
Abstract
In Latin America, men who have sex with men (MSM) remain disproportionately impacted by HIV. Pre-exposure prophylaxis (PrEP) is an effective HIV prevention tool and has been FDA approved in the United States since 2012, but no Latin American state, with the recent exception of Brazil, has implemented PrEP guidelines. We carried out a multinational online survey of MSM in Latin America (n = 22698) in 2012 to assess whether MSM at highest risk of HIV acquisition (i.e., those engaging in condomless anal sex [CAS; n = 2606] and transactional sex [n = 1488]) had higher levels of awareness of PrEP, PrEP use and interest in participating in a PrEP trial. After adjusting for demographic and psychosocial characteristics including depressive symptoms, hazardous alcohol use, childhood sexual abuse, and sexual compulsivity, transactional sex and CAS were associated with increased PrEP awareness (aOR = 1.29, 95% CI: 1.05–1.59, p < .001 and aOR = 1.22, 95% CI: 1.11–1.34, p < .001, respectively) and PrEP trial interest (aOR = 1.45, 95% CI: 1.25–1.71, p < .001 and aOR = 1.74, 95% CI: 1.57–1.95, p < .001, respectively). Findings demonstrate substantial awareness of and interest in PrEP among MSM with behavioral risk factors for HIV in Latin America, suggesting that this region is primed for PrEP implementation, which has been slow.
Introduction
Men who have sex with men (MSM) in Latin America, including Mexico, Central America, South America, and the Spanish-speaking Caribbean, are disproportionately affected by HIV.1–5 Moreover, men who engage in transactional sex with other men (i.e. exchange sex for money or drugs) are at further increased risk of HIV due to reduced ability to negotiate condom use, stigma, and increased burden of psychosocial risk factors.6–8 While countries in this region have been largely successful in expanding antiretroviral therapy (ART) coverage in the past decade to individuals living with HIV, 2 they have yet to successfully curb the HIV epidemic. As such, Latin American countries might best supplement their HIV prevention efforts with newly available tools, including promotion of tenofovir/emtricitabine (TDF/FTC) as pre-exposure prophylaxis (PrEP). 9
Mexico, Brazil, and Colombia, the three largest countries by population in the region, have concentrated HIV epidemics among MSM (prevalence of 16.9%, 17.5–18.4%, 15.0–24.1%, respectively), all higher than the pooled regional prevalence for Latin America (14.9%).10–12 While all three countries have universal healthcare systems which provide ART for HIV, as of June 2018, Brazil is the only Latin American country to have implemented comprehensive distribution of PrEP for HIV prevention through state-sanctioned systems. Mexico has active PrEP demonstration projects, while Colombia has implemented a unified public health plan in March of 2017, under which PrEP is not explicitly prohibited. However, state-sanctioned guidelines for PrEP do not yet exist in either country, and implementation of PrEP would follow precedent set by Brazil, and be in line with the 2015 Rio Call to Action. 13 Brazil, Mexico, and Colombia, as the three largest countries in the region, could set the stage for wider adoption throughout the region.
The continuing HIV epidemic among MSM in Latin America implores targeted HIV prevention approaches that are acceptable to MSM. 9 Yet, there is limited literature to date which explores awareness and acceptability of PrEP in Latin America among MSM. 14 To this end, we assessed PrEP awareness, PrEP use and interest in PrEP trial participation, and differences by sexual risk behaviors, among a large, multinational sample of MSM in Latin America—namely, Mexico and Spanish- or Portuguese-speaking Central America, South America, and the Caribbean. The goal of this paper is to elucidate associations between sexual risk behaviors and interest in PrEP among MSM in the region.
Methods
Participants and procedures
The data for these analyses were collected through an anonymous online survey of Spanish- and Portuguese-speaking MSM in Latin America and the Caribbean (over 30 days from October to November of 2012), age 18 or older, actively using a popular social/sexual networking site. Procedures have been described in detail elsewhere. 1 In brief, a survey was developed and subsequently translated into Spanish and Portuguese collaboratively by native speakers of each language who are experts in HIV prevention or sexual minority sexual health, and back-translated to English to verify accuracy. The surveys were then piloted with a small sample of the target population, and was distributed via email to approximately 643,000 network members who had logged on at least once in the previous 90 days and listed their country of residence as any of the following: Spain, Portugal, or any Spanish- or Portuguese-speaking country/territory in Latin America or the Caribbean. In all, 246,620 emails were opened, 56,584 individuals clicked the survey link and 36,063 initiated the survey. For these analyses, we limited our sample to respondents who reported: residence in a Spanish- or Portuguese-speaking country in Latin America (including the Caribbean), male gender at birth and current male gender identity, sex with a man in the past year, and being HIV uninfected or of unknown HIV status (n = 22,698). All study procedures were approved by the Institutional Review Board at The Fenway Institute at Fenway Health in Boston, MA.
Measures
Demographics: Respondents reported their age, sexual orientation, self-perceived income/class (high, middle, and low), type of living area (urban vs. rural), and country of residence.
Sexual behavior: Respondents were asked if they had received payment for sex in the past year and if they had any condomless anal sex with an HIV-infected partner or partner of unknown status (serodiscordant/serostatus unknown CAS) in the past three months.
Psychosocial factors: Given evidence that psychosocial risk factors can result in reduced engagement in care and increased HIV incidence3,5 (and therefore may impact PrEP knowledge or interest), we assessed the following as covariates: Depressive symptoms were assessed by the validated ten-item Center for Epidemiologic Studies Depression Scale (CES-D 10), with a score of 10 or greater considered suggestive of clinical depression. 15 Alcohol dependence was assessed using the validated four-item CAGE scale,16,17 with a score of 2 or greater considered suggestive of dependence. Childhood sexual abuse was assessed by a series of questions about any sexual experience prior to age 13 with someone 5 or more years older and/or sexual experience between ages 13 and 17 with someone 10 or more years older. Lastly, a score of 24 or greater on the sexual compulsivity scale was considered suggestive of sexual compulsivity.18,19 These measures have been described in further detail elsewhere. 5
PrEP measures: Respondents were briefly informed (in one paragraph of text) about on-going testing of PrEP for HIV prevention, including that PrEP is taken daily and is intended to prevent HIV among HIV-uninfected individuals. Awareness of PrEP was operationalized as the following questions: (1) “Have you ever heard of HIV-negative people taking HIV medicines before sex because they thought it would prevent HIV infection?” and (2) “Have you ever taken “anti-HIV” medicines before sex because you thought it would reduce your chances of becoming infected with HIV?” Responses were dichotomous (yes or no). Interest in PrEP was operationalized as the following question: “How interested are you in participating in a PrEP trial?” Responses were dichotomized (any interest vs. no interest/unsure) as the magnitude of their interest was not the primary outcome for this analysis.
Statistical analysis
Frequencies and percentages were calculated for personal characteristics and psychosocial factors for the overall sample and by sexual risk behavior for each outcome. We used unadjusted and multivariable logistic generalized estimating equations (GEE) to examine association of (1) recently receiving payment for sex (defined here as “transactional sex”) and (2) recent serodiscordant/serostatus unknown CAS with PrEP knowledge, prior PrEP use and PrEP trial interest. GEE was used to account for clustering by country. Multivariable models were adjusted for a priori selected demographics and psychosocial factors. Models examining the association of transactional sex with PrEP-related measures also adjusted for CAS to estimate the association independent of CAS. All models were examined for all countries combined and separately for Mexico, Brazil, and Colombia to assess potential country-level differences for the countries with the largest populations in the region and largest representation in our sample (Ns = 7657, 3072, 3028, respectively). We used listwise deletion for our analysis.
Results
The overall respondent profile has been described in further detail previously. 1 In this sample, the average age of respondents was 30.0 years (n = 22,698; SD = 8.8). Most participants identified themselves as middle class (n = 16,359; 74.8%), had completed a university or post-graduate degree (n = 17,852; 79.0%), lived in urban areas (n = 21,707; 95.6%), and identified as homosexual/gay (n = 17,163; 75.8%). Nearly three-quarters (72.7%) of participants reported depressive symptoms, over one half (59.0%) reported experiencing childhood sexual abuse, 15.6% reported alcohol dependence and 14.8% reported sexual compulsivity.
Overall, 10.4% were aware of PrEP, 0.8% had ever used PrEP, and 62% expressed interest in participating in a PrEP study. Of 7.2% (n = 1488) of the respondents who reported receiving payment for sex in the past 12 months (Table 1), 13.4% (n = 199) had heard of PrEP previously compared to 9.7% (n = 1851) of those who had not received payment for sex (n = 19140). Similarly, 1.9% (n = 28) of those who reported receiving payment for sex reported prior use of PrEP compared to 0.7% (n = 128) of those who did not; additionally, 69.1% (n = 1028) were interested in participating in a PrEP trial compared to 58.8% (n = 11,252) of those who did not receive payment for sex.
Awareness, prior use, and interest in participating in PrEP trials by behavioral HIV risk.

PrEP: pre-exposure prophylaxis; MSM: men who have sex with men; UAI: unprotected anal intercourse.
Of the 14.6% (n = 2606) respondents who reported serodiscordant/serostatus unknown CAS in the past three months (Table 1), 11.0% (n = 287) had heard of PrEP previously compared to 8.9% (n = 1360) of those who had not (n = 15,260). Similarly, 1.1% (n = 29) of those who reported serodiscordant/serostatus unknown CAS reported prior use of PrEP compared to 0.6% (n = 88) of those who did not; additionally, 67.6% (n = 1763) were interested in participating in a PrEP trial, compared to 54.0% (n = 8240) of those who did not report serodiscordant/serostatus unknown CAS.
Overall
Unadjusted and adjusted models are displayed in Table 2. In adjusted models for the overall sample, MSM that received payment for sex had higher odds of having heard of PrEP (adjusted odds ratio [aOR]=1.29, 95% CI: 1.05–1.59), of having ever taken PrEP (aOR = 1.98, 95% CI: 1.05–3.73), and of expressing interest in participating in a PrEP trial (aOR = 1.45, 95% CI: 1.25–1.71) compared to MSM who did not receive payment for sex, even after adjusting for CAS as a proxy for sexual risk. Similarly, MSM who engaged in recent serodiscordant/serostatus unknown CAS had higher odds of having heard of PrEP (aOR = 1.22, 95% CI: 1.11–1.34), of having ever taken PrEP (aOR = 1.76, 95% CI: 1.16–2.65), and of expressing interest in participating in a PrEP trial (aOR = 1.74, 95% CI: 1.57–1.95).
Associations of sexual risk and PrEP awareness, use and interest.
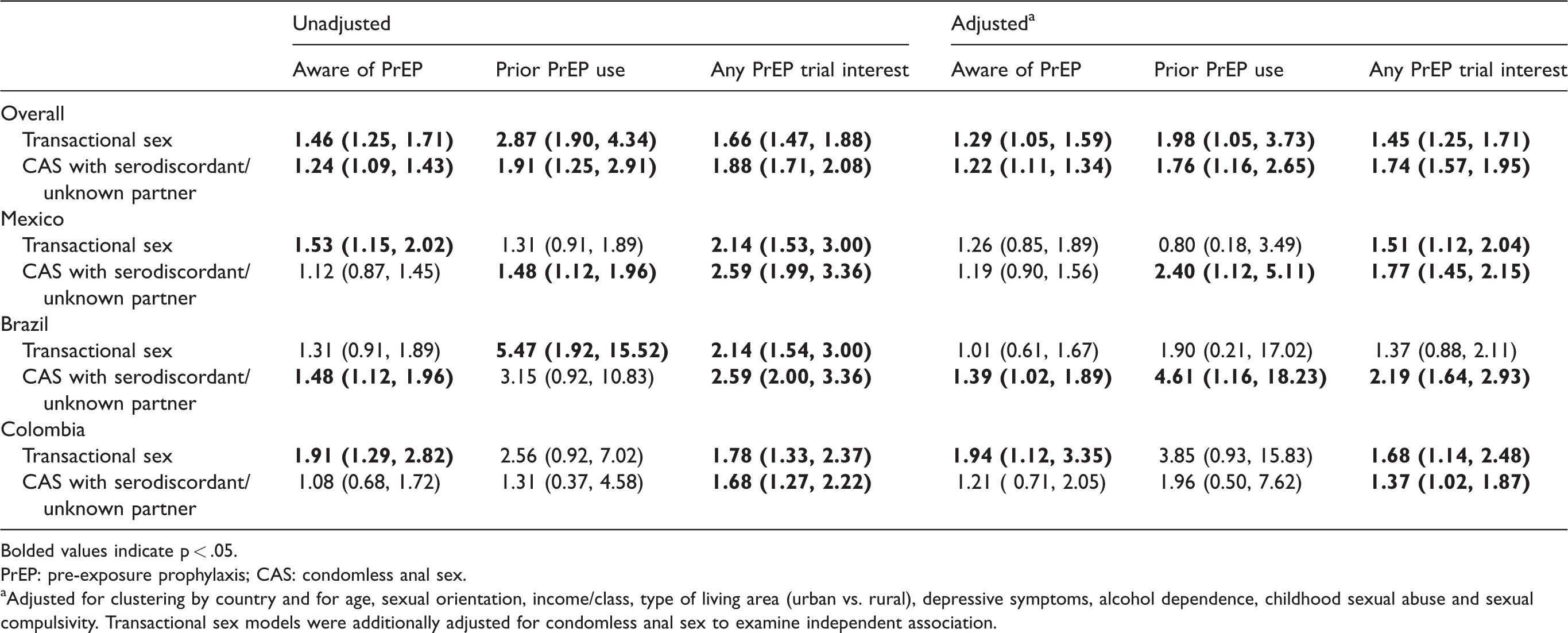
Bolded values indicate p < .05.
PrEP: pre-exposure prophylaxis; CAS: condomless anal sex.
aAdjusted for clustering by country and for age, sexual orientation, income/class, type of living area (urban vs. rural), depressive symptoms, alcohol dependence, childhood sexual abuse and sexual compulsivity. Transactional sex models were additionally adjusted for condomless anal sex to examine independent association.
Country-specific
Country-stratified analyses suggest differences with respect to at least one association (Table 2). Mexico: There was not a significant increase in odds of having heard of PrEP for MSM who received payment for sex or CAS with serodiscordant/unknown partner within Mexico. Regarding prior use of PrEP, MSM who engaged in CAS with serodiscordant/unknown partner had higher odds of prior use (aOR = 2.40, 95% CI: 1.12–5.11), but this did not hold true for MSM reporting receiving payment for sex. Both of the defined risk groups had increased odds of PrEP trial interest (transactional sex: aOR = 1.51, 95% CI: 1.12–2.04; CAS: aOR = 1.77, 95% CI: 1.45–2.15). Brazil: Receiving payment for sex was not associated with increased odds of awareness, prior use, or interest in PrEP trials. CAS with serodiscordant/unknown partner was associated with increased odds of awareness (aOR = 1.39, 95% CI: 1.02–1.89), prior use (aOR = 4.61, 95% CI: 1.16–18.23) and interest in PrEP trials (aOR = 2.19, 95% CI: 1.64–2.93). Colombia: Only receiving payment for sex was associated with PrEP awareness (aOR = 1.94, 95% CI: 1.12–3.35). Neither receiving payment for sex nor CAS with serodiscordant/unknown partner was associated with prior use of PrEP, but both were associated with interest in PrEP trial (transactional sex: aOR = 1.68, 95% CI: 1.14–2.48; CAS: aOR = 1.37, 95% CI: 1.02–1.87).
Discussion
PrEP is an effective HIV prevention tool,27,28 but no Latin American state, with the recent exception of Brazil, has implemented PrEP guidelines. The findings from our study document increased awareness, self-reported use, and interest in PrEP trials among MSM with higher behavioral risk factors in Latin America compared to MSM overall, and are supported by previous work done in the USA and internationally.20–23 A recent study in Brazil 24 found that higher risk sexual behaviors for HIV infection, as well as increased perceived risk for HIV infection, are associated with increased willingness to use PrEP. Similarly, findings from this study mirror those recently published regarding an online survey of MSM using popular geosocial networking smartphone apps across ten Brazilian cities. 25 Notably, Torres et al. found that willingness to use daily oral PrEP was associated with higher numbers of male sexual partners and receptive CAS. Furthermore, we note that the observed patterns of increased awareness, prior use and interest in PrEP remained even after adjusting for psychosocial risk, which has been shown to be associated with reduced engagement in HIV care and increased HIV incidence in similar populations in the US.3,5
This analysis provides further evidence that at-risk MSM in Latin America show increased interest in PrEP trials compared to MSM overall, and suggests that they may be willing to integrate PrEP into their HIV prevention efforts. To date, however, there has been limited progress in implementing PrEP policies in the region. Currently, seven countries in the region are planning or beginning to implement PrEP projects; however, only some of these will include MSM, and political, social, and economic barriers remain to large-scale implementation beyond demonstration projects in most of the region. 14 To date, Brazil is the only country in Latin America to have implemented comprehensive, national guidelines for PrEP as part of its HIV prevention efforts. 9 Overall, there has been limited research on awareness and interest in PrEP among high-risk MSM in Latin America. Despite this, communities throughout the region have been increasingly vocal about their support for PrEP, with numerous activist groups and civil society organizations positioning PrEP as an essential next step in HIV prevention efforts. 26 More work is needed to guide the implementation of biomedical HIV prevention guidelines throughout the region in a way that meets the needs of expectations of the communities that have mobilized around PrEP access.
This analysis highlights Mexico, Brazil, and Colombia as they are the three largest countries in Latin America by population, among the wealthiest in the region, and carry much of the regional HIV burden among MSM. 2 Comprehensive implementation, or expansion of PrEP distribution, to MSM in these countries would be in line with regionally determined targets and set a precedent for further distribution throughout the region.13,14 Current PrEP demonstration projects in Mexico City and Brazil (such as the ImPrEP project) for high risk MSM could provide further indication for wide distribution of PrEP to eligible patients in these country’s public healthcare systems.9,14 However, these three countries are not representative of the region as a whole, and certainly are home to unique cultural contexts which do not mirror those found in other countries throughout the region. Thus, though these three countries may serve as a good indicator of the future of PrEP in Latin America, additional work is needed to assess the acceptability of PrEP among MSM across sociodemographic groups within each Latin American country.
Our findings should be taken in the context of some limitations. First, the data were obtained in 2012, so these findings may not approximate current levels of awareness and interest in PrEP. In light of ongoing PrEP demonstration projects in Brazil and Mexico (HIV/AIDS, 2018), and the increasing visibility of PrEP globally since this survey was conducted in 2012, awareness and interest in PrEP may be even greater now among these groups, particularly in light of ongoing demonstration projects in a number of Latin American countries. Additionally, emtricitabine/tenofovir as PrEP for HIV was approved by the Food and Drug Administration (FDA) in the United States, including Puerto Rico, in July 2012, just months prior to this survey. However, the survey was conducted only three months after FDA approval, so we do not expect that awareness of PrEP had been influenced significantly by this among respondents from Puerto Rico in the sample (n = 228). However, even though prevalence of awareness, use and interest may be underestimated, the associations between sexual risk and the PrEP-related measures are not likely to change substantially.
Additionally, the sample of MSM in this study was reached through a social/sexual networking website, so they are likely not representative of MSM in Latin America overall. Our analytic sample largely identified as college educated and middle class or higher, which indicates that we may not have reached lower income or less-educated MSM that may face increased obstacles in access to care, and therefore, also have less awareness of or interest in PrEP. Self-reported use of PrEP for HIV prevention was very low (n = 156) and may include the use of other medications in a manner inconsistent with their intended use, including other antiretrovirals. Increased odds of use of PrEP among HIV-uninfected MSM in the overall sample, though, does suggest experience taking any medication with intent to prevent HIV infection, and warrants further research on the prevalence of informal antiretroviral use for HIV prevention among this population. Furthermore, while a number of the psychosocial scales were pilot-tested with members of the target population, they have not been validated in Spanish and Portuguese, and may not be relevant for MSM in Latin America. Lastly, interest in participating in PrEP trials is only a proxy for interest in using PrEP itself, and may not directly predict uptake of PrEP outside of studies.9,20,24,29,30
Conclusion
Despite these limitations, our findings document increased awareness, self-reported use, and interest in PrEP trial participation for HIV prevention for those with highest behavioral risk for HIV among a large, multinational sample of MSM in Latin America. In response to increasingly visible calls for PrEP implementation, 26 Latin American states will need to focus on uptake, education about risk for HIV infection, and proper use of PrEP as a supplementary tool for curbing the HIV epidemic that continues to disproportionately impact MSM. As demonstration projects continue to highlight14,31 that PrEP is an effective HIV prevention method for MSM in Latin America, it is imperative that regional governments endorse or develop implementation guidelines. Stigma around homosexuality and moralistic arguments against PrEP 14 will likely remain a significant barrier to PrEP implementation. As such, further efforts to implement PrEP regionally will necessarily require further understanding of willingness to use PrEP, and advocacy and activism from key stakeholders in Latin America, including at-risk MSM.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.