
Abstract
External genital warts (EGW) are the most common viral sexually transmitted infection. Ablative treatments like cryotherapy, curettage, and CO2 laser therapies offer rapid onset of effect, fast clearance, and reduction of virus load. However, these procedures are associated with high recurrence rates (RRs) ranging from 20% to 77% in the short and medium terms and do not provide sustained clearance. After laser therapy removal of EGW, an RR up to 77% has been reported. Topical sinecatechins (TS) 10% is a patient-applied regimen for the treatment of EGW with a low RR (<6.5%) at three months after completion of the therapy in the pivotal trials conducted so far. Sinecatechins can be considered a suitable proactive sequential therapy (PST) after ablative strategies to obtain a low RR. So far, no prospective data are available regarding the efficacy of sinecatechins 10% as PST. We evaluated the efficacy and tolerability of TS 10% ointment applied twice daily in subjects with “difficult to treat” EGW after CO2 laser ablative treatment in a prospective controlled trial. A total of 87 subjects (76 men and 11 women; mean age 42 years) were enrolled in this three-month masked outcome assessment parallel group trial with imbalanced randomization allocation (2:1). One week after a successful CO2 laser treatment, 60 subjects were randomized to TS 10% treatment and 27 subjects to no treatment (control group: ConTRol (CTR); no sequential therapy). All patients had a history of an average of 4.5 previous ablative treatments in the last 12 months due to recurrent EGW. Mean (standard deviation) baseline number of treated lesions was 6.5 (2.7). One subject in the TS arm dropped out due to burning sensation after the application of the product. Therefore, 86 subjects completed the study. After three months, in the TS group, three subjects presented new EGW lesions (RR: 5%) on treated sites. In the CTR group, eight subjects presented new EGW lesions (RR: 29%) on treated sites (p = 0.0024; odds ratio: 0.16; 95% confidence interval: 0.04–0.68). In the TS group, 34 subjects (56%) reported mild to moderate erythema or burning sensation at the application site. In this prospective multicenter trial, the use of TS 10% as PST after ablative treatment with CO2 laser was associated with a lower recurrence rate of new EGW lesions in the short term in comparison with the control group. Comparative larger trials are warranted to evaluate the role of this approach as PST (Trial Registration Number: ISRCTN44037479).
Introduction
External genital warts (EGW) are very common, being the most frequent viral sexually transmitted infection affecting the general population. 1 One percent of the population between the age of 15 and 49 is affected by symptomatic EGW. 2 EGW are caused by human papillomavirus (HPV) infection. 3 So far, more than 200 HPV types have been identified 4 and, among those, 40 types could cause EGW. 5 HPV is transmitted mainly by sexual or direct skin-to-skin contact, and the use of condoms offers only partial protection because skin regions like the mons pubis and proximal penile shaft, not covered by condoms, can transmit infection to a sexual partner. 6 EGW are in general asymptomatic; however, the request of treatment is high to reduce the risk of transmission. Direct and indirect costs of caring for HPV infections represent a significant economic burden. 7 EGW treatment is commonly classified as either provider- or patient-applied. 8 Provider-applied treatments such as cryotherapy, curettage, and CO2 laser therapy offer rapid onset of effect, fast clearance, and reduction of virus load. However, these procedures are associated with high recurrence rates (RRs) of 20%–77% in the short and medium terms and do not provide sustained clearance. 9 After CO2 laser therapy removal of EGW, an RR up to 60%–77% has been reported. 10 CO2 laser therapy relies upon the use of a concentrated beam of infrared light energy, which will heat and eventually vaporize the targeted areas. 11 Topical sinecatechins (TS) 10% (green tea extract) is a patient-applied regimen for the treatment of EGW with a low RR (6.5%) at three months after completion of the therapy in the pivotal trials conducted so far. 12 As first-line therapy, this product should be applied three times a day up to 16 weeks of treatment. 13 However, sinecatechins, like imiquimod, can be considered a suitable proactive sequential therapy (PST) after ablative strategies to obtain a low RR. 14 On et al. 15 have shown that sinecatechins 15% ointment, used sequentially after cryotherapy, is more effective in comparison with cryotherapy alone in reducing EGW lesions. So far, no prospective controlled clinical data are available evaluating the efficacy of sinecatechins 10% as PST after CO2 laser ablative treatment.
Study aim
We evaluated the efficacy and tolerability of TS 10% ointment applied twice daily in subjects with EGW after ablative therapy with CO2 laser in a prospective randomized trial evaluating the RR of new EGW lesions at the treated sites (The PACT Trial: post-ablation immunomodulator treatment of condylomata with sinecatechins).
Materials and methods
Study design
This was a three-center, prospective, masked-assessment outcome, two-arm parallel trial with imbalanced randomization allocation (2:1). The study protocol was approved in July 2017 by the Institutional Review Board of the Coordinating Center (Tor Vergata University, Rome). The trial was conducted according to the Declaration of Helsinki and the International Conference on Harmonization-Good Clinical Practice Guidelines. 16 Trial Registration Number was ISRCTN44037479. The study was conducted in three tertiary level Sexual Transmitted Disease Centers in Italy.
Subjects
Eligibility criteria were: immunocompetent men or women aged 18 years or more, with clinically typical visible EGW lesions (first appearance or recurrent) suitable for ablative procedures located in the penile shaft, glans, pubis, scrotum, and labia majora. Anal and meatal lesions were excluded. Exclusion criteria were immunosuppression, pregnancy or breastfeeding, or known allergy to green tea extract. All participating subjects provided written informed consent. After routine skin cleaning preparation (5% povidone iodine solution) and local anesthesia with 2% lignocaine, the EGW lesions and a 2-mm margin around them were evaporated with CO2 laser (SmartXide 2; DEKA M.E.L.A. Srl – Calenzano, Florence, Italy). This laser had a fractional mode with the wavelength of 10,600 nm and fluency of 5 J/cm2. Laser therapy was repeated every three weeks up to six weeks depending on the clinical response (partial or complete response or the appearance of new lesions). Two weeks after the last EGW laser ablative treatment, a total of 87 subjects (75 men and 12 women; mean age 42 years) were enrolled in this three-month randomized, masked-assessment outcome parallel group with imbalance randomization allocation (2:1) trial. Sixty subjects were allocated to TS 10% ointment (Veregen™, Cantabria Labs Difa Cooper, Caronno Pertusella, Italy) twice daily (morning and evening) treatment for three months and 27 subjects allocated to no treatment (CTR group; no sequential therapy). Sinecatechins ointment was applied to the laser-treated areas and to the surrounding skin margin (a radius of 1 cm). Compliance with the sinecatechins treatment was evaluated by checking the returned empty tubes at the final visit. The randomization list was generated with dedicated computer software (RandomizedIt!; www.Random.org. Dublin, Ireland.).
Study outcomes
The primary outcome was to compare the percentage of subjects with the appearance of new lesions in the area treated with laser CO2 and TS during a three-month observational period after the last ablative session. An investigator, for each participating center, evaluated the primary outcome of the trial unaware of group allocation. The secondary outcome of the study was the evaluation of local tolerability, recording the appearance of local side effects such as burning, itching, pain. The intensity of skin side effects was graded as none, mild, moderate, or severe.
Statistical analysis and sample size calculation
Statistical analysis was performed using GraphPad statistical software ver. 13.0 (La Jolla, CA, USA). Continuous variables were expressed as mean ± standard deviation (SD). The primary endpoint of the trial was the comparison between TS and CTR groups of the percentage of subjects with the appearance of new lesions during the study observational period. The Chi square test was used for the analysis of this study outcome. We also calculated the 95% confidence interval (CI) of the odds ratio (OR). Sample size calculation was performed on the hypothesis that sinecatechins treatment could reduce the risk of recurrence of new lesions from 70% to 10%. With an alfa value of 0.05 and a power of 95%, a total of at least 70 subjects (with a randomization balance of 2:1) should be enrolled to detect this difference. With a hypothesis of a 20% dropout rate, we decided to enroll at least 80 evaluable subjects. The sample size was calculated using G-Power statistical software version 3.9 (Kiel, Germany). A p-value of <0.05 was considered significant. The analysis was performed based on an intention-to-treat basis.
Results
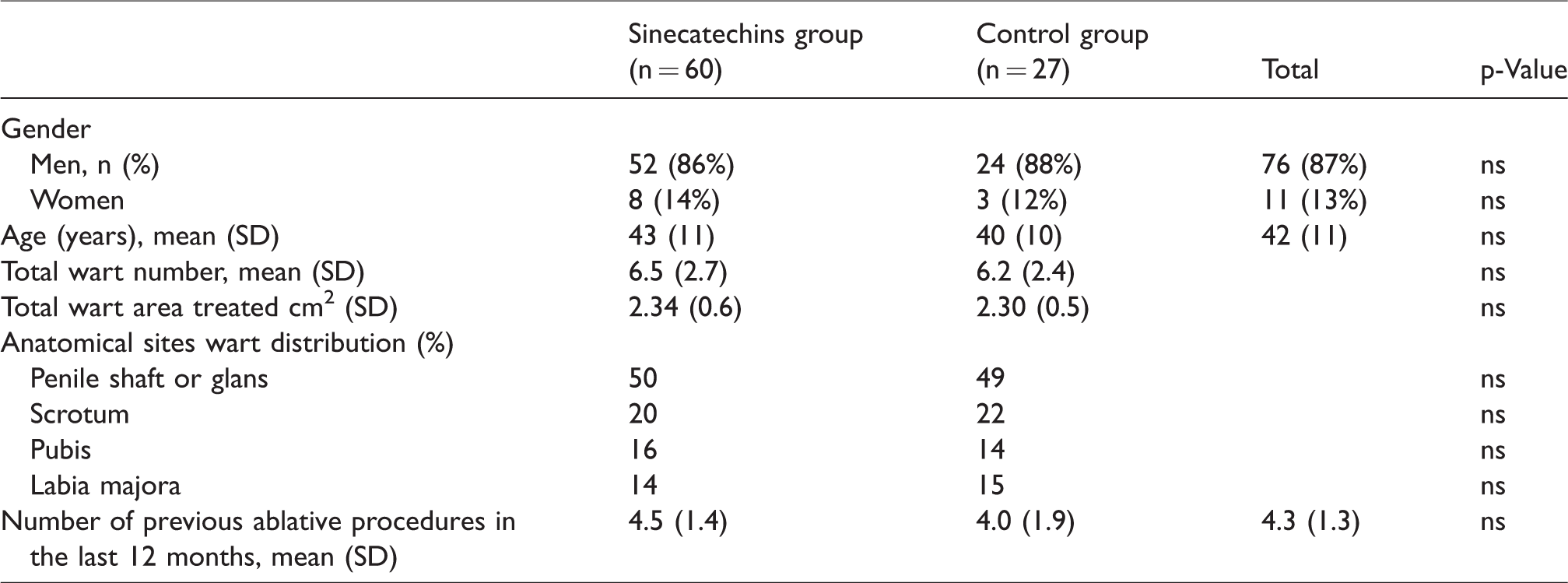
All enrolled patients had a history of two or more ablative treatments in the last 12 months due to recurrent EGW. Table 1 reports the main demographic and clinical characteristics of enrolled subjects (60 in the TS group and 27 in the CTR group) at the baseline visit. The two groups were well balanced for all the variables evaluated. Mean (SD) number of treated lesions at baseline visits was 6.5 (2.6). One subject in the TS dropped out due to burning sensation after the application of the product. Therefore, 86 (98%) subjects completed the study. During the observation period, three subjects in the TS group presented new EGW lesions on treated sites (RR: 5%). In the CTR group, eight subjects presented new EGW lesions on treated sites (RR: 29%) (p = 0.0024; OR: 0.16; 95%CI: 0.04–0.68) (Table 2). In the TS group, 34 subjects (55%) reported mild to moderate erythema or burning sensation at the application site. Figure 1 shows a subject in the sinecatechin group before CO2 therapy and after sinecatechins therapy with no recurrence at month 6. Figure 2 shows a subject in the control group with recurrence after CO2 therapy.
Baseline characteristics of enrolled subjects.
Primary outcome: recurrence rate of EGW during the three-month observational period.

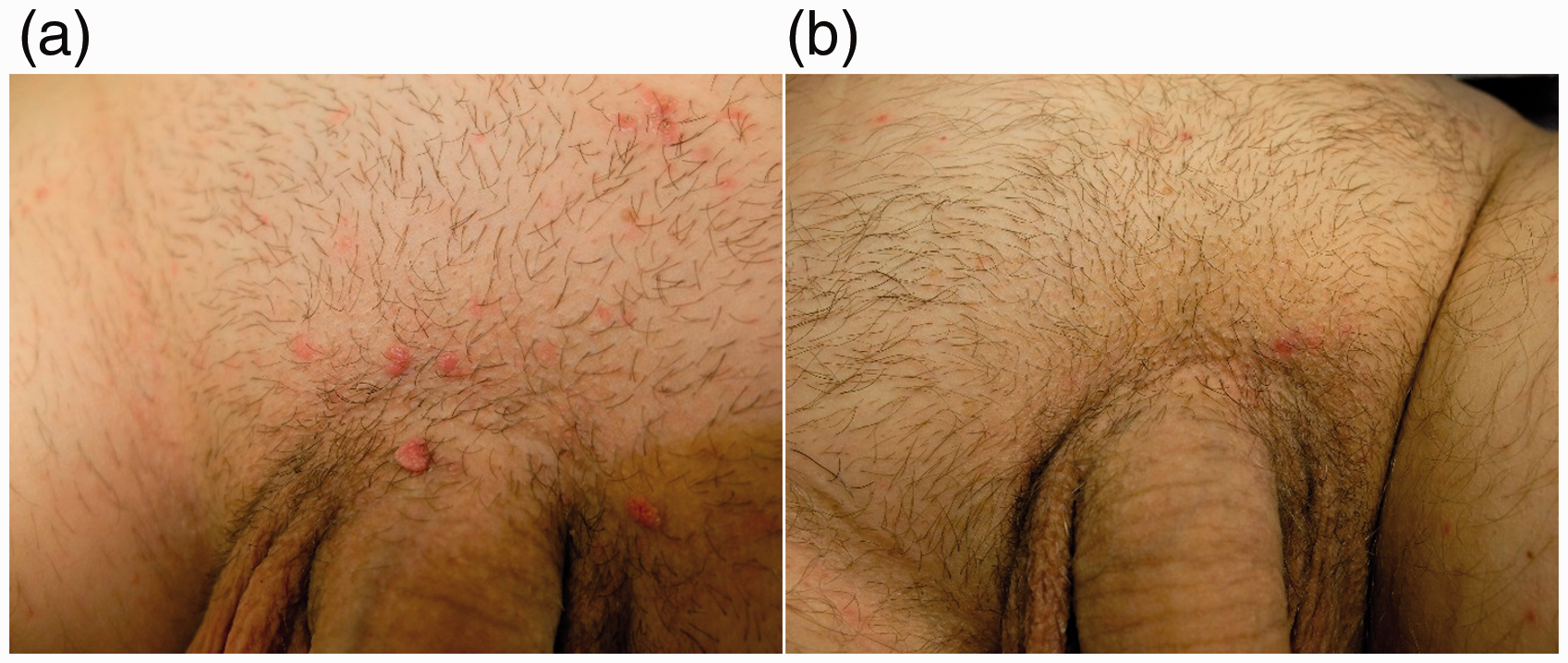
Subject in the sinecatechins 10% group with multiple pubic condylomata: (a) at baseline and (b) no recurrence after CO2 laser at month 6.
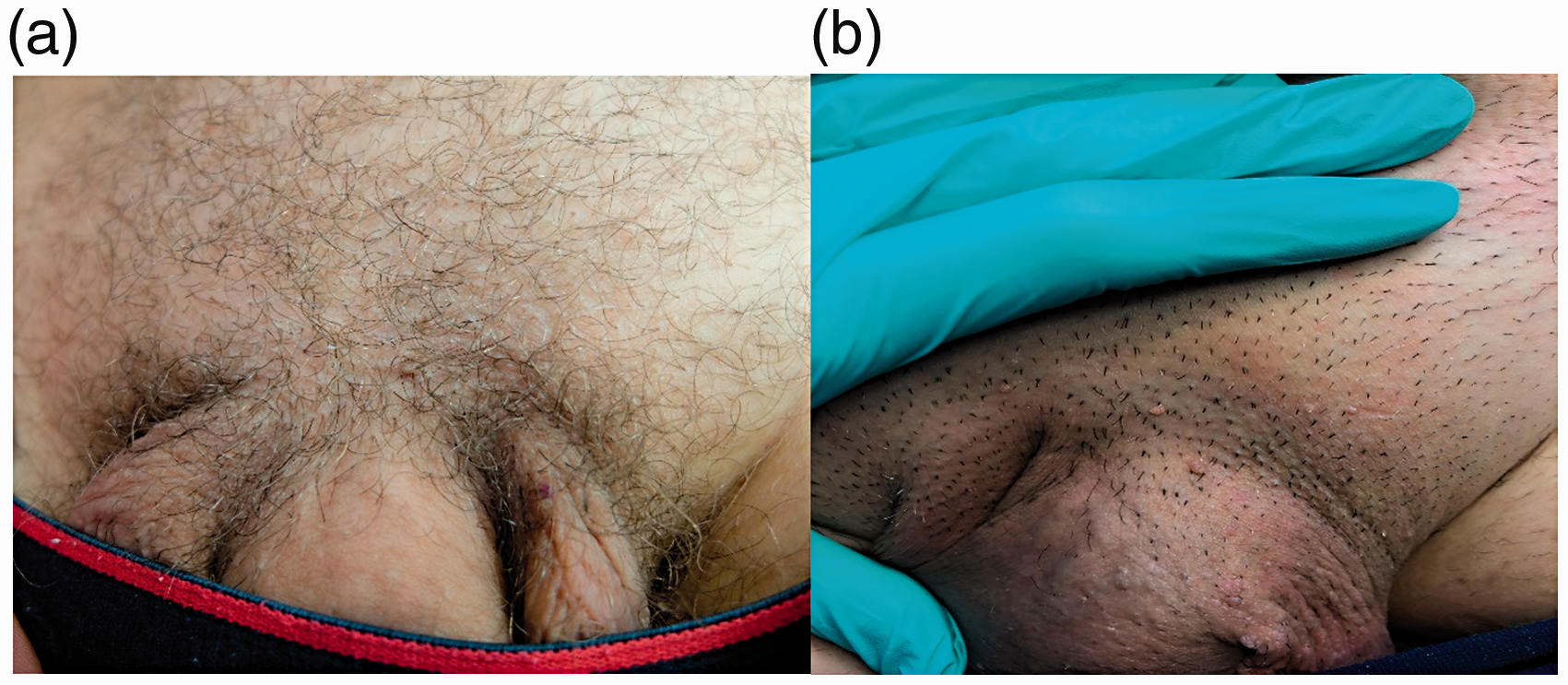
Subject in the control group with pubic condyloma: (a) at baseline and (b) recurrence after CO2 laser.
Discussion
Several treatments (both physician- or patient-applied) for EGW are available, but there is not an ideal approach. 17 Treatments for EGW are often frustrating for both clinicians and patients. 18 Destructive therapies, cryotherapy, curettage, or laser, are in general painful and sometimes unsuccessful. 18 Furthermore, EGW commonly recur after successful therapy. 19 Recurring HPV infection is a complex phenomenon probably involving different mechanisms (auto-inoculation, reactivation of latent infections, lack of homologous immunity, etc.). 19 An RR at three months after cryotherapy up to 40% of treated subjects has been reported. 20 After CO2 laser treatment, Yanofsky et al. 21 reported that EGW RR after CO2 laser session was up to 77%. However, another study by Padilla-Ailhaud 22 showed that the RR after CO2 laser after six months of treatment was up to 25%, a percentage comparable to the RR we observed in the control group in the present study. After sinecatechins treatment, the reported RR at three months was between 7% and 12%.12,13 Epigallocatechin gallate (EGCG), the main component of green tea extract, has shown anti-viral activities against HPV. 23 EGCG has potent anti-inflammatory, anti-oxidant, and pro-apoptotic actions. 24 These mechanisms could explain its anti-viral properties. 25 In the two pivotal trials conducted to assess the efficacy of green tea extract in the treatment of EGW, RR during the three-month follow-up occurred in a very small number of patients (less than 5%).26,27 In a retrospective trial, Juhl et al. 28 have evaluated the efficacy of combined treatment of EGW with cryotherapy, podophyllin and post-ablative immunomodulation with sinecatechins 15% ointment. The initial complete clearance rate was 96%, with an RR at six months of 7.4%. In our prospective trial, we evaluated the efficacy of green tea extract as PST after CO2 laser to assess if this approach could reduce the RR of new lesions in the treated sites. The results of the present study support the fact that the use of green tea extract as PST is associated with a lower RR in comparison with the subjects treated with laser CO2 without PST. Some study limitations should be taken into account evaluating the study results. First, this was not a double-blind trial. However, to increase the internal validity of the trial, we performed an assessor-blinded evaluation of the primary outcome (the RR of EGW lesions). A second aspect was the relatively short period of study treatment (three months). However, the major burden of recurrence lesions after both patient- or provider-applied EGW treatment strategies is observed in this period. 29 Finally, our results could be applied only to subjects treated with CO2 laser, not to other ablative treatments like cryotherapy or electrodesiccation. Specific trials are warranted to evaluate if green tea extract could be effective in reducing recurrent lesions after these kinds of treatments. In this trial, sinecatechins 10% ointment was applied twice daily. In the treatment of EGW, this product is commonly used with a daily three-application schedule. However, recently de Vries et al., 30 using the adhesive tape stripping method, have shown that after topical application of sinecatechins 10% significant amount of the active substance is detected in the skin at 12 h. No significant difference in EGCG concentrations was found after 8 and 12 h. These data, therefore, support the rationale of twice-daily administration.
Conclusion
In this prospective randomized multicenter trial, the use of TS 10% as PST after CO2 laser ablative treatment was associated with a lower RR of new EGW lesions in the short term in comparison with the control group with an OR of 0.16. Comparative larger trials are warranted to evaluate the role of this approach as PST.
Footnotes
Authors’ contributions
MP, EC, GM, LB, IL participated in study design, data collection, data analysis and interpretation, development, review, and final approval of the manuscript. MM participated in data collection and analysis, study design, review, and final approval of the manuscript.
Acknowledgments
This study was a non-profit trial. MM is an employee of Cantabria Labs Difa Cooper, the company selling the study product. Cantabria Labs Difa Cooper supplied the participating centers with green tea extract (Veregen® ointment).
Ethics approval and consent to participate
This study was conducted in compliance with the ethical principles originating in or derived from the Declaration of Helsinki and in accordance with Good Clinical Practice Guidelines. All patients provided signed informed consent. The study protocol was approved in July 2017 by Institutional Review Board of the Coordinating Center (Tor Vergata University, Rome).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.