LR) and types 16, 18, 31, 33, 45, 52, and 58 (HR) may be prevented with the use of the nine-valent HPV vaccine (9vHPV) Gardasil®9 (Merck and Co., Kenilworth, NJ).6,15–17 In the US and Puerto Rico this vaccine is indicated for males and females aged 9–26 years, with optimal efficacy seen in individuals without evidence of current or past HPV infection. 6 Other available prophylactic vaccines with reduced valency include Gardasil (HPV 6, 11, 16, 18) (Merck and Co., Kenilworth, NJ), and Cervarix (HPV 16, 18) (GSK, Brentford, UK) that is licensed only for females. In Thailand, Peru, and South Africa while HPV vaccines have been approved for use by the respective governmental agencies, there is no indication for its use in males.
Risk factors for anal HPV infection include receptive anal intercourse (RAI), smoking, immunosuppression, genital warts, higher sexual partner number, and injection drug use. 18 In Western populations, the prevalence of anal HPV infection in MSM varies, with reported rates in non-population-based sampling of 45–70% in HIV-uninfected MSM, with HPV 16 the most common type.19–22 In Thailand and Peru, anal HPV infection rates are 58 and 51% in HIV-uninfected MSM, respectively, while in the same population in South Africa the anal HPV infection rate is 73%.23–25 There are few data specifically addressing anal HPV infection in HIV-uninfected TW.
We hypothesized that anal 9vHPV types would vary by geographical location, and this subanalysis of MTN-017 is aimed to define the prevalence of anal HPV and risk factors in a population of sexually active MSM, and TW at risk of HIV infection.
Materials and methods
Study design
MTN-017 was a phase 2 randomized sequence open label expanded safety and acceptability crossover study of the oral emtricitabine/tenofovir disoproxil fumarate tablet and rectally applied tenofovir reduced-glycerin 1% gel (ClinicalTrials.gov number NCT01687218). The MTN-017 study protocol is available at http://www.mtnstopshiv.org/studies/4495. The primary manuscript was published in Clinical Infectious Diseases. 26 What follows is an additional exploratory subanalysis that was not included in the original study analysis plan.
Study sites
There were eight study sites: four in the US (Boston, Pittsburgh, San Francisco, and San Juan), two in Thailand (Bangkok and Chiang Mai), and one each in Peru (Lima) and South Africa (Cape Town).
Ethical considerations
Prior to implementation, the study protocol was reviewed and approved by the institutional review boards/ethics committees at each participating site. In addition, the protocol was approved by the Thailand Ministry of Public Health Ethical Review Committee for Research in Human Subjects, the South African Medicines Control Council, the US Centers for Disease Control and Prevention Institutional Review Board, the Peruvian National Institute of Health (Instituto Nacional de la Salud), and the Prevention Sciences Review Committee of the National Institute of Allergy and Infectious Diseases of the US National Institutes of Health. All participants provided written informed consent.
Population
Healthy HIV-1-uninfected MSM and TW ≥18 years of age with a history of RAI at least once in the previous three months were recruited via social and traditional media, online advertising, flyers, community engagement, and word of mouth. Individuals with abnormalities of the colorectal mucosa, significant gastrointestinal symptoms, rectal Chlamydia trachomatis or Neisseria gonorrhoeae infection or any sexually transmitted infection requiring treatment, chronic hepatitis B infection, hepatitis C exposure, a requirement to use drugs that were likely to increase the risk of bleeding following mucosal biopsy, or symptoms suggestive of HIV seroconversion were excluded from the study. Full inclusion and exclusion criteria are available at http://www.mtnstopshiv.org/studies/4495.
Anal HPV sample collection
All study site staff were trained by the same study team on anal swab collection technique and laboratory sample management. Anal swabs were collected at the study enrollment visit prior to digital rectal examination. A water-moistened Dacron swab from the Digene Female HPV Swab Specimen Collection Kit (Qiagen, Venlo, Netherlands) was inserted a minimum of 6 cm proximal to the anal verge to ensure anorectal transition zone sampling. With lateral pressure on the swab, it was rotated in a circular fashion while being withdrawn over 10–15 s. The swab was immediately placed into the kit specimen transport tube, the shaft was snapped leaving the swab inside, and the tube capped. The tube was stored at ≤ −70°C within 2 h of collection and batched shipped from study sites to the MTN central laboratory on dry ice.
HPV detection
Testing was undertaken using the PapilloCheck® (Greiner Bio-One, Kremsmünster, Austria) platform. After viral and human DNA were extracted from the swab specimen, a 350 base-pair fragment of the HPV E1 gene was amplified in the presence of HPV-specific primers by polymerase chain reaction and the amplified products were hybridized to specific DNA probes fixed on a DNA chip. Both LR (6,11,40,42,43,44) and HR (16,18,31,33,35,39,45,51,52,53,56,58,59,66,68,70,73,82) HPV types were reported.
Statistical analysis
Linear regression models using a log link were used for baseline factor significance testing of HPV positivity in participants for each HPV type. All p-values were two sided. Due to the exploratory nature of these analyses, there were no adjustments made for multiple comparisons. For multivariable models, backward stepwise regression with a log link was used to find the factors most predictive of HPV infection using all the variables of interest. Results presented are from the bivariate models unless otherwise noted.
Lubricant and saliva use were reported only in categorical form. If either saliva and another lubricant were used more than infrequently but both were less than always, the participant was considered a frequent user of lubricant. In addition, if the participant reported no partners in the past eight weeks, the participant was categorized as never using lubricant or saliva and as not having had RAI. The variable for condom use with RAI was divided into four categories: no RAI in past eight weeks which included participants with no partners in past eight weeks, no condom used with RAI in the past eight weeks, sometimes used a condom with RAI in the past eight weeks, and always used a condom with RAI in the past eight weeks.
Results
Between September 2013 and November 2014, 349 participants were screened and 195 enrolled. There were 13 participants who did not have any HPV test results available due to test failure: six from San Francisco; two from Bangkok; and one each from San Juan, Pittsburgh, Boston, Cape Town, and Lima. Therefore, this analysis included the 182 enrolled participants with HPV results. One participant at the Lima site had HPV testing at an interim visit one week after enrollment and one participant at the Boston site received at least one quadrivalent HPV vaccination; both were included in the analysis.
Participant demographic and baseline characteristics variables are presented in Table 1. The mean participant age was 30.9 years (range 18–64), with 114 (63%) over the age of 26 years and thus ineligible for HPV vaccination. Most participants identified as male (158, 87%), were sexually active (174, 97%) and the majority were recruited from the US (76, 42%). Stimulant drug use was uncommon (23, 13%) and over half the participants had never smoked or had not smoked cigarettes in the past eight weeks (122, 68%). Participants douched in preparation for RAI a mean of 5.3 times (range 0–60) in the previous eight weeks, lubricant use (whether commercial lubricant, household product, or saliva) was common (150, 90%), and 71 (41%) reported not using condoms for RAI in the past eight weeks.
Demographics and baseline characteristics.

HPV: human papillomavirus; RAI: receptive anal intercourse; STI: sexually transmitted infection.
One participant refused to report gender. The significance test for gender is male versus transgender woman or other.
Information not reported for one or more participants.
Douche use is a continuous variable. Mean, standard deviation, median, quartiles, minimum, and maximum are presented.
Overall, anal infection with HPV was common, with 169 (93%) of participants having at least one of the HPV types tested. For the 9vHPV types, 132 (73%) were positive for at least one type with the most and least common types being HPV 16 (66, 36%) and HPV 33 (8, 4%), respectively. The prevalence of all HPV types tested is shown in Table 2, including non-9vHPV LR types that ranged from 3% (HPV 73) to 23% (HPV 51), and HR types that ranged from 11% (HPV 58) to 20% (HPV 39). The prevalence of HPV 16 as it relates to demographic and baseline characteristics is shown in Table 3. Between countries, participants in the US had a significantly higher prevalence of HPV 16 (RR estimate 1.8, 95% confidence limits [1.2, 2.6], p = 0.004) and HPV 6 (RR estimate 3.2, 95% confidence limits [1.7, 6.0], p < 0.001) compared to the other geographical regions with prevalence of 56 and 69%, respectively (Tables 3 and 4). The prevalence of anal HPV 6 and 16 by clinical site is shown in a supplemental table. In addition, participants who had ever used stimulant recreational drugs were more likely to be HPV 6 positive (RR estimate 2.6, 95% confidence limits [1.5, 4.7], p = 0.001) (Table 4). In a multivariable model, geographic region remained statistically significant after adjusting for other demographic and baseline characteristics (data not shown).
Anal HPV type prevalence.
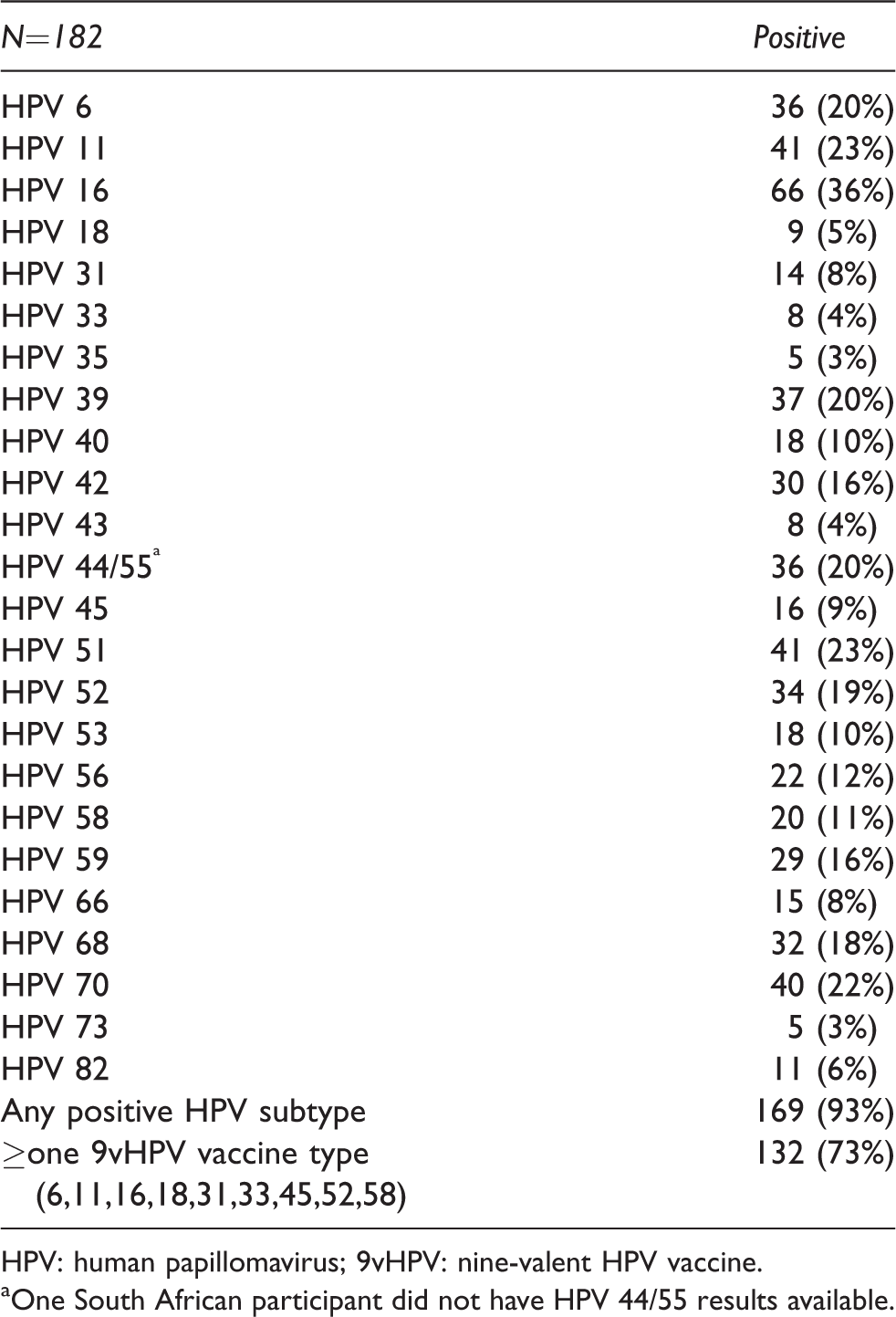
HPV: human papillomavirus; 9vHPV: nine-valent HPV vaccine.
One South African participant did not have HPV 44/55 results available.
HPV 16 prevalence by demographic and baseline characteristics.
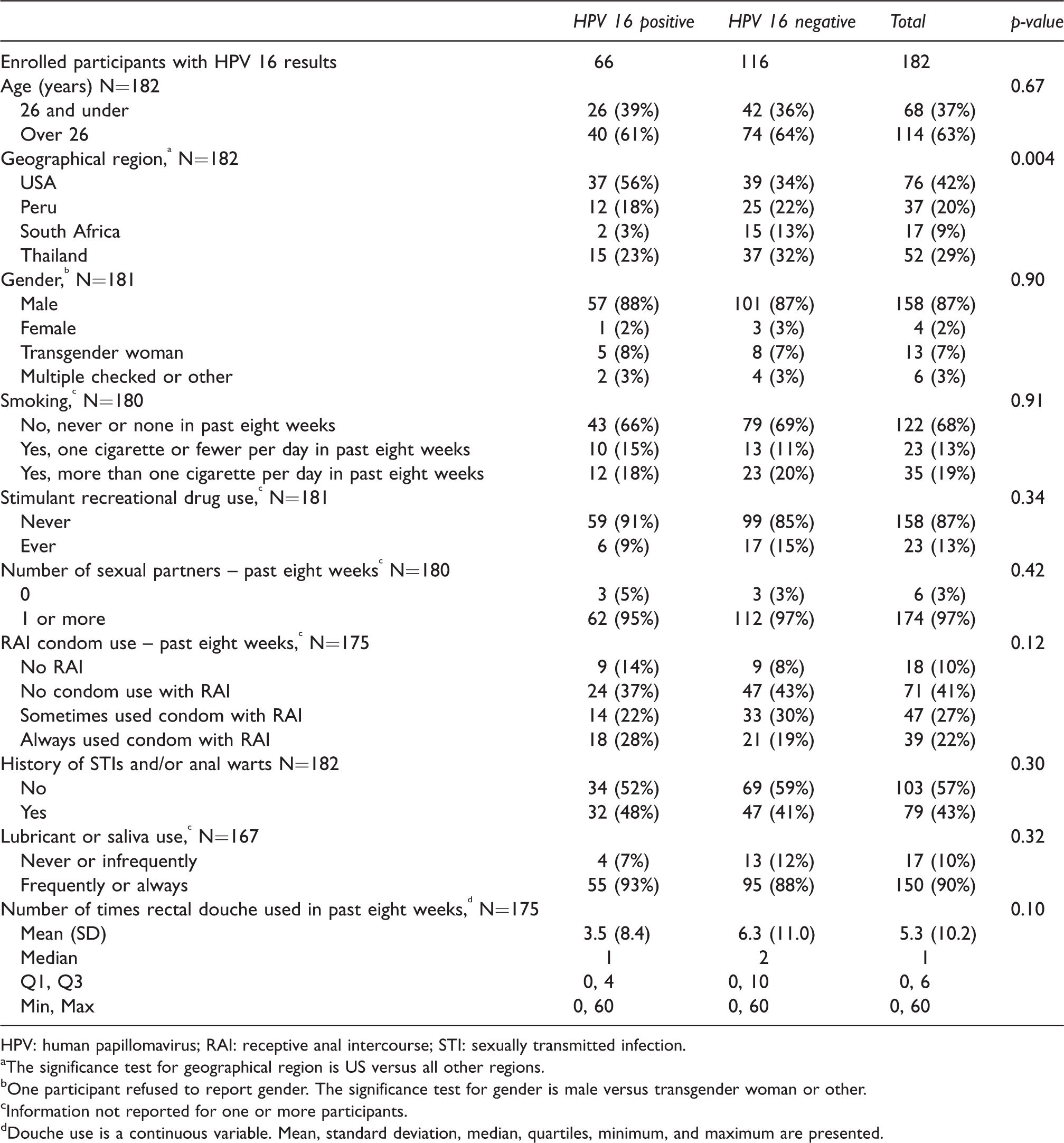
HPV: human papillomavirus; RAI: receptive anal intercourse; STI: sexually transmitted infection.
The significance test for geographical region is US versus all other regions.
One participant refused to report gender. The significance test for gender is male versus transgender woman or other.
Information not reported for one or more participants.
Douche use is a continuous variable. Mean, standard deviation, median, quartiles, minimum, and maximum are presented.
HPV 6 prevalence by demographic and baseline characteristics.
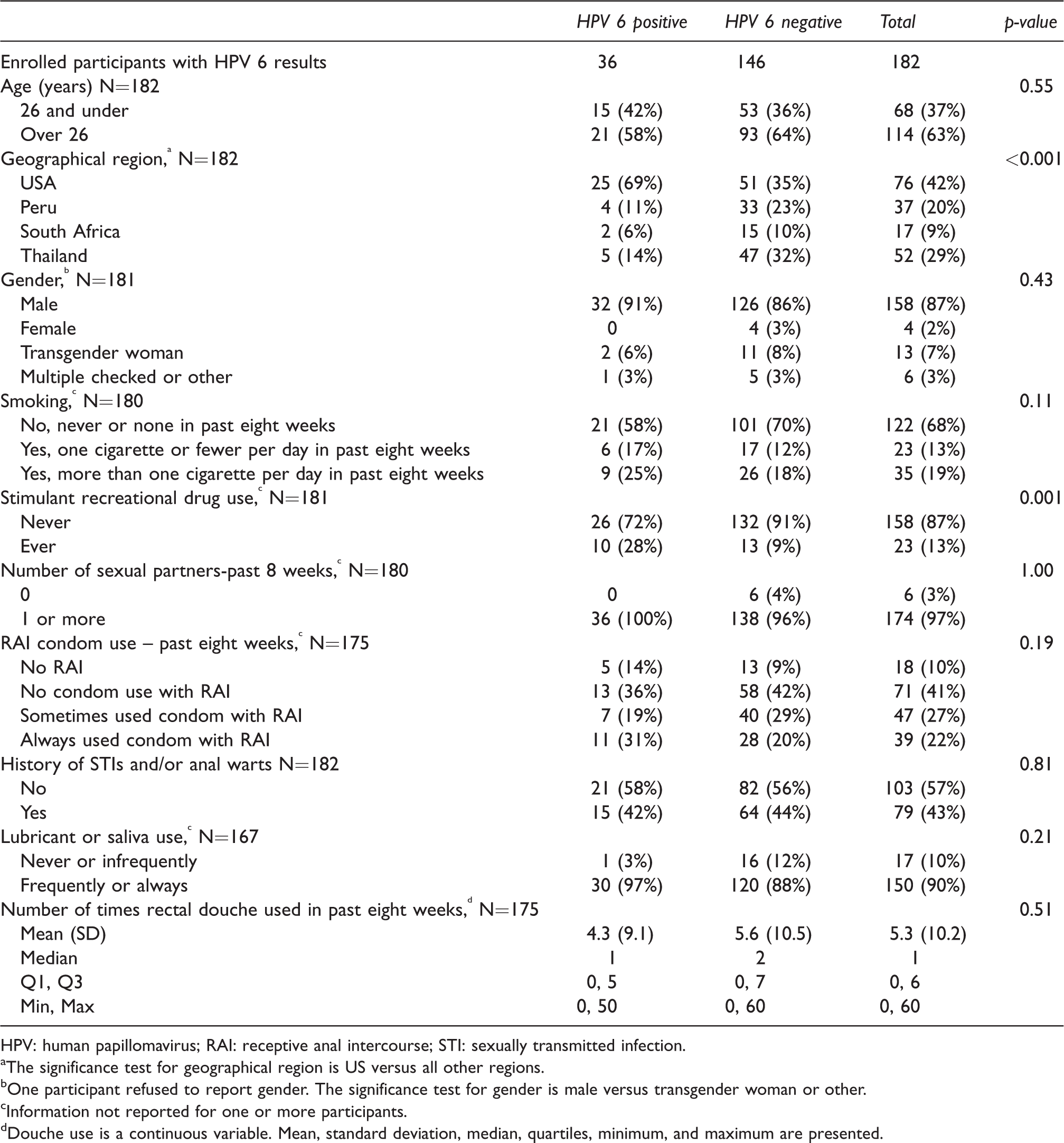
HPV: human papillomavirus; RAI: receptive anal intercourse; STI: sexually transmitted infection.
The significance test for geographical region is US versus all other regions.
One participant refused to report gender. The significance test for gender is male versus transgender woman or other.
Information not reported for one or more participants.
Douche use is a continuous variable. Mean, standard deviation, median, quartiles, minimum, and maximum are presented.
Participants who used lubricants or saliva frequently or always for RAI were less likely to be HPV 33 positive (p = 0.015). There was no significant association detected with rectal douching and HPV detection.
For the combined 9vHPV type outcome, no significant differences were found using multivariable logistic regression between HPV-positive and HPV-negative participants for any of the demographic or baseline characteristics of interest (Table 5).
Combined HPV a prevalence by demographic and baseline characteristics.
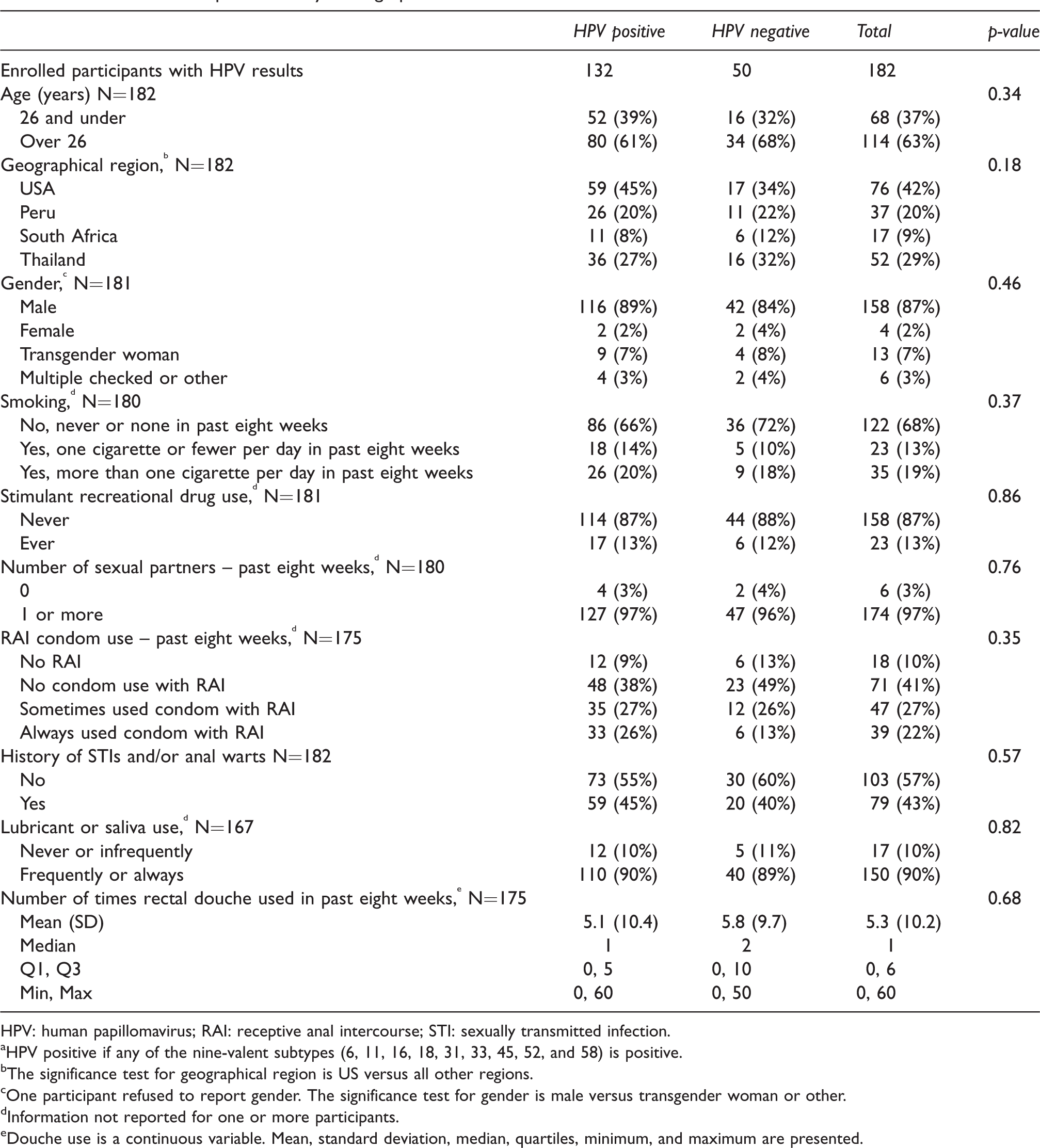
HPV: human papillomavirus; RAI: receptive anal intercourse; STI: sexually transmitted infection.
HPV positive if any of the nine-valent subtypes (6, 11, 16, 18, 31, 33, 45, 52, and 58) is positive.
The significance test for geographical region is US versus all other regions.
One participant refused to report gender. The significance test for gender is male versus transgender woman or other.
Information not reported for one or more participants.
Douche use is a continuous variable. Mean, standard deviation, median, quartiles, minimum, and maximum are presented.
Discussion
This HIV-uninfected study population had a high prevalence of anal HPV with predominance of HPV 16 that places the group at increased risk of adverse HPV-associated outcomes such as dysplasia and cancer.
Anal HPV is highly infectious and is strongly associated with RAI. 22 Even in this lower risk population without other viral coinfections, the high rates of condomless RAI likely contributed to increased rates of anal epithelial HPV exposure and subsequent risk of establishing infection. The predominance of HPV 16 seen in this population, like previous studies, is cause for concern as MSM are at higher risk for both anal dysplasia/cancer outcomes related to persistent HR-type infection.
In this international study there was variation in HPV prevalence by country, with US participants more likely than their peers in Peru, Thailand, or South Africa to have detectable anal HPV 6 and 16. This, however, was in the context of lower than expected rates at the non-US sites compared to previous reports in these countries. One consideration is that the US study sites may have been more familiar with anorectal sample collection related to their previous experience with rectal microbicide development studies, despite identical clinical staff training at all sites that impacted specimen adequacy.
Despite the likelihood that individual anal infections will be cleared over time in many of the current population, 27 the comparable HPV prevalence in the 26 years and under, and older age groups indicates ongoing sexual exposure and infection. 28 Some of these prevalent infections, particularly with HPV 16 that is less rapidly cleared than other types, 27 may represent persistent infection that places the individual at increased risk of cancer-associated HPV associated sequelae.
The increased detection of HPV 6 that is commonly associated with exophytic warts in participants taking stimulant drugs is intriguing – even more so as this was seen despite lower levels of stimulant drug use reported in this population. Recent studies have indicated that some types of stimulant drugs have immunosuppressant effects 29 that may contribute to increased HPV prevalence as is seen in HIV-infected individuals with lower CD4 T cell counts. 30 While this mechanism may contribute to the current study findings for HPV 6, it does not explain why other HPV types were not similarly affected, although this may be related to the smaller numbers of HPV-infected participants in this exploratory analysis.
Cigarette smoking is also associated with an increase in anal HPV detection, possibly by local immune suppression, 31 but despite 32% of participants verifying smoking at some time in the prior eight weeks there was no significant increase in anal HPV detection in this group. Information was collected on ‘ever smoking/smoking in the previous 8 weeks,’ and either a closer temporal association to sampling may be required or one that is related to lifetime exposure to cigarette smoke/nicotine.
Both douching practices prior to RAI and use of lubricant to facilitate RAI appear to be inconsistently associated with either increased or decreased detection of individual HPV types. Again, this most likely represents the relatively small number of participants in this analysis and a study with larger numbers of participants would help define these risks further.
The detection of HPV DNA at one timepoint is open to interpretation, with the possible detection of ‘DNA deposition’ from recent sexual partners that does not represent productive infection. Additionally, there may have been a failure to adequately sample and detect all HPV types present. This may result in an over- or underrepresentation of HPVs present, respectively, although this method is comparable to other studies using similar detection techniques. The presence of non-9vHPV types of both LR and HR phenotypes had prevalence rates up to approximately 20%. However, it is HPV types 16 and 18 that are responsible for over 90% of anal cancers and the contribution of these other HR viruses, although possibly contributory, has not been individually defined.
Vaccination of MSM and TW prior to HPV exposure in the population studied has the potential to reduce the high anal HPV prevalence rates seen, as well as avoiding the sequelae of these infections. Unfortunately, most of this study population have no vaccination options as they are either above the age where the HPV vaccination is indicated, or the vaccine is only available to women in their country. In the absence of a therapeutic HPV vaccine or expansion of country-based vaccine recommendations for younger men, they must rely only on awareness of risk for HPV-associated anal disease and seek medical attention accordingly.
Supplemental Material
Supplemental material for Prevalence and determinants of anal human papillomavirus infection in men who have sex with men and transgender women
Supplemental material for Prevalence and determinants of anal human papillomavirus infection in men who have sex with men and transgender women by Ross D Cranston, Alex Carballo-Diéguez, Holly Gundacker, Barbra A Richardson, Rebecca Giguere, Curtis Dolezal, Aaron Siegel, Ratiya P KunjaraNaAyudhya, Kailazarid Gomez, Jeanna M Piper, Javier R Lama, Ian McGowan and the MTN-017 Protocol Team in International Journal of STD & AIDS
Footnotes
Authors’ contributions
Study conception/design: RDC, IM, AC-D, BAR, JMP
Study sample collection: KG, RPKNA, AS
Study data analysis and interpretation: RDC, IM, AC-D, RG, TF, BAR, HG, AS
Involvement in drafting and revising the manuscript: RDC, IM, AC-D, RG, JR, CD, BAR, HG, AS, KG, RPKNA, AS, JMP
Gave approval of the final draft for publication: RDC, IM, AC-D, RG, JR, CD, BAR, HG, AS, KG, RPKNA, JMP
Overall responsibility for accuracy and integrity of the research: RDC, IM, AC-D, BAR, JMP
Acknowledgments
We are grateful to the study participants for their participation and dedication. We thank the study team members at the research sites, the protocol management team, and the MTN leadership operations center for their contributions. We are grateful to Gilead Sciences who provided the FTC/TDF and CONRAD for providing RG-TFV.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RDC (UpToDate medical encyclopedia royalties, Merck and Co. institutional grant support), IMG (Orion biotechnology, ABIVAX consultancy, Aelix Therapeutics).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Institute of Allergy and Infectious Diseases (UM1AI068633, UM1AI068615, UM1AI106707), with co-funding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institute of Mental Health, all components of the U.S. National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the other institutions represented.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.