
Abstract
Raltegravir (RAL) is an HIV-1 integrase strand transfer inhibitor that is well established as a component of highly active antiretroviral therapy regimens for the treatment of adults living with human immunodeficiency virus (HIV), due to its high virological efficacy and good tolerability profile. To date, limited data are available on the use of RAL with abacavir/lamivudine (ABC/3TC). We investigated retrospectively 62 HIV-1 infected patients managed by three Italian Infectious Diseases Outpatient Departments, including 57 treatment-experienced patients and 5 treatment-naïve patients, treated with ABC/3TC plus RAL. In all five naïve patients (100%), virological suppression was achieved and maintained , while 55 experienced patients (96.5%) maintained viral suppression at the most recent review. In the treatment-experienced patients, we observed a significant decrease in triglyceride levels (p < 0.01), while liver transaminases, renal function and cholesterol levels remained substantially stable. In the 34 treatment-experienced patients who switched from a protease inhibitor (PI)-based regimen, we observed a significant improvement of total cholesterol (p=0.03) and triglyceride (p < 0.01) levels. No significant alterations were found on renal and liver function and serum lipid profile of treatment-naïve patients. Despite the small number of participants, results support the efficacy and safety of ABC/3TC plus RAL, either in treatment-naïve or treatment-experienced patients.
Keywords
Introduction
International treatment guidelines for adults living with human immunodeficiency virus (HIV) recommend as the first-line antiretroviral therapy (ART) regimen a combination of two nucleoside reverse transcriptase inhibitors (NRTIs) with either a boosted protease inhibitor (PI), an integrase strand transfer inhibitor (INSTI), or a non-nucleoside reverse transcriptase inhibitor (NNRTI).1–3 The need for lifelong ART must lead the physician to consider, in addition to the effectiveness of the drugs, the long-term adverse effects of these drugs, such as lipid metabolism toxicity, mitochondrial toxicity and renal dysfunction. Raltegravir (RAL), an INSTI, was licensed in 2007 in the USA and, subsequently, in 2008 in Europe for treatment-experienced and treatment-naïve subjects living with HIV. RAL has potent in vitro activity against HIV-1, with a 95% inhibitory concentration in human T lymphoid cell cultures of 31 ± 20 nmol/L. Additive to synergistic activity was observed when human T lymphoid cell culture samples infected with the H9IIIB variant of HIV-1 were incubated with RAL and a panel of available nucleoside analogue reverse-transcriptase inhibitors, non-nucleoside reverse-transcriptase inhibitors and PIs. Furthermore, RAL demonstrated a good tolerability profile, particularly regarding lipid and glucose metabolism, and reduced drug interactions compared with other antiretroviral drugs in both treatment-experienced and -naïve subjects; although well tolerated, RAL requires twice-daily dosing and has a lower genetic barrier to resistance compared with dolutegravir (DTG).4,5
Only few data are available on the efficacy and safety of the abacavir/lamivudine (ABC/3TC) plus RAL regimen, either in treatment-naïve or in treatment-experienced patients. The aim of this study was to assess the efficacy of RAL in combination with ABC and 3TC in both virologically-suppressed treatment-experienced subjects and treatment-naïve subjects living with HIV and the metabolic and immunological changes after the start or the switch to this regimen.
Patients and methods
This observational, retrospective, multi-centre study included 62 HIV-1 infected patients followed by Infectious Diseases Outpatient Departments of three medical centres in Italy: G.B. Rossi Hospital in Verona, Azienda Ospedaliera in Padova and Sant’Orsola Hospital in Bologna. Data were collected between January and February 2018. Eligible patients were living with HIV-1, aged ≥18 years, HLA-B5701 negative and had at least one viral load assessment prior to and after the switch or the commencement of ABC/3TC plus RAL. The patients who began ART with ABC/3TC plus RAL constituted the treatment-naïve group, while the patients who began ABC/3TC plus RAL after the discontinuation of another regimen constituted the treatment-experienced group. We collected retrospectively the zenith viral load and CD4+ cell count nadir before the start of ART and the metabolic profile, comprising total, low density lipoprotein (LDL) and high density lipoprotein (HDL) cholesterol, triglycerides, transaminases, creatinine and creatine phosphokinase. These metabolic parameters were collected before the switch or the beginning of ABC/3TC plus RAL. These data were compared with the latest metabolic profile, viral load and CD4+ cell count available. Treatment adherence was measured by self-reported adherence at the time of the visit. Statistical analysis was performed using t-test for paired data, a two-tailed p-value of <0.05 was considered to be statistically significant.
Patients (46 men and 16 women) had a mean age of 53 years (range 30–85), with a mean period of 12.4 years (range 1–33) since HIV-1 infection diagnosis. In the whole population, the mean period of ART was 107.1 months (range 10–295), while the mean period of ART with ABC/3TC plus RAL was 26.5 months (range 2–70). Data separated for the treatment-naïve and treatment-experienced groups are presented in Table 1. Five patients (8.1%) were naïve to ART, while the other 57 patients (91.9%) were ART-experienced, virologically suppressed at the start of the new regimen. Prior to switch, ART consisted of a PI-based regimen in 33 patients (57.9% of treatment-experienced patients), NNRTI-based regimen in 5 patients (8.8%), INSTI-based regimen in 15 patients (26.3%), NRTI-based regimen in 2 patients (3.5%). In one patient (1.8%), the regimen was a combination of NNRTI and PI, while in another patient (1.8%) it consisted of a combination of INSTI and NNRTI. The reasons for switching to ABC/3TC plus RAL were toxicity to the previous regimen (50.9%), dyslipidaemia (40.4%), treatment simplification (3.5%) and drug interactions (1.8%). For the patients experiencing toxicity, renal toxicity was the most frequent (22.8% of total patients), followed by gastroenteric toxicity (17.5%) and hepatic toxicity (5.3%); two patients (3.5%) experienced bone toxicity, while one patient (1.8%) presented psychiatric disorders. Dyslipidaemia, gastroenteric toxicity and drug interactions were mainly related to the switching from PI and NNRTI to RAL, while renal toxicity was the main cause for the switching from a tenofovir/emtricitabine (TDF/FTC) backbone to ABC/3TC.
Baseline characteristics of the study population.
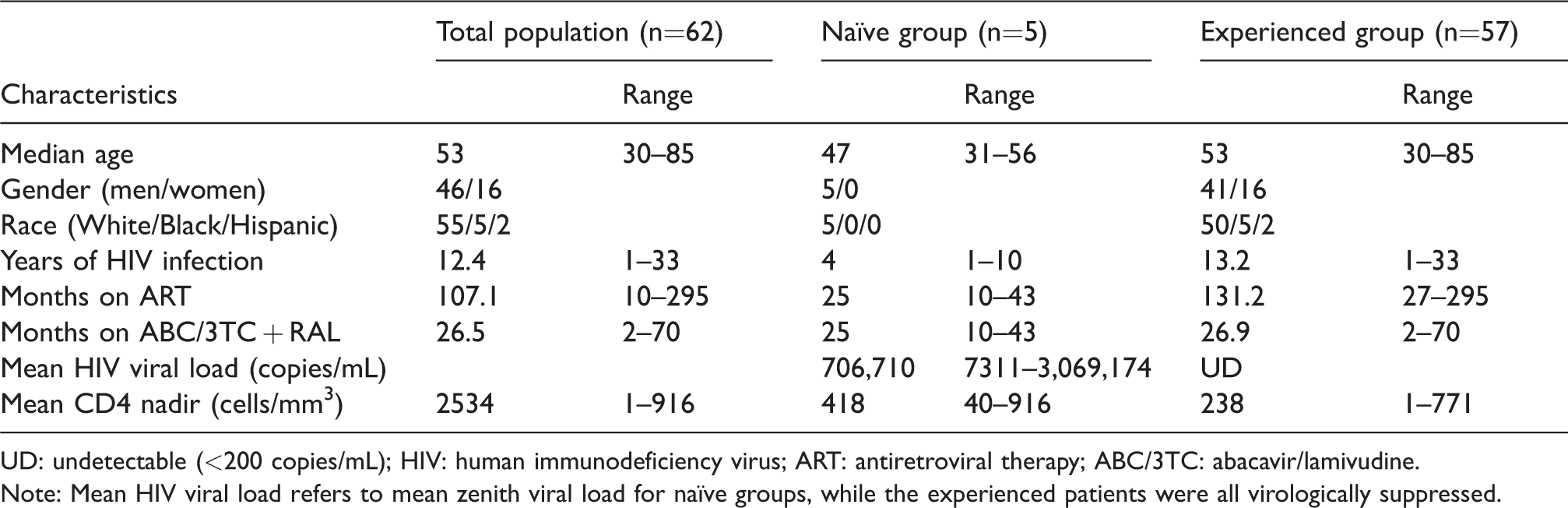
UD: undetectable (<200 copies/mL); HIV: human immunodeficiency virus; ART: antiretroviral therapy; ABC/3TC: abacavir/lamivudine.
Note: Mean HIV viral load refers to mean zenith viral load for naïve groups, while the experienced patients were all virologically suppressed.
The mean zenith viral load among the naïve group was 706,710 copies/mL (range 7311–3,069,174). Among all patients, the mean nadir CD4+ cell count was 253 cells/mm3 (range 1–916): in particular it was 418 cells/mm3 in the treatment-naïve group (range 40–916) and 239 cells/mm3 in the treatment-experienced group (range 1–771). Twenty-nine patients (46.8%) had a nadir CD4+ <200 cells/mm3 (one of them was in the treatment-naïve group, the remaining were in the treatment-experienced group). Characteristics of patients are shown in Table 1.
Results
The results of our study are shown in Table 2.
Metabolic changes in the study population, in the treatment-experienced group and in the switched from PI group.
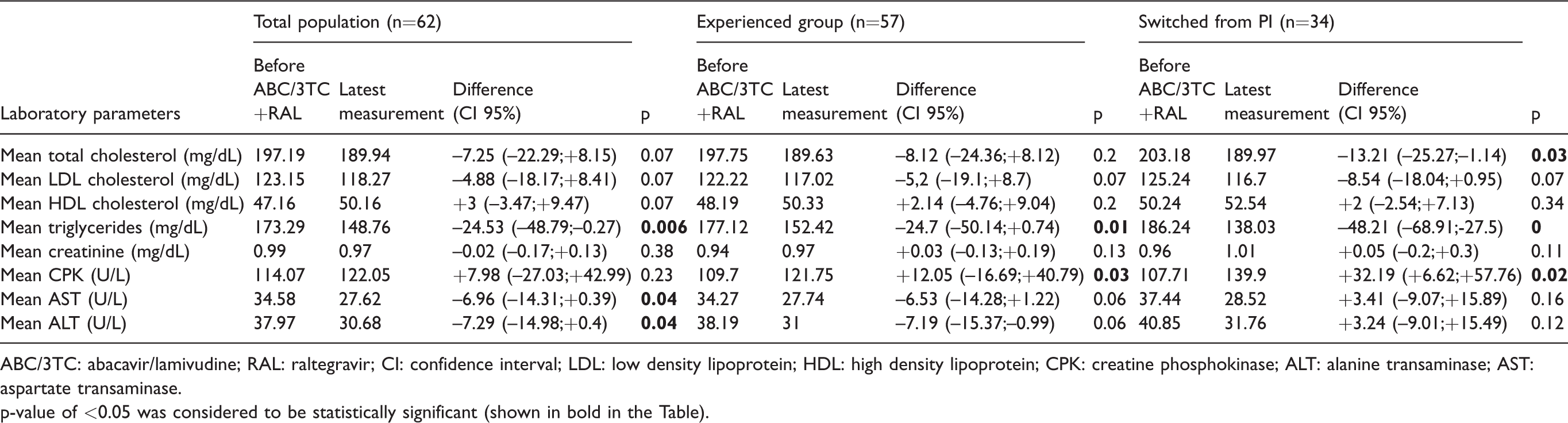
ABC/3TC: abacavir/lamivudine; RAL: raltegravir; CI: confidence interval; LDL: low density lipoprotein; HDL: high density lipoprotein; CPK: creatine phosphokinase; ALT: alanine transaminase; AST: aspartate transaminase.
p-value of <0.05 was considered to be statistically significant (shown in bold in the Table).
Sixty of the 62 patients were virologically suppressed (HIV-RNA <200 copies/mL) at the latest measurement (96.8%). The two patients who presented virological failure at the time of analysis (respectively, 666 copies/mL and 1370 copies/mL of HIV-RNA) were both treatment-experienced patients; virological failures were due to lack of adherence. Genotypic resistance tests were not performed. The five patients who started ABC/3TC plus RAL as their first ART were virologically suppressed at the latest measurement. Among these patients, three had baseline HIV-RNA >100,000 copies/mL, while two had baseline HIV-RNA <100,000 copies/mL.
The mean increase of CD4+ cell count from baseline to the latest measurement was 461 cells/mm3 (p < 0.01) among all the patients of the study. In the treatment-naïve group, the mean increase of CD4+ was 318 cells/mm3 (not statistically significant), while in the treatment-experienced group the mean increase was 474 cells/mm3 (p < 0.01).
Regarding lipid metabolism, we observed a mild non-significant decrease of total cholesterol and LDL cholesterol in the whole population of the study. On the other hand, among all the patients of the study, we observed a significant decrease in triglycerides (p=0.006) and transaminases (p=0.04 for both AST and ALT values). Creatinine and creatine phosphokinase did not differ before and after the start of ABC/3TC plus RAL.
Data were similar in the treatment-experienced group, with only a significant decrease of triglyceride values after the switch to ABC/3TC plus RAL (p=0.01). On the other hand, differently from the whole population of the study, we observed a significant increase in creatine phosphokinase values in the treatment-experienced group (p=0.03), but within the range of normal values.
We observed a significant improvement in the lipid profile of treatment-experienced patients who switched from a PI-containing regimen to the new regimen: particularly, we observed a significant decrease of total cholesterol (p=0.03) and triglycerides (p < 0.01). We also observed a significant increase in creatine phosphokinase in this specific population (p=0.02), but within the range of normal values. Non-significant differences were observed in patients who switched from other regimens to ABC/3TC plus RAL.
Considering the small number of patients, in the five treatment-naïve patients we did not find any significant difference in lipid profile, renal and liver function and creatine phosphokinase between pre-treatment values and values at the latest measurement.
Discussion
In this retrospective observational study, we evaluated the safety and efficacy of ABC/3TC plus RAL in treatment-experienced and treatment-naïve patients.
In the treatment-experienced group, 96.5% of the patients (55/57) were virologically suppressed at the latest measurement. The two virological failures were due to the lack of adherence; genotypic resistance tests were not performed; they became subsequently aviraemic after switching to, respectively, ABC/3TC/DTG single tablet regimen and ABC/3TC plus darunavir/cobicistat (DRV/c). This may be due to improved adherence to the new regimen, as reported by both patients (both new regimens have once-daily dosing).
A limited number of other small-scale studies have investigated the efficacy of ABC/3TC plus RAL in treatment-experienced patients. Suzuki et al. observed viral suppression at 48 weeks in 91.6% of the treatment-experienced subjects, who switched from a PI-based or NNRTI-based regimen to ABC/3TC plus RAL 6 ; Kang et al., in their study, assessed the efficacy of ABC/3TC plus RAL in treatment-experienced patients, with 93% achieving viral suppression after the switch from PI-based or NNRTI-based regimens to RAL plus ABC/3TC or ZDV/3TC. 7 Similarly, the ORALSWIRAL study showed the efficacy of ABC/3TC plus RAL in treatment-experienced patients with virological suppression, with 95% achieving viral suppression at 96 weeks. 8 Finally, in the RASTA study only two of the 40 subjects included (5%) discontinued treatment for virological failure. 9 The KIRAL study, a recent multi-centre, non-controlled, retrospective study, assessed the efficacy of ABC/3TC plus RAL in 380 virologically-suppressed patients, showing a high virological suppression rate at 48 weeks (97.6% of subjects with HIV-RNA <50 copies/mL). 10
With regard to the metabolic profile, as already mentioned, we observed a significant difference in triglycerides between mean values before the switch to ABC/3TC plus RAL and mean values at the latest measurement. We have therefore differentiated subjects according to the previous regimen: in the patients who switched from PI-based regimens, we observed a significant improvement of the lipid profile, particularly a decrease of total cholesterol and triglycerides. Similarly to our study, in other studies the switch to ABC/3TC plus RAL led to an improvement in lipid levels and liver function, particularly if the previous regimen contained a PI.6,7,10,11
In the treatment-naïve group, all five patients achieved viral suppression at the latest measurement, suggesting the efficacy of ABC/3TC plus RAL among treatment-naïve patients. Three patients had pre-treatment viral loads > 100,000 copies/mL, and all of them achieved viral suppression. In the DHHS guidelines announced this year 1 and in the recent European 2 and Italian 3 guidelines, the regimen ABC/3TC plus RAL is recommended as an alternative regimen, only if pre-treatment viral load is <100,000 copies/mL. This is because there is only one randomized clinical trial which has investigated the safety of ABC/3TC plus RAL in treatment-naïve patients (SPRING-2 study). In this study, DTG was compared with RAL in association with TDF/FTC or ABC/3TC: in the ABC/3TC group, virological non-response rates in people with a pretreatment viral load above 100,000 copies were, at 96 weeks, significantly higher in RAL than in DTG. 12
However, the SHIELD trial demonstrated durable virological suppression after 96 weeks of treatment with ABC/3TC plus RAL in treatment-naïve patients, even in patients with pre-treatment viral load >100,000 copies/mL, despite it being a small sample size. 13 Similarly, Suzuki et al. and Kang et al., already mentioned with regard to treatment-experienced subjects, showed in their abovementioned studies optimal therapeutic effect of ABC/3TC plus RAL also in treatment-naïve patients, even with pre-treatment viral loads >100,000 copies/mL.6,7
As regards the safety of ABC/3TC + RAL in treatment-naïve patients, we did not observe any significant alteration in lipid profile, liver and renal function, in accordance with Suzuki et al. 6
Conclusions
Some limitations should be recognized when interpreting the results of our study. The structure of the study (observational, retrospective, absence of a control group) and the small number of the sample size, especially for the treatment-naïve patients, are important limitations to allow definitive conclusions. Furthermore, the point prevalence of suppressed viral load is not a good marker of viral suppression. In addition, metabolic values were not stratified by age, co-medications or duration of ART. On the other hand, it can provide clinicians who want to start ART with useful information on the safety and efficacy of this regimen. Indeed, the limited proportion of virological failures observed and the metabolic safety, particularly regarding lipid levels, suggest a higher tolerability of this RAL-based regimen compared to PI-based or NNRTI-based regimens. Furthermore, the switch to this ART, with the recent availability of a generic co-formulation of ABC/3TC, could have a significant economic impact on hospital drug expenditure. Given the low number of studies which have investigated the safety and efficacy of this regimen, either in treatment-naïve or -experienced patients, prospective studies on larger populations are required.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.