
Abstract
Despite the decline in HIV mortality and morbidity, Pneumocystis jirovecii pneumonia (PJP) is still frequently seen, particularly in patients with a low CD4+ cell count. We present a case series where we analyzed the possible role of lung ultrasound (LUS) in the management of PJP in a real-life clinical setting. We describe the ultrasound findings from a consecutive series of six HIV patients hospitalized for PJP, all with a favorable outcome, and evaluated with LUS at admission in our ward and then repeated this once during the hospitalization. Multiple B lines indicating interstitial syndrome were detected at admission in all cases, with a bilateral asymmetric pattern mostly localized in middle and upper lobes. In the follow-up LUS, we noted a substantially improved pattern in all patients, observing a reduction of B lines which correlated with clinical amelioration. One patient at admission and three patients during the follow-up showed lung consolidations with hyperechoic spots inside, that might be typical of the disease. In conclusion, LUS could be a practical and noninvasive imaging tool for supporting diagnosis and treatment response of PJP.
Pneumocystis jirovecii pneumonia (PJP) remains one of the most prevalent AIDS-defining illnesses in patients with a low CD4+ T cell count.1–4 Its diagnosis may not always be obvious, especially because of non-specific symptoms and signs, which overlap with those of other infections. 5
Typical radiological findings consist of a reticular interstitial pulmonary pattern, which may be identified on chest radiograph (CXR) or, with more accuracy, on computed tomography (CT) scan.6–8 High-resolution CT (HRCT) is the most appropriate diagnostic imaging tool, showing ground glass opacities which may be associated with reticulations and small consolidations, 9 but it presents some important drawbacks, such as the limited availability (especially in resource-limited countries), high cost and radiation exposure.10,11
Lung ultrasound (LUS) has already been established as a very promising technique in the diagnosis and management of various pulmonary diseases, especially in critically ill patients. 12 It is operator-dependent, but its advantages include bedside availability, the absence of radiation, real-time imaging, and repeatability.13,14 Assessment of a few sonographic features is usually enough to differentiate between different patterns of disease. In particular, B lines are vertical hyperechoic reverberation artifacts which arise from the pleural line and extend to the bottom of the screen without fading, moving synchronously with lung sliding. 15 They are usually an expression of high impedance discontinuities due to close opposition between alveolar air and increased interstitial fluid and allow semi-quantification of congestion of the lung parenchyma. The simultaneous presence of more than three B lines in a single scan is defined as an interstitial pattern 16 which can be later classified into focal or diffuse depending on its distribution. 15 LUS can be used to manage follow-up of patients and assess response to treatment in certain conditions, such as acute decompensated heart failure. 17
In our work, we report the ultrasound features of a series of HIV-infected patients with PJP admitted to the Infectious Diseases Department at the L. Sacco Hospital of Milan. They all underwent LUS assessment at the admission in the ward and then a follow-up examination. No standard protocol was followed. All scans were done by the same two operators, infectious disease residents with about one year of experience after completion of training on LUS. All patients were scanned twice (admission and follow-up) by both operators, who were not blinded in respect of radiological information of each patient.
Patients’ work up included clinical history and examination, blood tests, CXR, bronchoscopy, and CT scan. All these exams were performed routinely for clinical reasons. We considered the diagnosis of PJP to be “definitive” when it was possible to prove the presence of P. jirovecii in respiratory specimens, either with microscopy and staining (Grocott-Gomori), or by performing polymerase chain reaction (PCR). A “suspected diagnosis” was instead defined according to clinical features, radiographic findings, and response to targeted therapy. Our diagnostic criteria were in line with those found in the literature. 18
Six HIV-infected patients were analyzed; four of them newly diagnosed with HIV. Patients’ features are listed in Table 1.
Patients’ demographical, clinical and laboratory features at the time of hospital admission and management.
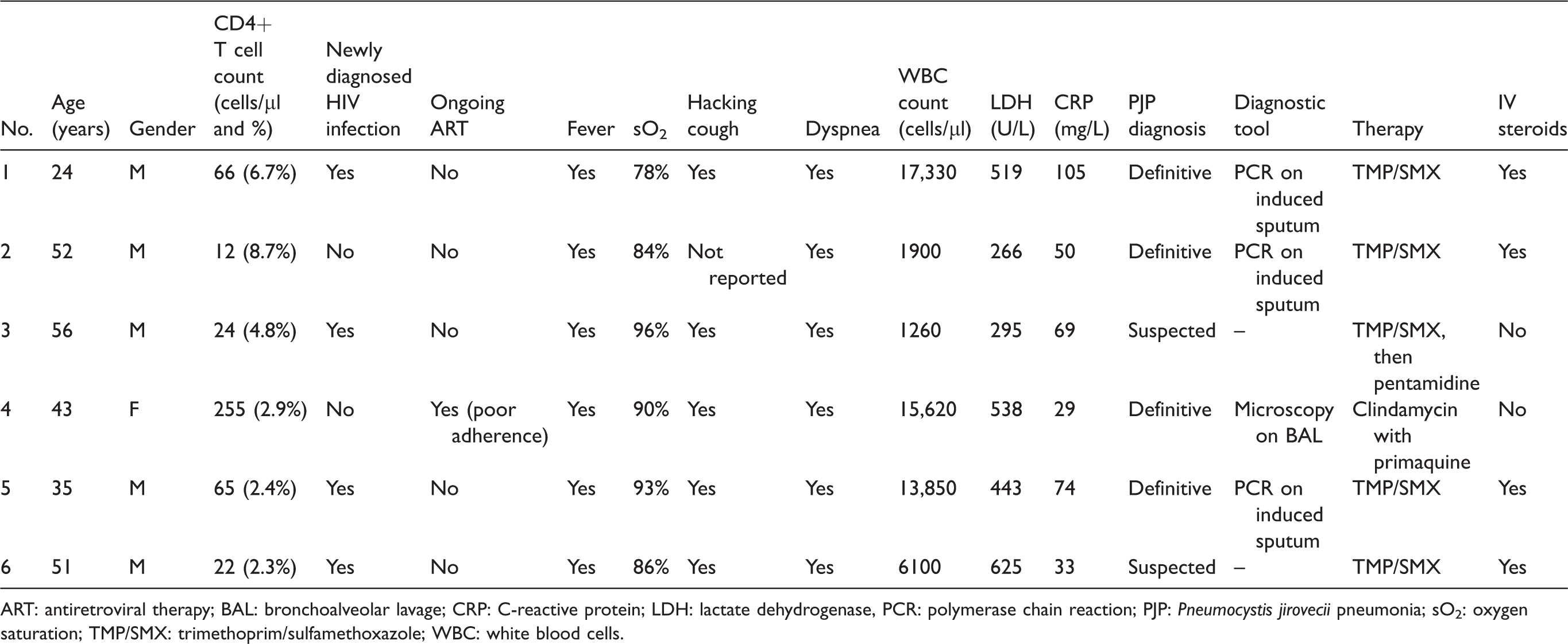
ART: antiretroviral therapy; BAL: bronchoalveolar lavage; CRP: C-reactive protein; LDH: lactate dehydrogenase, PCR: polymerase chain reaction; PJP: Pneumocystis jirovecii pneumonia; sO2: oxygen saturation; TMP/SMX: trimethoprim/sulfamethoxazole; WBC: white blood cells.
At the time of hospital admission all subjects complained of fever and dyspnea, all except one presented with hacking cough and low percutaneous oxygen saturation. Blood exams revealed a rise in C-reactive protein and lactate dehydrogenase (LDH), most patients presented leukocytosis or leukopenia (Table 1). Diagnosis of PJP was confirmed in three cases by PCR on induced sputum and in one case by microscopy on bronchoalveolar lavage, while the remaining two cases showed a complete clinical response to specific treatment. Because of respiratory distress four patients received intravenous steroid therapy. All of them recovered and were discharged after a median of 23 days.
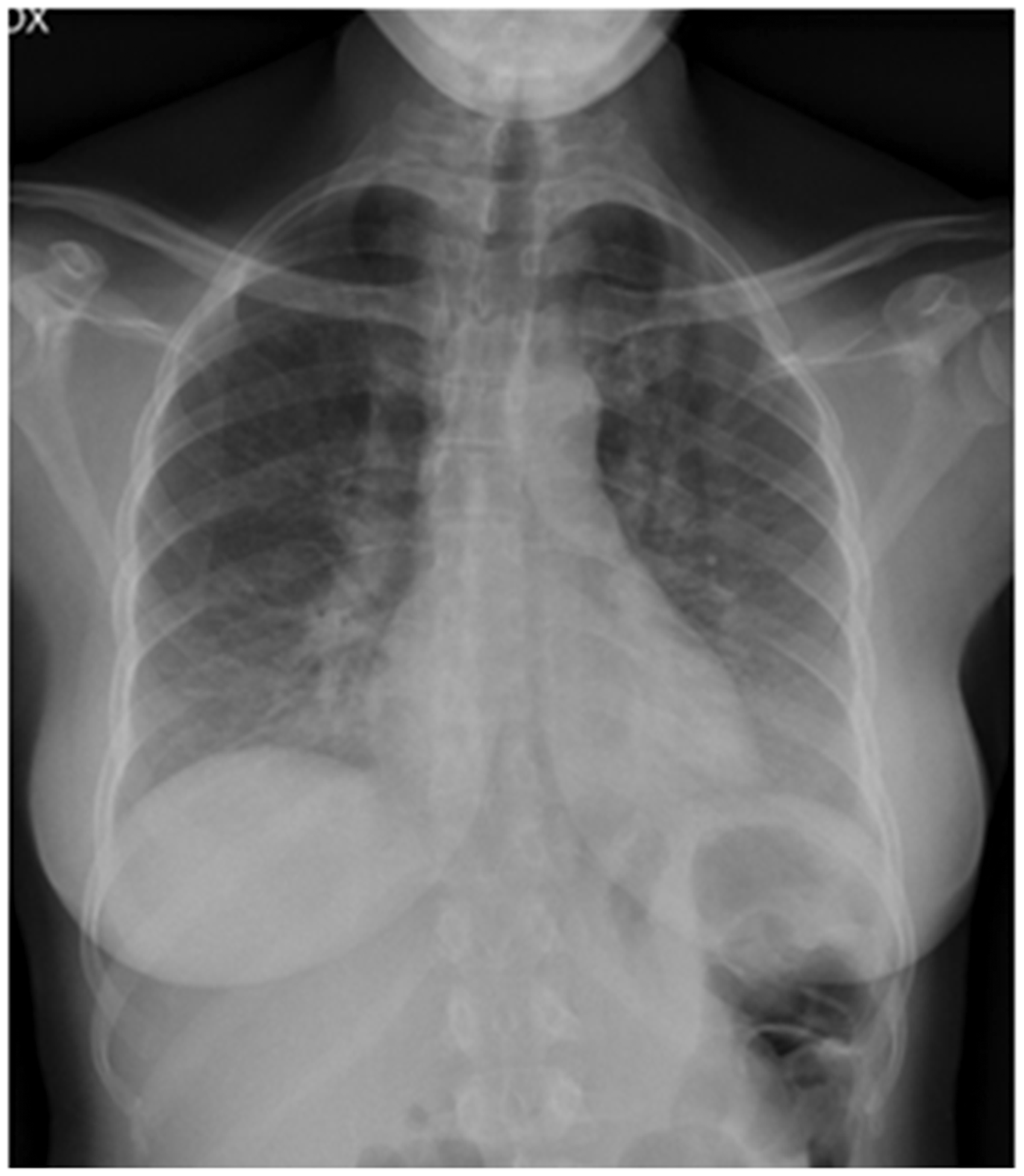
All six patients underwent CXR as first-line imaging in the emergency department, while CT scan was performed in four patients after a median of five days after the admission (see Table 2), showing as the major feature a ground-glass interstitial pattern, sometimes with consolidations.
Imaging assessment and description.
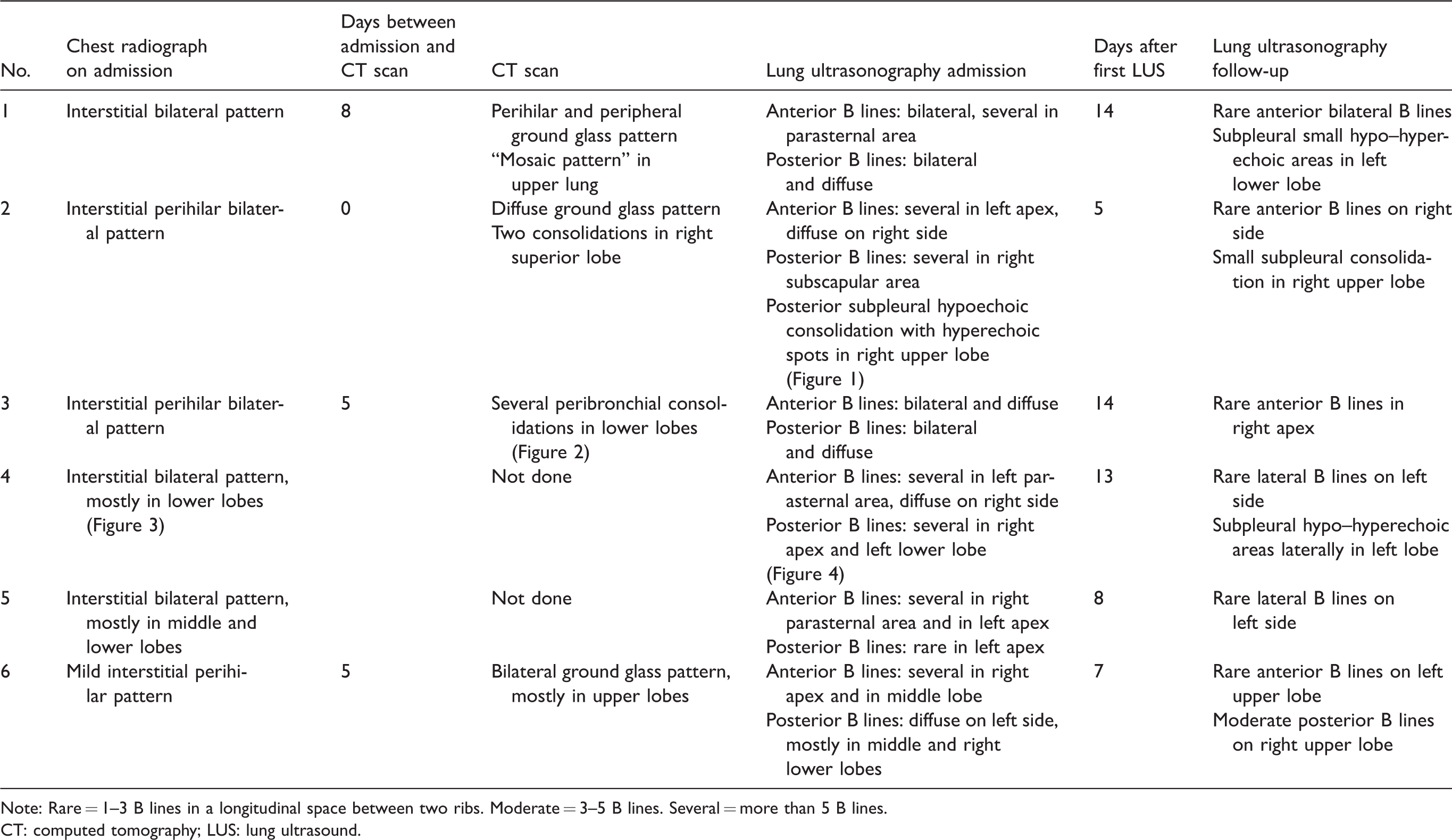
Note: Rare = 1–3 B lines in a longitudinal space between two ribs. Moderate = 3–5 B lines. Several = more than 5 B lines.
CT: computed tomography; LUS: lung ultrasound.
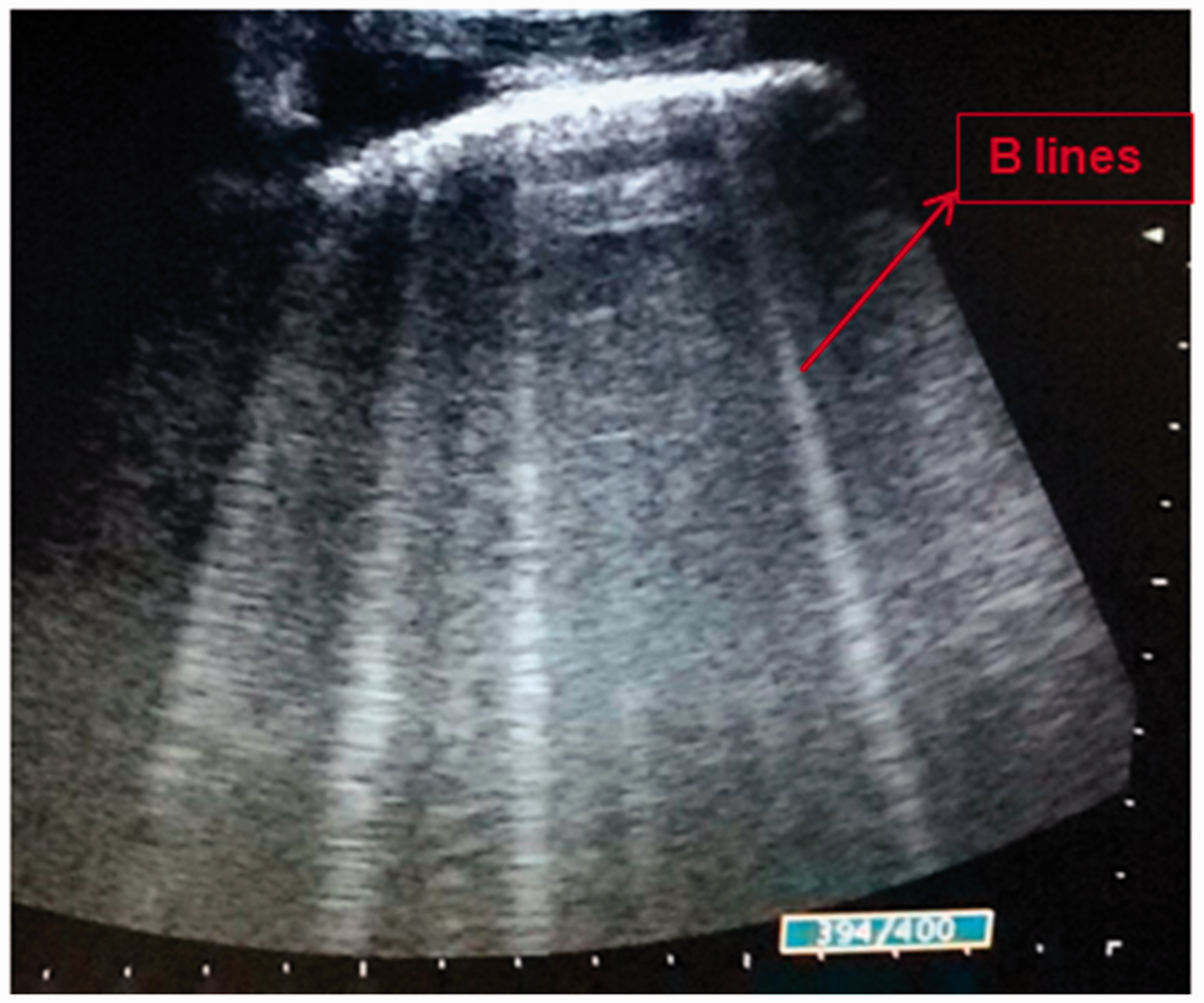
In all cases, the first LUS showed the presence of multiple B lines, specific for interstitial pattern. In particular, the involvement was bilateral but not symmetric and predominantly localized in middle and upper lobes. In one case (patient number 2), we detected peripheral consolidation that was small, subpleural, hypoechoic, interrupting the visceral pleura, and surrounded by some small hyperechoic spots, which was not detected by CXR, but only by CT scan (Table 2; Figures 1 to 4).
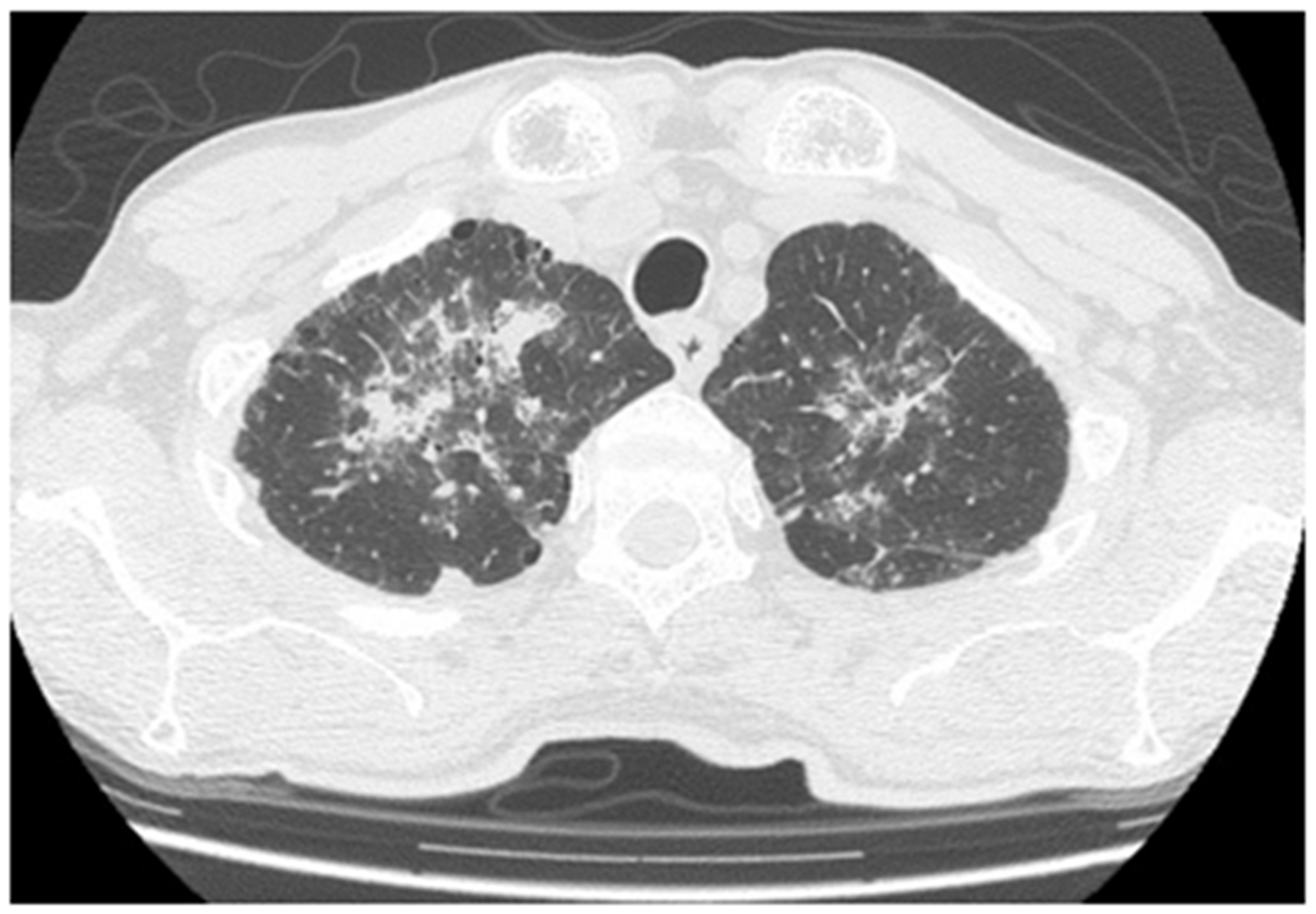
LUS showing hypoechoic peripheral consolidation surrounded by hyperechoic spots (patient number 2). LUS: lung ultrasound. CT scan showing bilateral consolidations (patient number 3). CT: computed tomography. CXR showing an interstitial bilateral pattern in lower lobes (patient number 4). CXR: chest radiograph. LUS showing B lines (patient number 4). LUS: lung ultrasound.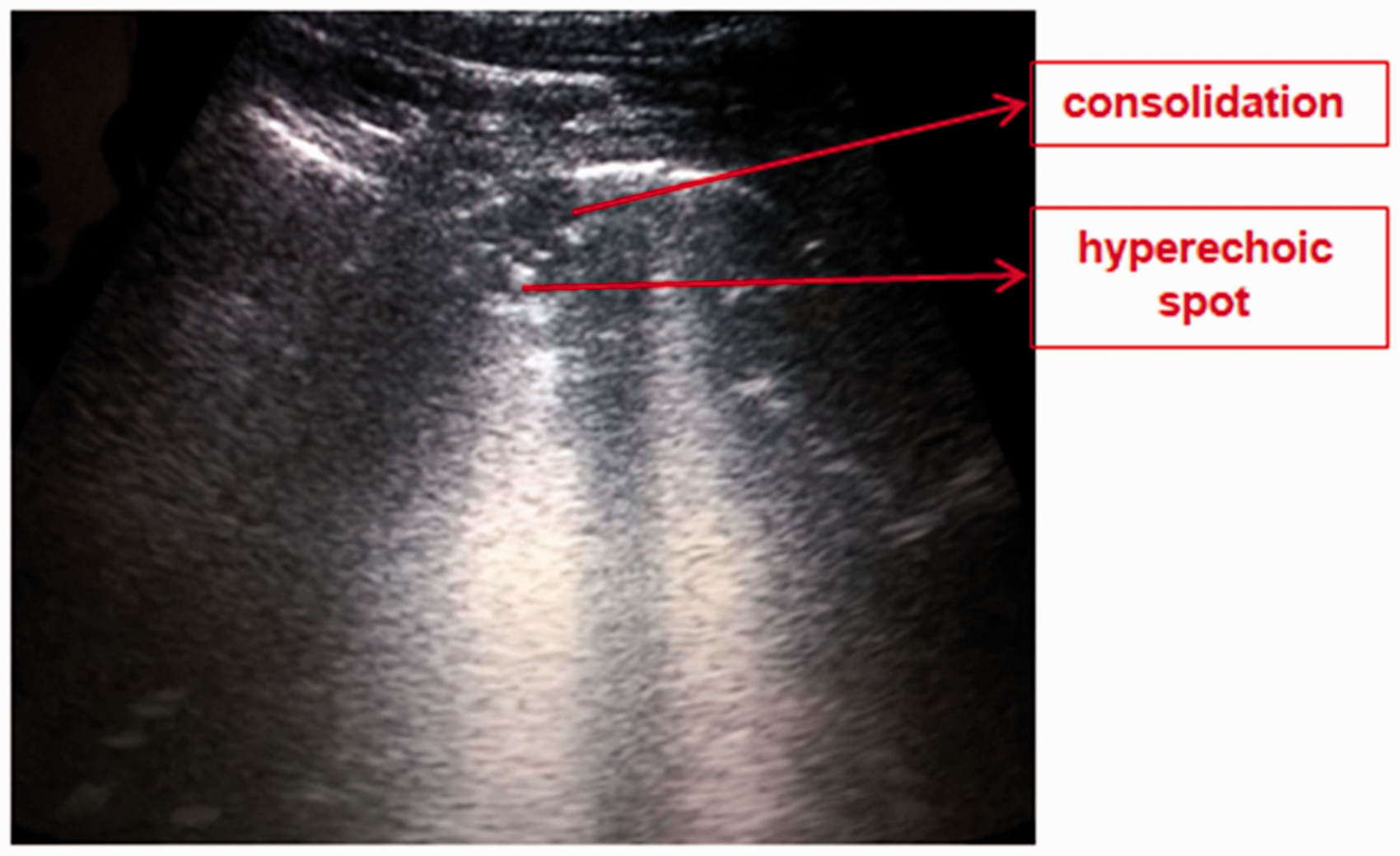
When LUS was performed in the follow-up of these patients, we always noted a reduction of B lines, which correlated with clinical and respiratory improvement, and we interpreted this as a sign of improvement. Moreover, compared to the initial examination, in two cases (patients 1 and 4), small peripheral subpleural hypoechoic areas containing hyperechoic spots appeared only in the second LUS. They seem to be a particular finding already described in other cases of PJP12,19 and that might represent the typical “cystic changes” of the disease (Table 2).
Data on LUS findings in PJP are limited: two case reports,12,20 a case series of six patients, 21 and a recent retrospective case-control study which explored the role of LUS in the diagnosis of PJP. 19 Our LUS features are in line with the expected pattern of interstitial disease, showing diffuse B lines,19–21 but in contrast with findings reported by Japiassu and Bozza, 21 we observed a bilateral but not symmetric localization. B lines, subpleural consolidations, and cystic changes were recently described as suggestive of PJP. 19 In the literature, repeat ultrasound assessment was described in only one patient who was clinically worsening; in this case, LUS showed large consolidated areas with hyperechoic reflexes suggesting air and fluid trapping. 12
Our work has some limitations: all the patients in our case series had a linear clinical course with a gradual improvement and a favorable outcome, thus we interpreted the reduction of B lines as an ultrasonographic sign of amelioration. Furthermore, the small subpleural consolidations may be a typical PJP finding, but their meaning and the timing of their appearance remain unclear and need to be specifically investigated.
LUS has definitely the potential to be helpful in the differential diagnosis of lung diseases in HIV-positive patients.19–21 In the setting of PJP, further research is needed to establish the application of LUS, not only for diagnosis but also in the follow-up of patients.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.