
Abstract
Late diagnosis of HIV remains a threat to personal and public health – both increasing the morbidity and mortality of the person and also increasing the chance of unknowingly transmitting HIV. Many HIV testing initiatives, including those of the British HIV Association (BHIVA), focus on levels of high prevalence (greater than 2:1000). However, late diagnosis can be an issue in areas of low prevalence – areas which can be less densely populated and in some cases classified as rural. In our rural catchment area, late diagnosis is an issue with 67% diagnosed late in 2015 (which is skewed by the single figure diagnoses). This lookback examined the number of missed opportunities for HIV diagnosis over a seven-year period and found that where diagnoses were made late in the context of a person having previously presented for care, unexplained weight loss, blood dyscrasias and lymphadenopathy were the most common presentations that could have triggered a HIV test.
Background
Public Health England has set the reduction of late diagnosis of HIV as one of its three key Public Health Outcome Framework Measures in relation to sexual health. 1 In 2008, the British HIV Association (BHIVA), British Association of Sexual Health and HIV (BASHH) and the British Infection Society (BIS) published guidelines of when clinicians should test for HIV, notably a list of conditions that should trigger testing (Indicator Conditions). 2 These conditions were split down by specialties such as gastroenterology, haematology, etc. and represented conditions where there was a higher likelihood of HIV. In Cumbria, there are high rates of late diagnosis of HIV, which leads to greater morbidity and mortality as well as increasing the risk of those with HIV unknowingly passing on HIV. We conducted a review to identify potential missed opportunities for HIV-testing in North Cumbria (2016 prevalence 0.53/1000).
Methodology
A retrospective review was performed of the case notes of patients with a first-positive HIV test at the local laboratory 2010–2017. Patients known to be infected with HIV before 2010 were excluded. We searched for secondary care episodes with a clinical indicator condition in the five years before diagnosis. Episodes of care where an indicator condition was present but no HIV test was performed were allocated as missed opportunities. Primary care records were not accessed – primary care contacts were inferred from secondary care contacts (i.e. review of hospital notes and letters).
Results
Fifty-two cases with male to female ratio of 5:1 were identified. Notes for 31 patients (59%) were reviewed. Of cases that were not reviewed, 11 (21%) declined sharing their HIV status across healthcare teams, and in 4 cases (8%), consent to disclose was not clear. Notes were not available for two patients, and four patients (8%) could not be identified.
Clinical indicator versus screening
Of 31 patients, 18 (58%) presented with an indicator condition in accordance with BHIVA/BASHH/BIS’s 2008 recommendations when diagnosed, compared with 13 patients (42%) who had the test as part of screening. Of the 18 patients, 2 were tested at their first presentation with an indicator condition.
Healthcare contact prior to diagnosis
Fifteen patients (48%) had no previous secondary health care contact excluding the occasion at which they had been diagnosed. Sixteen patients (52%) attended either their primary or secondary health care provider with a clinical indicator condition and were not tested at initial presentation. Of those 16 patients, age range was 24–79 years, mean = 55.8 years, median = 56.5 years; 12 (75%) were male and 4 (25%) were female.
Of those who attended either their GP practice or hospital with a clinical indicator condition where an HIV test should have been offered according to the guidance, eight patients (50%) had one contact before the episode leading to diagnosis, five patients (31%) had two contacts, two patients (13%) had three contacts and one patient had more than three contacts before an HIV test was offered.
Overlooked clinical indicator conditions
Unexplained weight loss was the clinical indicator in 13 occasions, followed by unexplained lymphadenopathy and blood dyscrasia in six occasions for each. (Figure 1 illustrates the clinical indicators that were overlooked.)
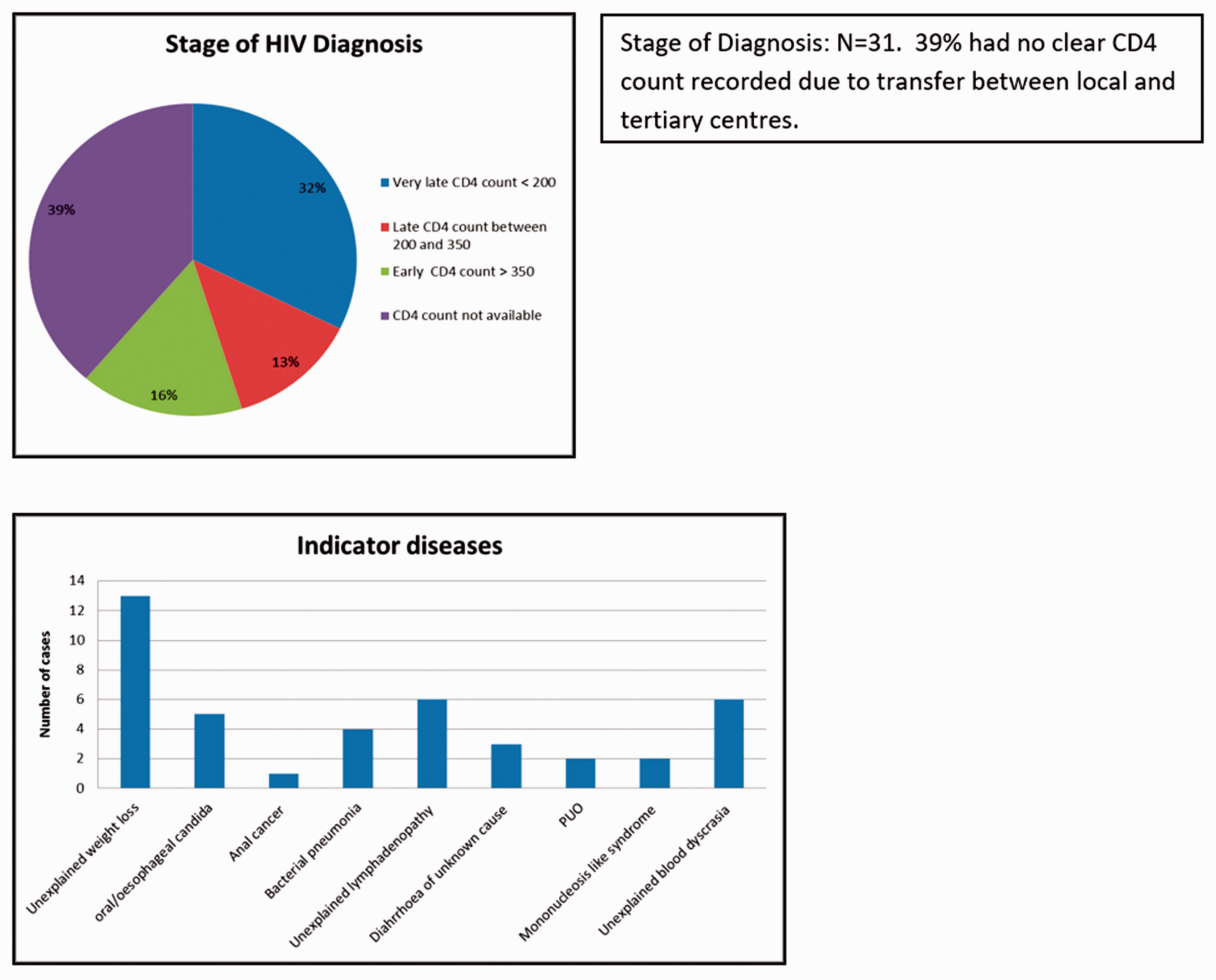
Clinical indicators that were overlooked. PUO: pyrexia of unknown origin.
Conclusions
The incidence of HIV infection in our study was 1.25/100,000 for 2017. This is similar to the nationally reported figure for 2016 (1.4/100,000). 3 One-third of the patients (32%) had a very late diagnosis, and more than a half of the cases (52%) attended either primary or secondary healthcare with a HIV clinical indicator condition, when an HIV test should have been offered. National surveillance data show that approximately one-eighth of all HIV infections in adults in the UK remain undiagnosed and that approximately 25% of newly diagnosed individuals have a CD4 cell count less than 200. For rural settings, this lookback suggests that ongoing support for all clinicians to consider HIV before labelling a condition unexplained is paramount – the top three indicator conditions being missed all being prefaced with ‘unexplained’.
Late diagnosis is the most important factor associated with HIV-related morbidity and mortality in the UK. 4 Testing for HIV infection is often not performed due to misconceptions held by healthcare workers when it is clinically indicated, as well as not having clinical suspicion that there is another process underlying the reason for presentation. We conclude that further education is needed of clinicians in a range of settings to enable confident testing of HIV when it falls within the differential diagnosis, and to know when to suspect HIV is within the differential diagnosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.