
Abstract
The incidence of penile squamous cell carcinoma (SCC) varies widely in different parts of the world. It is rare in Western countries but common in developing countries like India. The glans and foreskin are the most commonly affected sites. It can occur in two forms which have different evolution and prognosis. Exophytic papillary lesions have late and rare lymphatic spread and ulcero-infiltrating lesions are associated with rapid lymph node invasion and a poorer prognosis. Human immunodeficiency virus (HIV) is an aggravating factor for penile cancer and accelerates the progression of the disease. Cutaneous metastasis from penile SCC is rarely reported. Here, we report a case of metastatic SCC of the penis in a 51-year-old HIV-infected man who presented with cutaneous metastases in the inguino-pubic region with a hidden penile SCC.
Introduction
A higher incidence of penile squamous cell carcinoma (SCC) in developing countries can be attributed to poor hygiene. Other risk factors include old age, lack of circumcision, sexual risks (multiple sexual partners), phimosis, human papillomavirus (HPV) 16 and 18 infection, chronic inflammation, smoking and psoralen plus ultraviolet A phototherapy. 1 Lichen sclerosus appears to be an additional precursor in a subset of penile SCC. Circumcision done in the perinatal period gives protection against penile carcinoma. The two most common locations for penile SCC are the glans (48% of cases) and the foreskin (21% of cases).
Penile cancer assocaited wtih HPV infection and malignant tumours of soft tissue are more frequent in HIV-infected patients. They usually metastasize to regional lymphatics, initially to the superficial inguinal lymph nodes followed by dissemination to deep inguinal and pelvic lymph nodes, while distant metastases via the haematogenous route are rare. Cutaneous metastasis from penile SCC is very rare.
Case report
A 51-year-old uncircumcised, heterosexual widower presented with multiple nodulo-ulcerative lesions over the inguinal and pubic areas of two months' duration. The lesions were painful and associated with foul-smelling purulent discharge of two weeks' duration for which he had undergone incision and drainage one week prior to presentation. The patient had been diagnosed with HIV infection three years previously and was on antiretroviral therapy (zidovudine, lamivudine and nevirapine) since then.
The lesions started as asymptomatic small nodules over the right inguinal area, and gradually increased in size and number. They subsequently ulcerated and developed yellowish foul-smelling discharge. There was history of phimosis of two months' duration but it was not associated with difficulty in micturition. The man gave a history of unprotected penovaginal intercourse on many occasions with different partners. The patient had no other comorbidities or addictions.
Cutaneous examination revealed multiple well-defined erythematous nodulo-ulcerative lesions ranging in size from 0.5 cm to 2 cm with the largest ulcer being of size 8 cm × 5 cm in the right groin. A few nodules coalesced to form plaques with foul-smelling pus and blood discharging from them with features of a buried penis. The skin over the right inguino-scrotal area was indurated, adherent to the underlying inguinal lymph nodes. Diffuse ill-defined induration was also present over the pubic area and right thigh (Figure 1(a) and (b)).
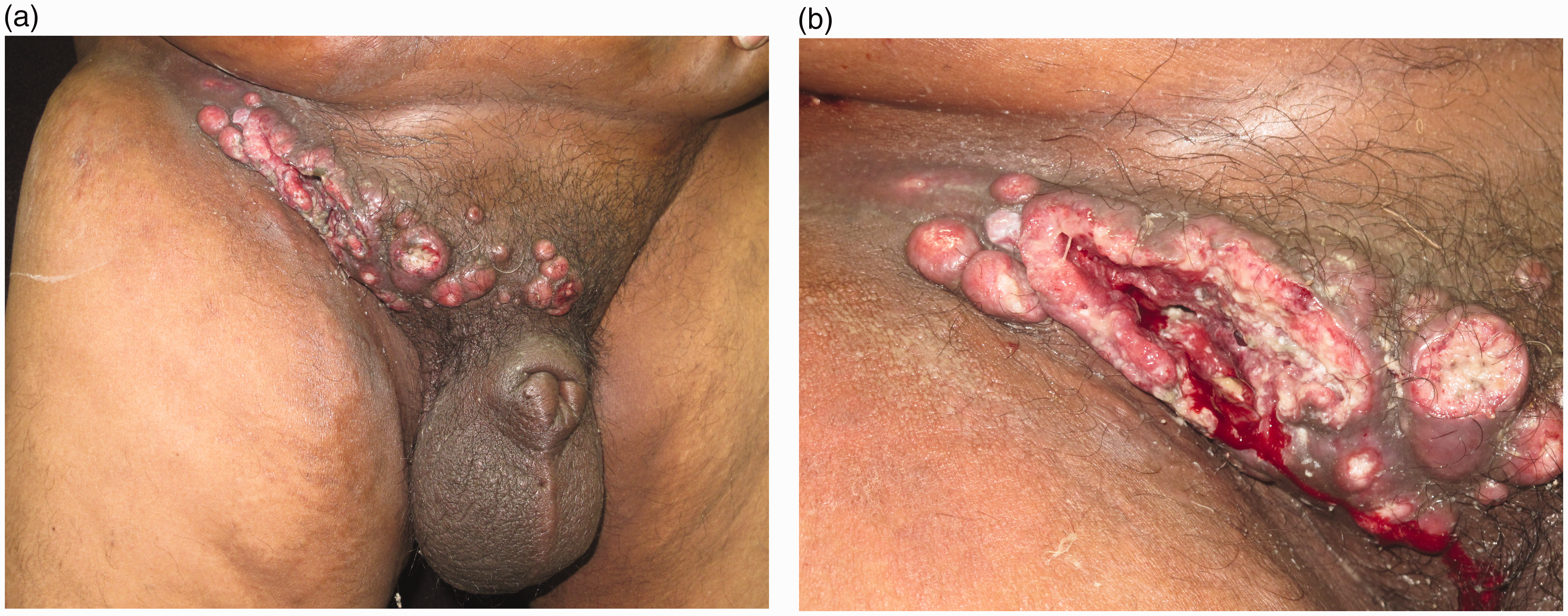
(a) Multiple well-defined erythematous nodulo-ulcerative lesions in the right inguino-pubic area discharging yellowish-grey material with features of a buried penis. Skin over the right inguinal area was indurated, adherent to underlying inguinal lymph nodes. Diffuse ill-defined erythema and induration were also present over the right pubic area and right thigh. (b) Large indurated ulcer discharging yellowish-grey material and blood, surrounded by nodular lesions.
Differential diagnoses of SCC and deep fungal infection were considered. Histopathologic examination revealed acanthosis and elongated rete ridges and a mass in the dermis which was separated from epidermis by a normal dermis. The tumour mass consisting of multiple horn pearls and atypical squamous cells was suggestive of a cutaneous metastasis from a cryptic SCC (Figure 2(a) to (d)). The patient's CD4 cell count at the time of presentation was 312 cells/mm3.

(a) Histopathology: acanthotic epidermis, dilated lymphatics and a mass in the dermis which was separated from epidermis by a normal dermis. The tumour mass consists of multiple horn pearls and atypical squamous cells (H&E, 40×). (b) Acanthotic epidermis, dilated lymphatics and collection of multiple horn pearls and atypical keratinocytes in the dermis (H&E, 100×). (c) Multiple horn pearls in the dermis surrounded by atypical keratinocytes (H&E, 100×). (d) Horn pearls (H&E, 400×).Hematoxylin & Eosin (H & E) stain.
Fluorodeoxyglucose whole body positron emission tomography (PET) scan revealed hypermetabolic disease in two discrete lesions involving the penis, which appeared to be the likely site of primary malignancy. Metastatic scrotal deposits were also seen. Active disease was noted in the large ill-defined ulcerproliferative lesion in the right inguinal region with involvement of the skin. Metastatic inguino-pelvic lymphadenopathy and multiple bilateral lung lesions were noted.
The patient underwent palliative chemotherapy consisting of paclitaxel and carboplatin injections and oral aprepitant. Unfortunately, the patient died following two cycles of chemotherapy.
Discussion
The incidence of penile SCC varies from 0.02% to 20% in different parts of the world. 2 It is more common in developing countries like India. Circumcision done in the neonatal period has a preventive role as it decreases the risk of penile SCC by 3–5 fold, probably by improving local hygiene. It has been theorised that the neonatal glans exposed at circumcision may acquire a protective layer of cutaneous cornification that does not appear after delayed circumcision. 3 In an uncircumcised male, SCC frequency increases due to retention of smegma and carcinogenic agents within the preputial sac. HPV DNA, particularly HPV16 and 18, has been associated with invasive carcinoma of the penis.3,4
Patients who are HIV infected have a two-fold higher risk of developing malignant tumours. 5 Penile cancer due to HPV infection and malignant tumours of soft tissue are more frequent in HIV-infected patients.
Penile SCC may present as an exophytic growth, ulcerated nodule, or flat ulcer with pruritus, burning, pain, discharge, bleeding or foul odour. Approximately 50% of patients have regional lymph node metastasis at the time of presentation but only half of these patients have nodal metastasis. 6 Local metastasis of penile carcinoma occurs primarily by lymphatics, initially to the superficial inguinal lymph nodes followed by dissemination to deep inguinal and pelvic lymph nodes.
Distant metastases via the hematogenous route are rare, accounting for 1–3% cases, as Buck’s fascia acts as a protective barrier against vascular invasion. 7 Distant metastases usually deposit in lungs, liver, bone and brain. 8
Diagnosis can be made by biopsy of the primary lesion or by lymph node biopsy. Radiological imaging should be conducted to determine the extent and stage of penile SCC. It is the standard method to detect subclinical nodal spread. These may be achieved by ultrasound, computed tomography, magnetic resonance imaging and PET.
Cutaneous metastasis from penile carcinoma is extremely rare. In the few reported cases, it has been described as multiple nodular swellings present discretely all over the body. It was reported simultaneously with the primary disease 8 and also after nine months of treatment of primary disease. 9 In our patient, cutaneous metastases were localized to inguinal and pubic area as nodulo-ulcerative lesions but the primary malignancy of the penis was hidden due to a buried penis. Another presentation of cutaneous metastasis of penile SCC was carcinoma en cuirasse. 10
Metastatic SCC can be differentiated from primary SCC of skin by the presence predominantly of metastatic lesions in the dermis or subcutaneous tissues. The overlying epidermis tends to show only reactive features or be ulcerated by the growth of the subjacent tumour. 11
Prognosis of penile SCC with metastases in HIV-positive patients depends on the stage of presentation and should be treated aggressively. Treatment of penile carcinoma remains difficult due to its aggressive nature and a paucity of data. Some patients have responded to combination chemotherapy with methotrexate, bleomycin and cisplatin with a response rate of 72% and median response duration of six months. 12
Summary
The pathogenesis of malignant tumours linked to HIV infection is poorly understood. Risk of developing a malignant tumour is higher in subjects infected with HIV than in the general population. Certain cancers like Kaposi’s sarcoma, early malignant non-Hodgkin’s lymphoma (MNHL) of the central nervous system, systemic MNHL and invasive cancer of the cervix are already reported in association with acquired immune deficiency syndrome. 13 Cutaneous metastasis from penile carcinoma can present as nodulo-ulcerative lesions involving inguinal, pubic and scrotal areas. In our patient, penile carcinoma was not visible as the penis was buried inside the prepuce and the cutaneous manifestations were the only clinical presentation.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.