
Abstract
Socioeconomic status (SES) appears to have positive and negative associations with sexually transmitted infection (STI) risk in resource-limited settings, but few studies have evaluated nationally representative data. We assessed multiple SES measures and their effect on STI risk. We conducted a secondary analysis of data from the Uganda Demographic and Health Survey (UDHS 2011). The primary outcome (STI risk) was self-reported STIs and/or symptoms in the prior 12 months. We examined associations between multiple SES measures and STI risk using a mixed-effects Poisson regression model. The results showed that of the 9256 sexually active individuals, 7428 women and 1828 men were included in the analysis. At an individual level, middle wealth quintile and disposable income were associated with STI risk, whereas being in the richest wealth quintile was protective. Residence in wealthier regions (adjusted incidence rate ratio [aIRR] 3.92, 3.62, and 2.75, for Central, Western, and Eastern regions; p < 0.01) was associated with increased STI risk. Regional level analysis revealed stochastic variability of STI risk across geographical region (variance 0.03; p = 0.01). The bilateral association between SES and STI risk underscores the need for multi-sectoral interventions to address the upstream effects of poverty on STI risk and downstream effects of STIs on health and economic productivity.
Keywords
Introduction
Sexually transmitted infections (STIs) constitute a considerable health and economic burden in resource-limited settings, where 75–85% of the estimated 357 million annual new cases of curable STIs occur. 1 Approximately 17% of economic losses are due to STIs and occur because of ill health, expenditure on health care visits, and substantial productivity losses particularly among adolescents, young adults, and pregnant women. 2 Up to 70% of the female infertility burden is due to STIs acquired from husbands or regular partners. 3 Persons who contract STIs are at higher risk for re-infection and acquiring non-HIV STIs, which increases the risk of HIV acquisition. 4 Among reproductive age women, STIs are a leading cause of disability adjusted life years (DALYs) lost. 5 The economic and health burden of STIs is largely preventable through available evidence-based strategies, including increasing community awareness about risks of STIs and prevention strategies, including treatment. 5
Socioeconomic status (SES) appears to have differing effects on STI risk in various settings. A study of young adults in the United States found a negative gradient of STI risk with increasing income within all racial/ethnic categories, and this effect was stronger for non-whites. 6 In this setting, lower maternal education and nonprofessional maternal occupations were associated with higher STI reports in all groups except white females. 7 In contrast, other studies have reported increased STI risk among higher socioeconomic strata. A nationally representative study in Malawi found that urban female youth in the richer wealth quintile were more likely to engage in multiple sexual relationships and acquire STIs. 8 In this study, women from households in the middle and second richest wealth quintiles were at highest risk of HIV and other STI infection compared to the poorest. 9
Uganda has a persistently high STI burden with up to 1.5 million cases reported annually between 2015 and 2017. 10 High STI incidence, complications, sequelae, socioeconomic impact, and increased risk of HIV acquisition and transmission make STI control a public health priority. The relationship between SES and STI risk has been assessed in prior studies, 11 but few have evaluated nationally representative data.8,12–14 To inform the implementation of effective public health interventions, we evaluated multiple SES measures and their effect on STI prevalence among sexually active women and men who participated in the 2011 Uganda Demographic and Health Survey (UDHS).
Methods
Subjects and setting
We analyzed secondary data from UDHS 2011, a nationally representative survey of 9033 households in the Central, Eastern, Northern, and Western regions, as previously described. 15 A total of 10,969 individuals (8674 females aged 15–49 years and 2295 males aged 15–54 years) were successfully interviewed. The UDHS sample was selected in two stages: first, 404 enumeration areas (EAs) were selected from among a list of clusters sampled for the 2010 Uganda National Household Survey (UNHS). In the second stage of sampling, households in each cluster were purposively selected from a complete listing of households, which was updated prior to the survey.
Inclusion criteria
For the present analysis, we excluded from the original cohort of 10,969 individuals, respondents aged less than 18 (n = 103) or greater than 49 years (n = 1610); the key 18–49 age category is widely used in health research, and restricting our analysis cohort to this age demographic improves the comparability of our findings. The remaining 9256 sexually active men and women aged 18–49 years were included in the analysis (Figure 1).
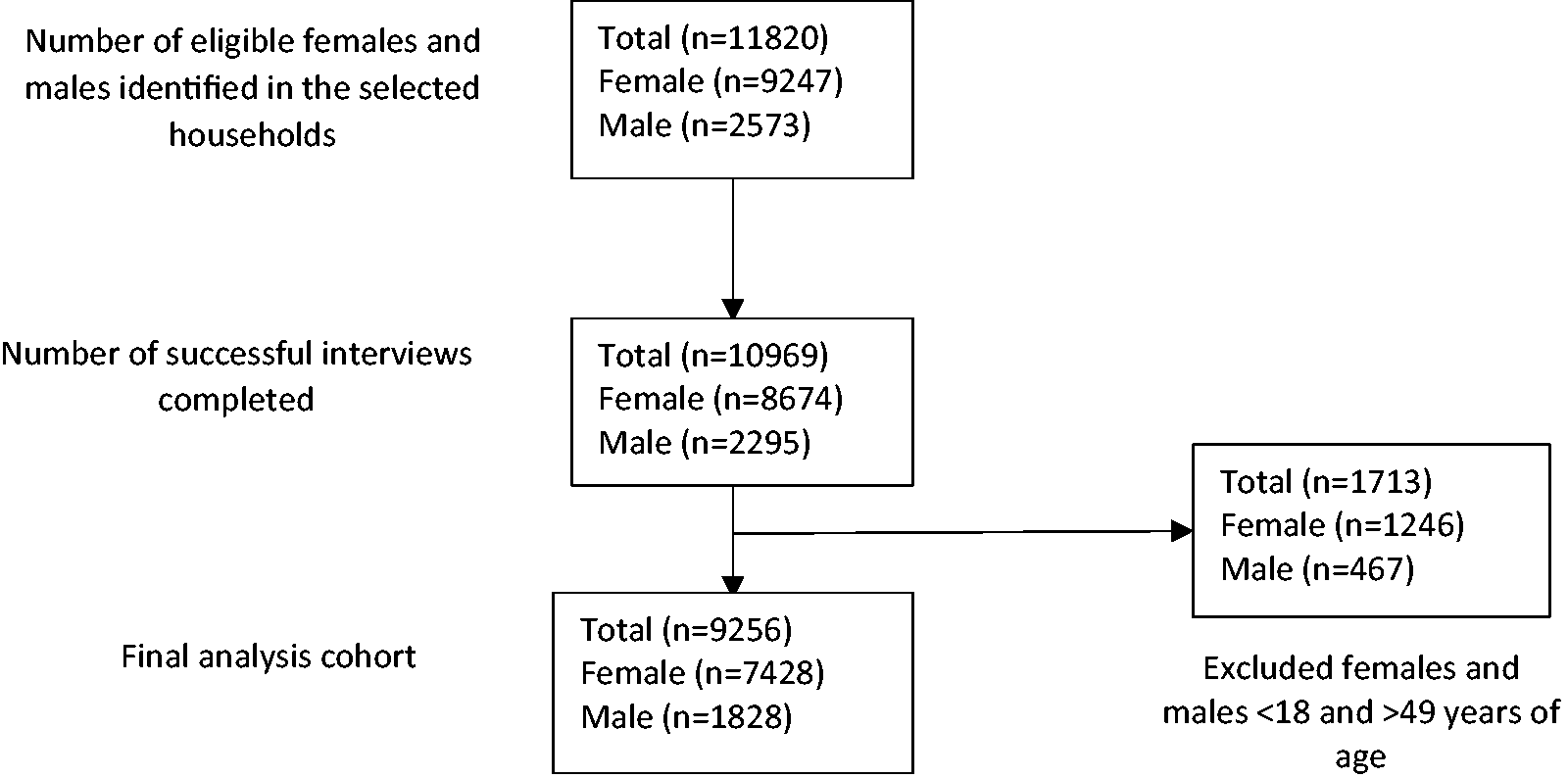
Flow diagram.
Data extraction and outcome definition
Information about history of STIs including genital discharge, sores, or ulcers in the prior 12 months was obtained from the survey questionnaire. We defined the primary outcome as self-reported STI(s) and/or symptoms in the 12 months preceding the survey. This composite outcome was generated by merging three variables: self-report of an STI, genital discharge, or genital sores/ulcers in the 12 months preceding the survey. Respondents who did not report having an STI, but reported genital discharge or genital sores/ulcers, were classified as having symptoms of an STI.
Statistical analysis
We evaluated multiple SES measures including wealth index (poorest, poorer, middle, richer, or richest), type of employment (occasional, seasonal, permanent), and type of earnings (none, cash, in-kind or cash and in-kind). Participant characteristics were described using frequencies and percentages. To examine bivariate associations, proportions and Pearson Chi-square tests were used to evaluate socioeconomic disparities across geographic regions. First, we fit a log-binomial regression model to evaluate the effect of SES on STI risk, and to estimate rate ratios, but this failed to converge. Therefore, we opted for a modified Poisson regression model. 16 Mixed-effects Poisson regression models with robust variances were used to estimate incidence rate ratios at 95% confidence intervals; rate ratios closely approximate risk ratios when the outcome is common.17,18 The mixed-effects modeling approach accounted for correlation of STI risk among individuals within the same region. We performed a sensitivity analysis to examine the relevance of the mixed-effects approach by comparing models without a random component (fixed-effect model) against that with random component (mixed-effects model) at three levels (region–household–individual) and two levels (region–individual, household–individual), using chi-square likelihood ratio test at 5% level of significance. Further, we assessed whether region and sex modified the effect of wealth index on risk of STIs, since wealth index may vary across individuals living in different regions.19,20 We further examined the confounding effect of other individual characteristics on the relationship between socioeconomic factors and STI risk. Factors examined included age (18–35, 35–45, ≥46 years), gender, marital status (never married, married, widowed, divorced/separated), level of education (none, primary, secondary, higher), number of lifetime sexual partners (one, >1), sexual activity in the four weeks preceding the survey (active, not active). Factors that changed risk estimates by at least 20% were included in the final analysis as confounders. Linear trend effects in STI risk across education levels and wealth quintiles were assessed by fitting models in which each of these factors was entered as a categorical variable, and then as a linear variable. Both models were compared using a likelihood ratio test, and linear trend was assumed if the p-value was not significant at 5% level. All analyses used survey weights to account for unequal sampling probability of selecting participants. Statistical analyses were performed using Stata 14.0 (StataCorp LLC, College Station, TX).
Ethical approval
Written permission to use secondary data from the UDHS was obtained from the Uganda Bureau of Statistics (UBOS). The study was approved by the Scientific Review Committee of the Infectious Diseases Institute, Makerere University.
Results
Population characteristics
Of the 9256 sexually active respondents, 7428 women (mean age 30 years, standard deviation [SD] 8.7) and 1828 men (mean age 31 years, SD 8.6) were included in the analysis (Table 1). The majority (80%) lived in rural communities, and more than half (58%) reported less than secondary education. One in four (26%) participants were in the richest quintile of the wealth index and 18% were in the poorest quintile. Overall, STI prevalence was 23.2%, and was significantly higher in women than men (80.4% vs. 19.6%; p < 0.01). Central region had the highest proportion of people in highest wealth quintile, whereas Northern had the highest proportion in the lowest wealth quintile.
Population characteristics by wealth index.

aPearson’s Chi-square p-values.
Relationship between socioeconomic status and STI prevalence
In unadjusted analyses, we observed strong evidence of a positive association between wealth index and STI risk (p < 0.01 for all comparisons) (Table 1). The association between wealth index and STI risk was not modified by geographical region (test of homogeneity, p = 0.08) or sex (test of homogeneity, p = 0.45).
In adjusted analyses at individual level, being in the richest wealth quintile was associated with a 14% lower risk of STIs (adjusted incidence rate ratio [aIRR] 0.86; 95% CI: 0.75–0.97; p = 0.02). The middle wealth quintile was associated with higher STI risk compared with the poorest quintile (aIRR 1.17; 95% CI: 1.02–1.34; p = 0.03) (Table 2). The STI rate in Central, Western, and Eastern regions was 3.92, 3.62, and 2.75 times the rate of Northern region, respectively (p < 0.01 for all comparisons). Among employees, payment in cash (aIRR 1.30; 95% CI: 1.15–1.47; p < 0.01), in kind (aIRR 1.47; 95% CI: 1.14–1.90; p < 0.01), or both (aIRR 1.32; 95% CI: 1.13–1.54; p < 0.01) were associated with higher STI risk. Having multiple lifetime sexual partners and sexual activity in the four weeks prior to the survey were associated with higher risk of STI (aIRR 1.49; 95% CI: 1.35–1.65, and aIRR 1.23; 95% CI: 1.17–1.28, respectively). In contrast, older age (>46 years) was associated with reduced risk of STIs (aIRR 0.74; 95% CI: 0.62–0.89; p < 0.01). We observed declining STI risk with increase in the educational level attained (test for no departure from linear trend, p = 0.13). At regional level analyses, there was stochastic variability of STI prevalence across geographical regions (variance = 0.03; 95% CI: 0.03 (0.00–0.34); p = 0.01).
Associations of socioeconomic status measures and STI risk.
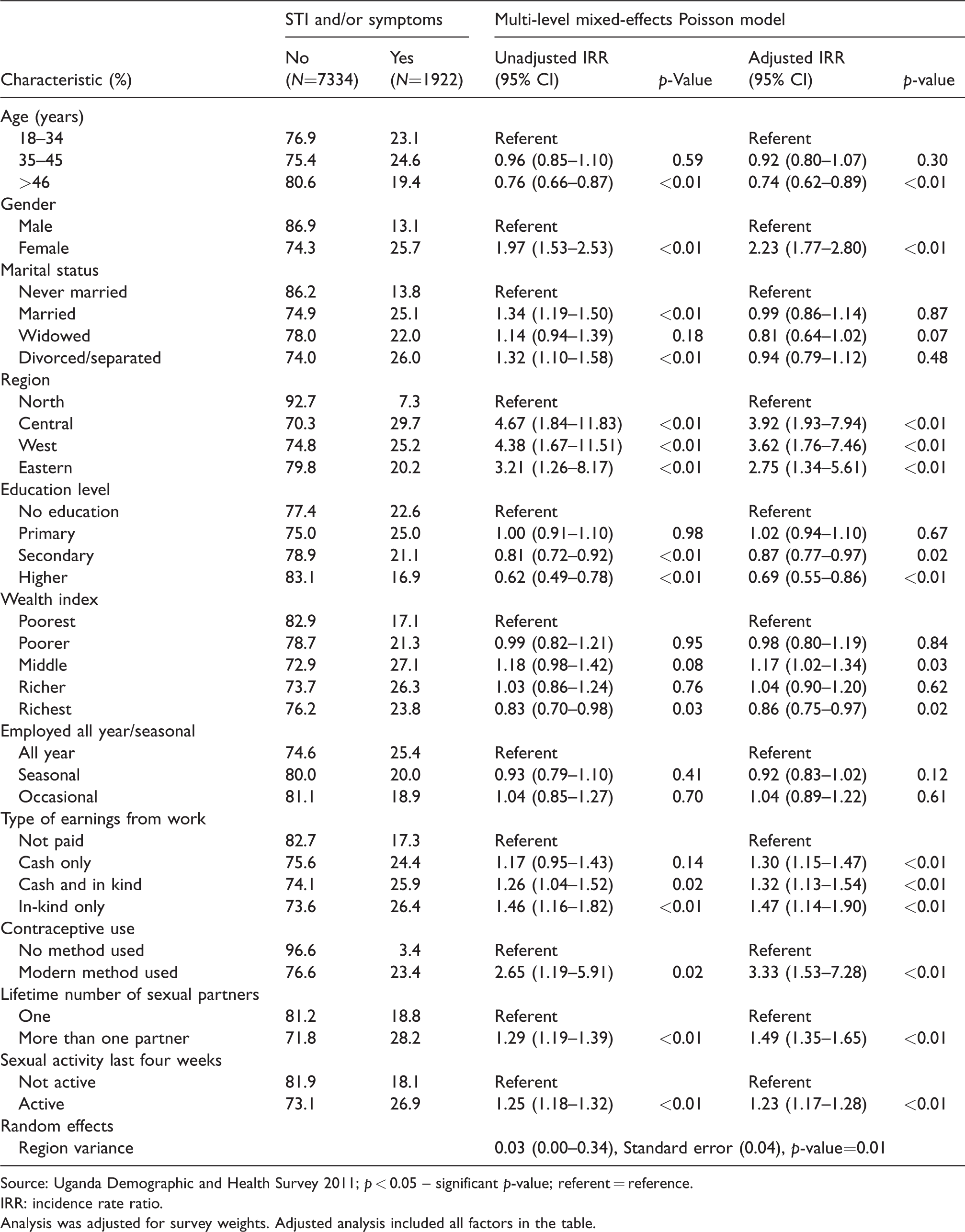
Source: Uganda Demographic and Health Survey 2011; p < 0.05 – significant p-value; referent = reference.
IRR: incidence rate ratio.
Analysis was adjusted for survey weights. Adjusted analysis included all factors in the table.
In sensitivity analyses of all 10,969 UDHS participants including those aged 15–17 years (n = 1610) and 50–54 years (n = 103), our findings were similar to the primary analysis. Middle wealth quintile (aIRR 1.16; 95% CI: 1.01–1.34; p = 0.04) and disposable income (aIRR 1.32; 95% CI: 1.11–1.57; p < 0.01) were associated with STI risk, whereas being in the richest wealth quintile was protective (aIRR 0.83; 95% CI: 0.73–0.95; p < 0.01). Residence in wealthier regions (aIRR 3.77, 3.47, and 2.59, for Central, Western, and Eastern regions; p < 0.01 for all comparisons) was associated with increased STI risk. In sub-group analyses, STI risk was not significantly different across age groups: 18–49 (p = 0.09), 35–49 (p = 0.30), and 50–54 (p = 0.29), respectively, compared with 15–17. Similar results were obtained for ages 18–49 (p = 0.10) and ages 50–54 (p = 0.33) compared with age 15–17.
Discussion
In this nationally representative study of sexually active women and men in Uganda, there was a bilateral relationship between SES measures and STI risk. We observed a negative association between STI risk and older age, any educational attainment and being in the richest wealth index quintile, and a positive association between STI risk and female gender, residence in wealthier geographical regions, availability of disposable income, sexual activity in the prior month, having multiple sexual partners and being in the middle wealth quintile. There was no association between type of employment and STI risk. These findings suggest that targeted interventions could increase access to care and decrease STI transmission in Uganda.
Our finding that middle and higher SES, as measured by wealth index quintile, had inverse effects on STI risk with middle SES posing the highest risk and higher SES being protective is in agreement with previous studies. SES appears to have a bilateral effect on STI risk: the upstream effect of poverty may lead to age-disparate or transactional sexual relationships, a vulnerability exacerbated by limited access to health care, while the downstream effect of STIs on household productivity and health care expenditure exacerbates poverty.21,22 Studies from India have reported that female sex workers without financial autonomy and women from poor economic strata were more likely to have STIs.3,23 Other work has found that urban females in the richer wealth quintile were more likely to report multiple sexual partnerships, and had higher risk of HIV and other STIs.8,9 In our study, availability of disposable income was associated with higher risk of STIs. Access to economic resources may facilitate mobility, access to social networks, and multiple sexual partnerships, factors that increase STI risk. 24 Multi-sectoral interventions in resource-limited settings should address the upstream effects of poverty on STI risk and downstream effects of STIs on health and economic productivity.
We found that longer duration of schooling was protective against STIs. A meta-analysis of 27 studies from resource-limited settings showed that higher educational attainment is often associated with increased HIV risk particularly in older cohorts and rural areas, and this risk was similar in women and men. 25 The association between higher education and reduced STI/HIV risk8,26–28 could be mediated through safer sexual behaviors, suggesting education may act as a “social vaccine”. 29 However, a Cochrane review of eight cluster randomized trials that enrolled 55,157 participants found little evidence that school-based sexual and reproductive health programs are effective in reducing STI prevalence among adolescents. 30 Keeping young women in school decreases STI risk. 27 Comprehensive prevention interventions should include incentives to promote school attendance.
The strengths of our study include the use of data from a large nationally representative survey, the large sample size providing statistical power to evaluate confounding and STI risk estimates, and use of multiple SES measures. Our study has limitations. We utilized secondary data from a cross-sectional population based survey, enabling assessment of correlations but not causality. Respondents may have had difficulty remembering previous exposures, and/or their recollection may have been biased by having had the outcome (recall bias). We relied on self-report of sexual behaviors and STI diagnoses, which may have been underreported because some STIs are asymptomatic. However, self-report is the standard method of collecting STI and sexual behavioral data. We performed a complete case analysis on secondary data and had no control over data quality. Data on high-risk groups (sex workers, truck drivers) and information about STI treatment that would have informed our findings were not available. Although it is likely that there were missing data, the large sample size provides sufficient power to evaluate the research question.
In conclusion, regional and individual SES measures had inverse effects on STI risk among sexually active women and men in Uganda. Residence in wealthier regions, female gender, and availability of disposable economic resources acquired through employment, may convey the highest risk, whereas being in the richest wealth quintile, older age, and any educational attainment were protective. Future studies should use multiple measures of SES in relation to STI risk, and investigate the effects of within-region and within-country disparities in order to elucidate the complexity of the SES and STI relationship.
In view of the World Health Organization goal to end STI epidemics as major public health concerns, and achieve a 90% decrease in curable STIs incidence by 2030, governments should increase investment in the STI response, focus resources on wealthier geographical regions and high risk populations with the greatest need (e.g. migrant laborers, middle wealth quintiles), integrate STI care with other health services, and adopt a multi-sectoral policy approach.
Footnotes
Acknowledgements
The authors are grateful to the respondents of the 2011–2012 Uganda Demographic and Health Survey (DHS) for their participation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Mentorship support for manuscript writing was provided by Fogarty International Center, National Institutes of Health (grants #D43TW009771 “HIV co-infections in Uganda: TB, Cryptococcus, and Viral Hepatitis” and K43 TW010695).