
Abstract
Gonorrhea is one of the most common sexually transmitted infections (STIs). In a minority of cases, a disseminated infection can occur including gonococcal osteoarticular disease. With the steep and sustained increase in STIs in the US, we could see invasive gonococcal disease more often. Most cases of gonococcal osteomyelitis receive prolonged courses of antibiotic therapy. We report here the successful treatment of gonococcal osteomyelitis with one week of antibiotic therapy. Given the emergence of bacterial resistance worldwide and associated side effects, it is crucial to limit antibiotic exposures to the smallest effective dose possible.
Introduction
The CDC has observed a steep and sustained increase in sexually transmitted infections (STIs) in the US reaching 20.3 million cases in 2017. 1 Disseminated gonococcal infection (DGI), gonococcal arthritis and osteomyelitis are infrequent complications of gonococcal infection. 2 The recommended duration of treatment for an invasive gonococcal osteoarticular disease is at least three to four weeks of antibiotic therapy.3,4 However, there is scarcity of information regarding the optimal treatment duration. We report a case of gonococcal osteomyelitis managed successfully with one week of antibiotic therapy. This case highlights the importance of enforcing optimal duration of therapy for gonococcal osteoarticular disease, decreasing exposure time to unnecessary antibiotics, which in turn decreases the risk of developing resistance and facilitates antibiotic stewardship.
Case report
A 37-year-old man with a medical history of Graves’ disease treated with radioiodine ablation (2013) and traumatic fracture to the right fifth metatarsal with right metatarsal fixation (March 2017) presented to our emergency department (ED) on October 2017 with acute onset of right foot pain and swelling (Figure 1(a)) after falling while walking to the grocery store three days prior. On presentation, he was febrile. The white blood cell (WBC) count was 12.2 × 109/L, with 74.9% segmented neutrophils and 0.4% immature granulocytes. The erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were 96 mm/h and 66.1 mg/L, respectively. He tested negative for hepatitis C, HIV-1 and 2, and syphilis. His right foot abscess was incised and drained. Magnetic resonance imagining (MRI) revealed cellulitis along the dorsal right foot and osteomyelitis of the distal cuboid and proximal base of the fourth metatarsal and early osteomyelitis of the fifth metatarsal, the site of the previous traumatic fracture (Figure 1(b)). Furthermore, his urine tested positive for Neisseria gonorrhoeae by nucleic acid amplification test (NAAT; Aptima Combo 2® , Hologic Inc., San Diego, CA, USA); but was negative for Chlamydia trachomatis and Trichomonas vaginalis. The patient reported having several days of green-yellow urethral discharge with dysuria following a new sexual relationship 3–4 day prior to admission. The patient received empiric intravenous vancomycin for presumed cellulitis and one dose ceftriaxone 250 mg intramuscularly plus azithromycin 1 g for presumed urethritis. Three days later, he underwent debridement of the right fifth metatarsal. Bone biopsy cultures taken from the site grew N. gonorrhoeae. The patient was discharged home on his sixth day of admission after his ESR and CRP returned to approximately normal values (1 mm/h and 12.2 mg/L, respectively). The patient was arranged to receive at least four weeks of intravenous ceftriaxone 2 g daily at home through a peripherally inserted central catheter (PICC). However, the following day, the home health agency attempted to see the patient at home, but he could not be reached by any means that day and the following days. He did not attend several outpatient appointments. Consequently, the patient received only one week of IV ceftriaxone. He finally came to a follow-up visit with his orthopedic surgeon two weeks later. Examination revealed that the patient had probable complete resolution of his right foot cellulitis and osteomyelitis.
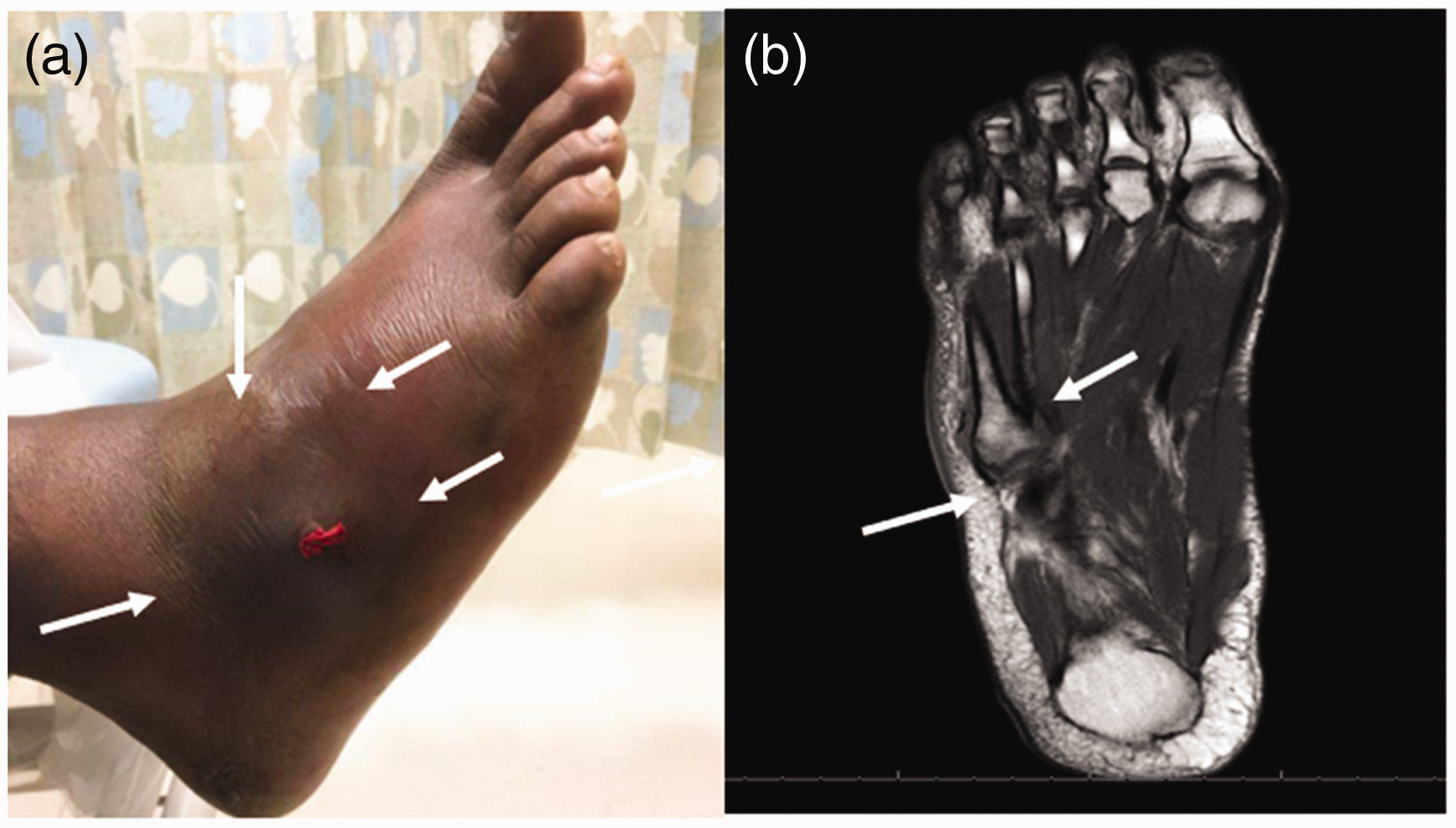
(a) Right foot cellulitis and swelling (arrows). (b) MRI showing osteomyelitis of the fifth metatarsal bone (arrows).
Discussion
Gonorrhea is one of the most common STIs.1,5 In a minority of patients, DGI can arise from an initial mucosal infection. This dissemination may be partly related to deficiencies of serum complement, especially terminal complement deficiencies (C5–8). 6 The main manifestations of DGI are the arthritis-dermatitis syndrome, with polyarthritis or tenosynovitis, oligoarticular septic arthritis, often accompanied with characteristic petechial or pustular skin lesions. Rare manifestations include endocarditis, meningitis and osteomyelitis, which usually represents an extension of septic arthritis.2,7,8 Osteomyelitis is associated with non-gonococcal septic arthritis, but it is unusual in gonococcal arthritis.2,9,10 Black and Cohen hypothesized that osteomyelitis develops due to the delay between the onset of joint symptoms and the administration of antibiotic therapy. 2 Alternatively, osteomyelitis can result from hematogenous spread. Damaged bone is more likely to be seeded from bacteremia compared to intact bone.11,12 Our patient had findings on MRI suggestive of osteomyelitis of the fourth metatarsal and early osteomyelitis of the fifth metatarsal. Given his history of recent traumatic fracture of the fifth metatarsal, our patient may have developed transient bacteremia following symptomatic urethritis that seeded his fifth metatarsal.
Most experts agree on a four-week to six-week course of intravenous antibiotic therapy for osteomyelitis. However, when surgical debridement is employed, the duration of treatment can be shortened. 13 Handsfield et al. 14 argued, more than 40 years ago, for shorter courses of antibiotic therapy. In previous case reports of gonococcal osteomyelitis, patients were given 1–12 months of antibiotic therapy. Not all of the cases fully recovered with treatment.4,10 Our case questions the need for a prolonged duration of therapy for gonococcal osteomyelitis. Given the emergence of antimicrobial resistance worldwide, 15 it has become imperative to use antimicrobials judiciously. Some studies have shown that shorter courses of antibiotics and longer courses have similar outcomes in many infection types.16,17 Shorter courses are cost-effective and are associated with fewer toxicities and better patient adherence.18,19 This isolated case limits our ability to extrapolate our findings to similar cases. In addition, cure was achieved with only one week of antimicrobial therapy probably due to the acute nature of osteomyelitis in our patient. 20 It could also be related to the low antimicrobial resistance in gonococci causing DGI. 21 We need more clinical studies in gonococcal osteomyelitis to determine the ideal duration of therapy.
In summary, clinicians should keep in mind that gonococcal infection can progress to osteomyelitis, either by direct extension from a septic joint or via hematogenous spread. Given the emergence of antibacterial resistance and specifically gonococcal resistance worldwide, it is important to limit antimicrobial use to the lowest effective dose possible. Good clinical practice entails a minimum of four weeks of antibiotic therapy for pyogenic osteomyelitis. However, this duration can be shortened when coupled with optimal surgical debridement and a favorable clinical response.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.