
Abstract
The genital colonization of certain Mycoplasma and Ureaplasma spp. has been associated with an increased the risk of acquisition and persistence of human papillomavirus. However, its association with high-risk human papillomavirus genotypes is not entirely clear, and the prevalence of such coinfections in cervical precancerous lesions has been poorly explored. Therefore, the aim of this study was to investigate the association of high-risk human papillomavirus with Mycoplasma and Ureaplasma spp. in 258 women recruited during their routine gynecological inspection at an outpatient clinic in Tabasco, Mexico. Among the Mycoplasma and Ureaplasma spp. evaluated in the present study, the highest peak of prevalence was attributed to Ureaplasma parvum (32.9%), followed by Mycoplasma hominis (14%), Ureaplasma urealyticum (6.6%), and Mycoplasma genitalium (0.8%). The overall prevalence rates of papillomavirus DNA and high-risk human papillomavirus were 25.6% and 17.1%, respectively. The overall association showed that M. hominis and U. urealyticum correlated significantly with high-risk human papillomavirus infection. According to the cytological results, the distribution of coinfection with high-risk human papillomavirus and U. urealyticum did not show significant differences with respect to severity of cervical lesions. Conversely, the association of high-risk human papillomavirus with M. hominis was more frequent in women with high-grade squamous intraepithelial lesions (P = 0.037).
Introduction
The colonization of the genitourinary tract with Mycoplasma and Ureaplasma spp. (Mycoplasma/Ureaplasma spp.) is commonly associated with the development of adverse clinical outcomes, such as nongonococcal urethritis, fallopian tube obstruction, and preterm birth. 1 The likelihood of presenting such complications is considered to depend greatly on the maintenance of an inflammatory environment, which may be enhanced by the presence of pathogenic microorganisms. 2 In the case of the cervix, previous studies have documented that sustained inflammation may modify the natural history of human papillomavirus (HPV) infection, thus increasing the risk of developing cervical cancer. 3 Therefore, it was proposed that Mycoplasma/Ureaplasma spp. play an important role in cervical carcinogenesis mediated by HPV. However, epidemiological data concerning the individual relationship of HPV with Mycoplasma and Ureaplasma spp. (Mycoplasma/Ureaplasma spp.) are not entirely clear.
The genital association between HPV and Mycoplasma/Ureaplasma spp. has been studied regarding several aspects of viral infection. Most of the studies have proposed that positivity for Mycoplasma/Ureaplasma spp. increases the risk of acquiring HPV infection, with Mycoplasma genitalium and Ureaplasma urealyticum being the most frequent species associated with viral infection, particularly with high-risk genotypes.4–6 In addition, some studies have evaluated the contribution of such an association on the risk of developing premalignant cervical lesions.7,8 However, to date, the epidemiological data are inconclusive, and the significance of such an association likely depends greatly on the intrinsic characteristics of the study, such as the number of high-risk HPV (HR-HPV) genotypes included in the study and the method employed for Mycoplasma/Ureaplasma spp. detection. Although it is widely known that persistent HR-HPV infection is the main risk factor for malignant progression to cervical cancer, few studies have found a significant correlation between the persistence of HPV and the concomitant prevalence of Mycoplasma/Ureaplasma spp.9,10
The association of HPV with Mycoplasma/Ureaplasma spp. has been mainly directed to M. genitalium and U. urealyticum due to the well-documented pathogenic behavior of these microorganisms.11,12 However, the contributions of other Mycoplasma/Ureaplasma spp. considered inhabitants of the genital tract, such as Mycoplasma hominis and Ureaplasma parvum, have been less studied. Therefore, the aim of this cross-sectional study was to assess the association of HPV with Mycoplasma and Ureaplasma spp. in cervical samples from apparently healthy women at an outpatient clinic in Tabasco, Mexico.
Materials and methods
Study population and sample collection
A cross-sectional study with a convenience sample of 258 women was conducted at a gynecology outpatient clinic in Tabasco, a southeastern city of Mexico. All individuals included in the study were women who underwent routine gynecological inspection from January to November 2017. All women were invited to participate in the study by explaining the purpose and procedures included in the protocol. Those who showed interest for inclusion in the study provided written informed consent before sampling. Two cervical samples were collected during gynecologic evaluation; the first sample was obtained using a cytobrush, which was used for a conventional Pap smear. The results from the cervical cytopathology were classified according to the Bethesda system 4 as described below: normal = negative for intraepithelial lesion or malignancy (NILM); inflammatory response (IR) = negative for intraepithelial lesion or malignancy with some degree of IR; atypical squamous cells of undetermined significance (ASC-US); low-grade squamous intraepithelial lesion (LSIL); high-grade squamous intraepithelial lesion (HSIL), and atypical squamous cells-cannot exclude HSIL (ASC-H). The second cervical sample was obtained with a medium-free culture swab (Becton, Dickinson, NJ, USA), which was stored at 4°C (2 h at maximum) during the patients’ sampling until genomic DNA extraction was performed at the laboratory. Cervical sampling for molecular evaluation was performed in only those individuals who voluntarily participated in the study. Women were not included in the study if they reported being pregnant, having undergone oral or vaginal treatment for urogenital infection in the previous six months, or having undergone a subtotal or total hysterectomy.
This study was designed according to the international standards for responsible research publication and was approved by the Institutional Review Board of the Juarez Autonomous University of Tabasco (Universidad Juarez Autonoma de Tabasco) (Protocol No. UJAT-20160006).
Processing of the biological samples
Cervical cells collected by swabs were detached by vortexing samples in a phosphate-buffered solution. DNA extraction was performed according to the manufacturer’s instructions included in the Purelink Genomic DNA mini kit (Thermo Fisher Scientific, MA, USA). DNA integrity was evaluated by β-globin amplification through qPCR. 5 Samples positive for β-globin were employed for molecular detection of HPV DNA and Mycoplasma/Ureaplasma spp.
Molecular differentiation of Mycoplasma/Ureaplasma spp
Detection of Mycoplasma/Ureaplasma spp. (M. genitalium, M. hominis, U. parvum, and U. urealyticum) was carried out by multiplex qPCR employing specific probes that were previously evaluated.6,7 In both multiplex PCR assays, the fluorophore and quencher combinations were 5′-FAM Carboxyfluorescein or Tetrachlorofluorescein (TET), combined with a 3′-Black Hole Quencher (BHQ)-1 or BHQ-plus, respectively (Integrated DNA Technologies, CA, USA). PCR was performed with a final 10-μL reaction volume containing 100 ng of the extracted DNA, 600 nM of each primer, and 500 nM of the probes. All reactions were performed in triplicate, and a positive sample (DNA from microorganisms isolated by culture) and a nontemplate control were included in each assay. Samples with a mean Cq value less than 30 were considered positive.
Evaluation of HPV DNA and genotyping
The overall prevalence of HPV DNA was assessed using the degenerate primers ELSI-f and ELSI-r by final-point PCR according to previously reported conditions. 17 The PCR products were visualized using electrophoresis with agarose gels stained with SYBR Safe (Thermo Fisher Scientific, MA, USA) and were visualized with the image documentation system ImageQuant LAS500 (General Electric, MA, USA). All samples positive with the ELSI primers were subject to further genotyping by qPCR.
HPV genotyping was conducted in separate reactions with type-specific primers that were previously reported.14,18 We analyzed the prevalence of the fifteen most common high-risk genotypes (HR-HPV: 16, 18, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, and 73) and two low-risk genotypes (LR-HPV: 6 and 11). PCRs were performed in a 10-μL reaction volume containing 100 ng of the extracted DNA and 350 nM each primer. Reactions were performed using the CFX96 real-time detection system (BIO-RAD, CA, USA). Reactions were performed in triplicate, and a positive sample (plasmid containing cloned target sequences) and a nontemplate control were included in each assay. Samples with a mean Cq value less than 30 were considered positive.
Statistical analysis
Statistical analysis was performed with the Statistical Package for the Social Sciences (SPSS, version 22; IBM, NK, USA). With the aim of analyzing the association between HPV and Mycoplasma/Ureaplasma spp., samples positive for HPV DNA were categorized and classified according to the number and oncogenic potential of the genotypes analyzed. The Fisher exact test was used to evaluate the statistical significance between groups. Data with a P value < 0.05 were considered statistically significant.
Results
The study population was composed of 258 healthy women aged 16–66 years (mean age 35, standard deviation 9.8). All women included in the study underwent routine gynecological examinations at an outpatient clinic and reported not being vaccinated against HPV. The β-globin amplification showed that all samples were suitable for molecular assessment.
The percentage of women positive for Mycoplasma/Ureaplasma spp. was 43.8% (113/258); of these, 34.9% were positive for at least one microorganism, while 8.9% of the samples harbored multiple Mycoplasma/Ureaplasma spp. (Table 1). The most common Mycoplasma/Ureaplasma spp. was U. parvum (32.9%), followed by M. hominis (14%), U. urealyticum (6.6%), and M. genitalium (0.8%).
Prevalence of Mycoplasma/Ureaplasma spp. and human papillomavirus (HPV) infection in a cross-sectional study of 258 healthy women.
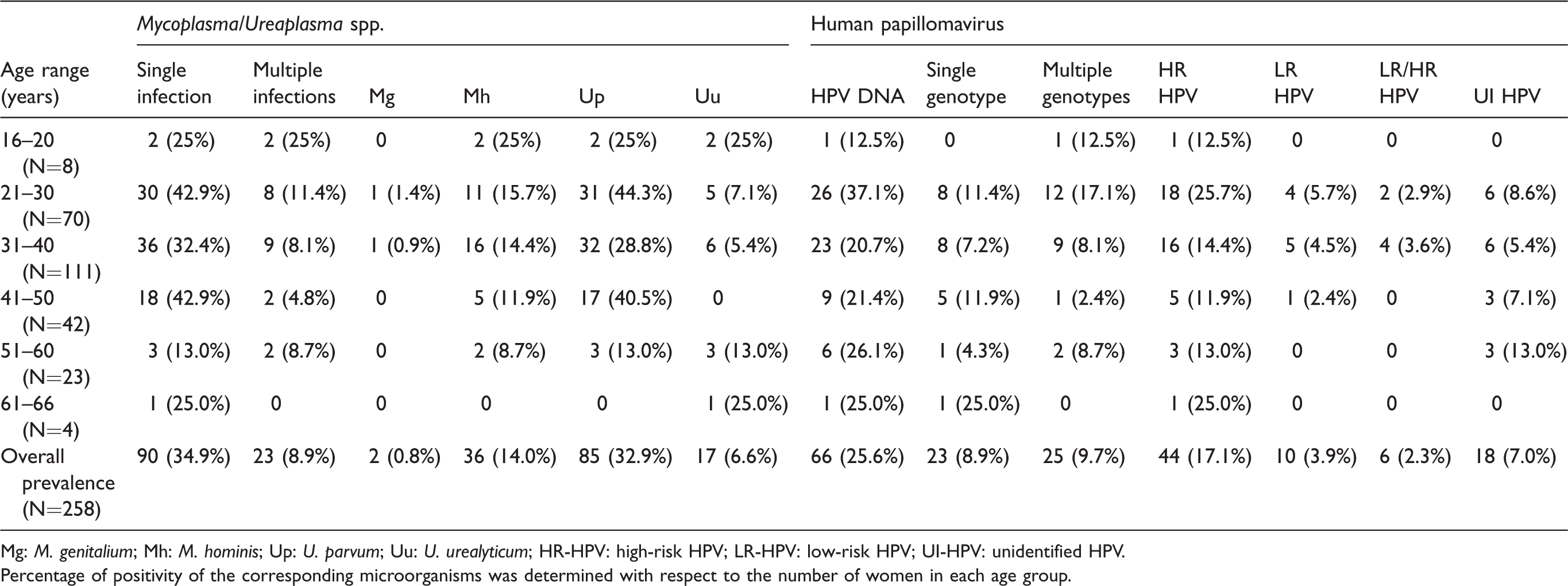
Mg: M. genitalium; Mh: M. hominis; Up: U. parvum; Uu: U. urealyticum; HR-HPV: high-risk HPV; LR-HPV: low-risk HPV; UI-HPV: unidentified HPV.
Percentage of positivity of the corresponding microorganisms was determined with respect to the number of women in each age group.
Regarding HPV infection, 25.6% (66/258) of the women were positive for HPV DNA. Of these, the percentage of women positive for low-risk and high-risk types analyzed was 15.1% (10/66) and 66.6% (44/66), respectively. However, the frequency of single (34.8%, 23/66) and multiple (37.8%, 25/66) HPV infections was similar in both groups. The remaining samples positive for HPV DNA (18, 27.2%) could not be genotyped since they did not match any sequence of the included genotypes. It is worth noting that the positivity of HPV DNA infection was highest in the age group of 21–30 years, while for the Mycoplasma/Ureaplasma sp., the rate of positivity varied strongly with age, with a first peak in the age group 21–30 years, and a second peak in the age group 41–50 years (Table 1).
The association of HPV infection with positivity for Mycoplasma/Ureaplasma spp. was analyzed. Overall, women positive with multiple Mycoplasma/Ureaplasma spp. were positively associated with HR-HPV infection (P = 0.007; odds ratio [OR] = 3.67, 1.47–9.13) (Table 2). However, the analysis by species showed that only M. hominis and U. urealyticum were correlated significantly with HR-HPV infection (P = 0.030 and P = 0.003, respectively) (Table 2). The relationship between M. genitalium and HPV was not analyzed due to the low number of samples positive for this pathogen in the studied population.
Genital association between human papillomavirus (HPV) and Mycoplasma/Ureaplasma spp. in a population of 258 healthy women.
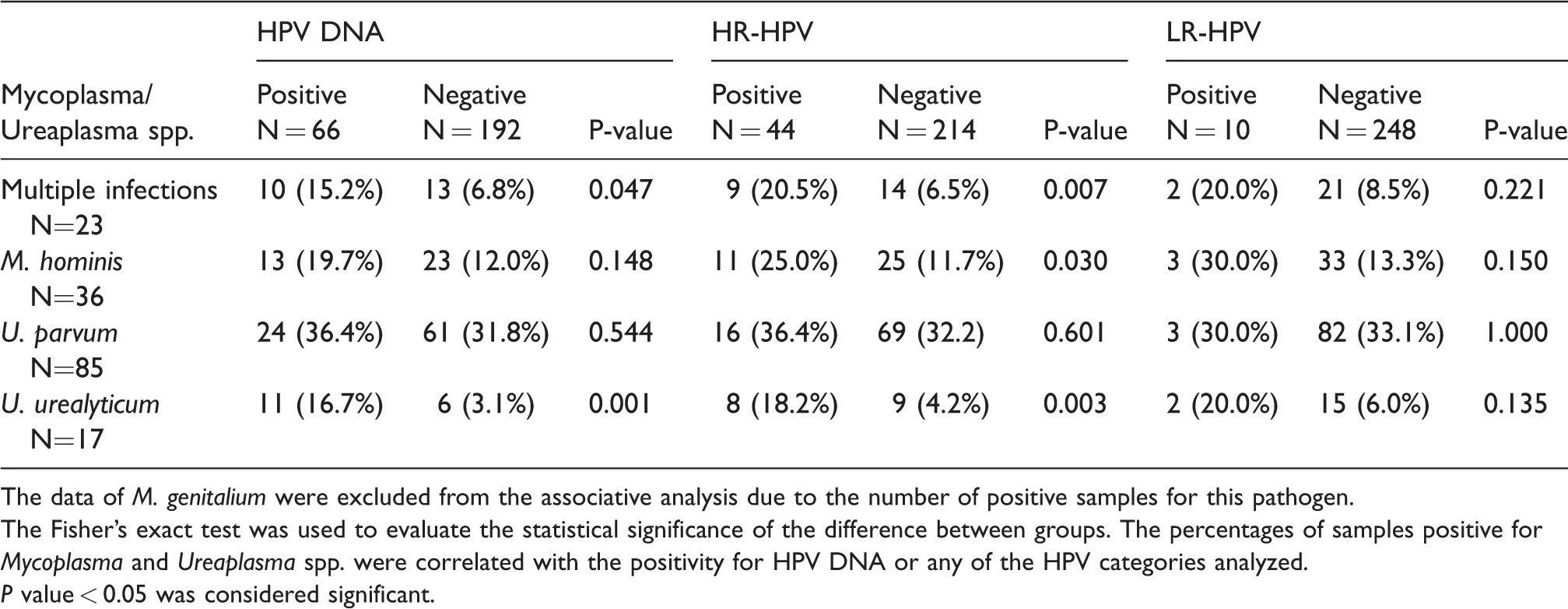
The data of M. genitalium were excluded from the associative analysis due to the number of positive samples for this pathogen.
The Fisher’s exact test was used to evaluate the statistical significance of the difference between groups. The percentages of samples positive for Mycoplasma and Ureaplasma spp. were correlated with the positivity for HPV DNA or any of the HPV categories analyzed.
P value < 0.05 was considered significant.
The cytological characteristics of the samples were as follows: half of the samples were negative for intraepithelial lesions and malignancy (53.4%, 138/258); of those samples, 91.3% (126/138) were normal and 8.7% (12/138) presented changes indicating IR. Samples with an abnormal Pap smear result (46.5%, 120/258) included ASC-US (43.3%, 52/120), LSIL (50%, 60/120), ASC-H (5.8%, 7/120), and HSIL (0.8%, 1/120). Due to the low numbers of ASC-H and HSIL cases, these categories were analyzed together (ASC-H/HSIL).
Regarding the cytological evaluation, although the positivity for HR-HPV increases according to the severity of premalignant lesions (P = 0.005), its association was statistically significant only in the ASC-H/HSIL group (P = 0.001) (Table 3). The positivity for U. parvum (P = 0.019) and/or M. hominis (P = 0.034) was significantly higher in samples with cervical IR. In addition, U. parvum was the most commonly identified bacterium in samples with abnormal cervical cytology (33.3%, 40/120). Nonetheless, there were no statistically significant differences in its distribution with respect to abnormal cytology categories analyzed (ASCUS, LSIL, and ASC-H/HSIL) (Table 3). Conversely, the prevalence of U. urealyticum was significantly higher in samples with LSIL than in normal samples (P = 0.029), while M. hominis was more frequently detected in women with ASC-H/SIL (P = 0.046) (Table 3).
The association between HPV and Mycoplasma/Ureaplasma spp. was evaluated regarding the cytological results (NILM, ASCUS, LSIL, and ASC-H/HSIL). The distribution of the HR-HPV and U. urealyticum coinfection did not show significant differences with respect to abnormal cervical outcomes detected (Table 4). Conversely, women double positive for HR-HPV and M. hominis correlated significantly with high-grade lesions (P = 0.037) (Table 4).
Distribution of human papillomavirus (HPV) and Mycoplasma/Ureaplasma spp. according to cervical cytological results in a cross-sectional study of 258 healthy women.
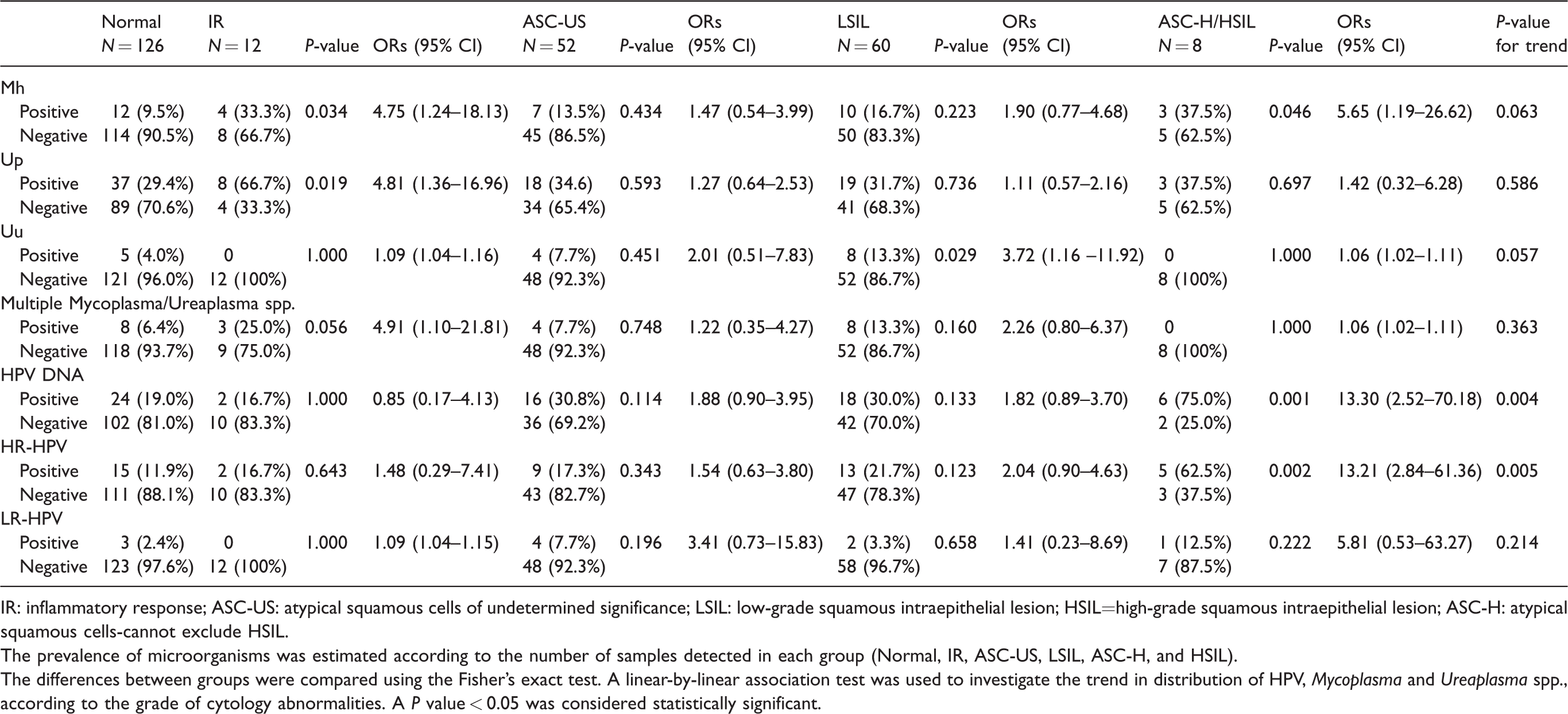
IR: inflammatory response; ASC-US: atypical squamous cells of undetermined significance; LSIL: low-grade squamous intraepithelial lesion; HSIL=high-grade squamous intraepithelial lesion; ASC-H: atypical squamous cells-cannot exclude HSIL.
The prevalence of microorganisms was estimated according to the number of samples detected in each group (Normal, IR, ASC-US, LSIL, ASC-H, and HSIL).
The differences between groups were compared using the Fisher’s exact test. A linear-by-linear association test was used to investigate the trend in distribution of HPV, Mycoplasma and Ureaplasma spp., according to the grade of cytology abnormalities. A P value < 0.05 was considered statistically significant.
Association between human papillomavirus (HPV) and Mycoplasma/Ureaplasma spp. in 258 Mexican women with abnormal cervical cytology outcomes.
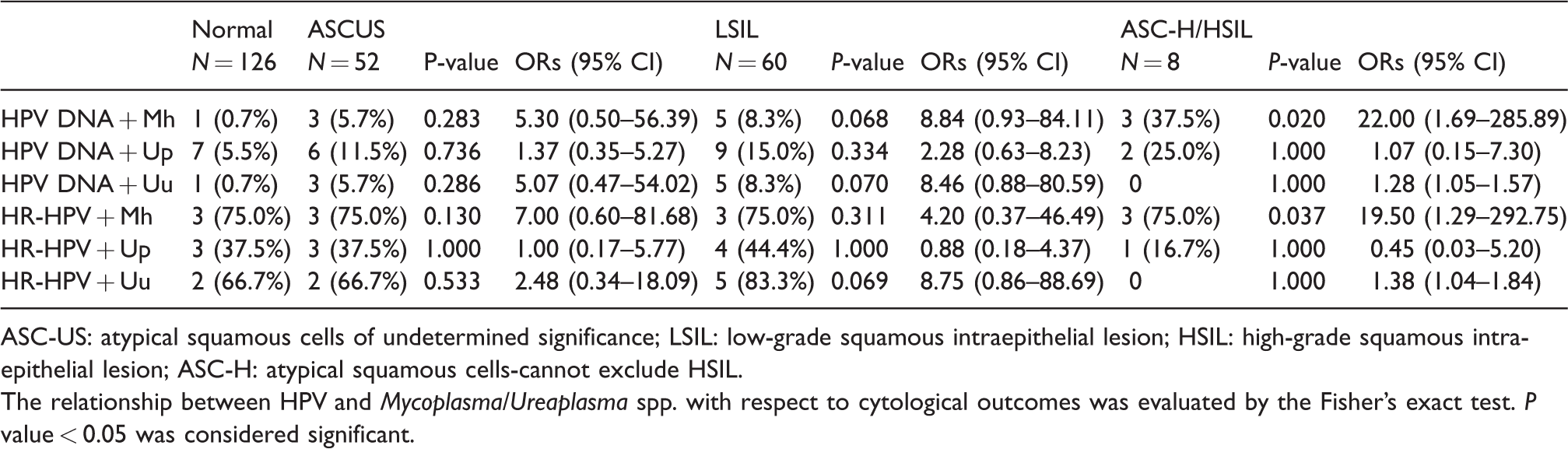
ASC-US: atypical squamous cells of undetermined significance; LSIL: low-grade squamous intraepithelial lesion; HSIL: high-grade squamous intraepithelial lesion; ASC-H: atypical squamous cells-cannot exclude HSIL.
The relationship between HPV and Mycoplasma/Ureaplasma spp. with respect to cytological outcomes was evaluated by the Fisher’s exact test. P value < 0.05 was considered significant.
Discussion
Genital colonization with certain Mycoplasma/Ureaplasma spp. has been associated with an increased risk of contracting HPV infection and with a higher probability of viral persistence, which may play a determining role in HPV-mediated cervical carcinogenesis. In this study, we evaluated the positivity for Mycoplasma/Ureaplasma spp. using nucleic acid amplification tests (NAATs) in cervical samples from healthy women to investigate their possible association with HPV infection.
The prevalence of Mycoplasma/Ureaplasma spp. varies widely depending on the studied population and methods employed for their detection. Among the Mycoplasma spp. identified in the genitourinary tract, the prevalence of M. hominis (<11.5%) is commonly higher than that of M. genitalium (<7%) in low-risk populations.19,20 This difference was partially explained by the severity of symptoms caused by M. genitalium infection, which encourages the search for a clinical evaluation, thus reducing its transmission. The proportion of women positive for M. hominis (14%) reported in this study was similar to that reported previously among asymptomatic women.19,21,22 In the case of M. genitalium, its prevalence (0.8%) was lower than that reported previously in asymptomatic women but similar to the infection rate observed in low-risk populations (∼1%).10,11 Regarding Ureaplasma spp., U. parvum (32.9%) was almost fivefold more prevalent than U. urealyticum (6.6%), which is similar to other studies conducted in European and Asian communities with healthy women.21–23
Regarding viral infection, the proportion of women positive for HPV DNA in this population (25.6%) was similar to that in other studies that evaluated its prevalence through consensus primers for L1 amplification.9,24 In agreement with the recently reported data from the Centers for Disease Control and Prevention (CDC), infection with HR-HPV was detected in less than 20% of women, 25 a finding that is also comparable to studies conducted among healthy women recruited during their routine gynecological examination.23--26
The role of Mycoplasma/Ureaplasma spp., as a cofactor for cervical carcinogenesis induced by HPV infection, is mainly related to the finding that some Mycoplasma/Ureaplasma spp. are strongly associated with chronic inflammatory processes.11,27,28 Consistent with this proposal, the presence of markers of IR in cervical cytology was significantly associated with U. parvum (P = 0.019) and/or M. hominis (P = 0.034). However, neither U. parvum nor M. hominis correlated significantly with abnormal cytological results (AS-CUS and LSIL). A possible explanation for this finding is that the cervical IR observed in samples positive to U. parvum could be activated by the primary interaction between the pathogens and cervicovaginal microbiota, which resolve spontaneously once microbial homeostasis is restored.
The relationship between U. parvum and HPV infection has been reported in few studies.9,22,29 Overall, the statistical significance of this association is limited exclusively to the prevalence of HPV DNA4,9,22 since the analysis with HR-HPV reported by other studies was not significant.4,21 The results of the study showed that the association between U. parvum and HR-HPV was not significant, even in samples with an abnormal cervical cytology, a finding similar to those results reported previously. It is worth mentioning that the geographical distribution of certain HR-HPVs could play an important role in the possible interaction between U. parvum and HR-HPV during cervical carcinogenesis. In studies where the coinfection with U. parvum and HR-HPV has been associated with an increased risk of developing cervical lesions, HPV16 and HPV31 occupy the first places of prevalence, while the studied population shows a high rate of viral infection attributed to HPV16 and HPV52.8,30 However, further studies are required to elucidate the significance of this coinfection.
The epidemiological evidence indicated that concomitant infection with U. urealyticum represents a risk factor for HPV infection and the progression of cervical premalignant lesions.4,9,10,22 In the present study, the positivity to U. urealyticum was correlated significantly with HPV infection (P = 0.001). However, the analysis regarding the epidemiological classification of HPV showed that only infection with high-risk genotypes was associated with U. urealyticum (P = 0.003). These results are on par with cross-sectional studies conducted in European countries,9,10,22 but they differ from studies conducted with Asian populations, where no relationship was detected between U. urealyticum and HR-HPV infection.21,26 The increased prevalence of U. urealyticum in women with an abnormal cervical cytology was associated with a high probability of interaction with HR-HPV in lesions of greater severity.9,10 The results of the present study showed the same trend with respect to the high prevalence of U. urealyticum in low-grade lesions, although its association with HR-HPV in women with LSIL was not significant (P = 0.069). These differences could be associated with the fact that the studies conducted by Lukic et al.10 and Biernat-Sudolska et al.9 included a greater number of high-grade cervical lesions in addition to the criteria employed for the diagnosis of U. urealyticum infection (>104 Colony Forming Units).
M. hominis is commonly considered a commensal organism of the genital tract that, under certain circumstances (e.g., immunosuppression), stimulates the production of pro-inflammatory cytokines (IL-1B) and modifies the structure of the cervical epithelium to facilitate colonization with other pathogens.31–33 Most of the studies that have investigated the relationship between M. hominis and HR-HPV have failed to find a positive association between them.9,22 According to the presented results, the overall prevalence of M. hominis correlated significantly with HR-HPV infection (P = 0.030). Moreover, the association of M. hominis with HR-HPV infection was notable in only women with ASC-H/HSIL. According to the follow-up study reported previously by Adebamowo et al., 32 the persistence of M. hominis was associated with an increased risk of having a persistent HR-HPV infection. Recently, Klein et al. 34 observed that the density of Mycoplasma/Ureaplasma spp. in the cervical microbiome of women with precancerous lesions increases with respect to the severity of cervical lesions. In addition to women with HPV infection having different bacterial communities, it is suggested that Mycoplasma/Ureaplasma spp. are part of bacterial communities that increase the risk of developing precancerous lesions. The coexistence of these microorganisms does not necessarily imply a synergistic effect on the risk of developing cervical dysplasia since other pathogens could be related to the persistence of both infections (e.g., pathogens associated with bacterial vaginosis).
This study has some limitations that should be considered. The high percentage of samples positive for HPV DNA that could not be identified with the included primers and reduced number of low-risk genotypes analyzed could cause bias with the results of the study. On the other hand, it is important to mention that other risk factors related to sexual behavior or reproduction were not recorded during the recruitment. In addition, it is worth noting the reduced number of ASC-H and HSIL cases employed for the analysis.
In conclusion, the results support the proposal that concomitant infection with U. urealyticum and HPV is a finding commonly observed in the female genital tract and is associated mainly with infection with HR-HPV genotypes. Conversely, the association of M. hominis with HR-HPV in women with high-grade cervical lesions could be associated with an increased risk of viral persistence and progression to high-grade lesions. However, follow-up studies are required to clarify the cause–effect relationship of this association. These results highlight the importance of the simultaneous detection of colonizing microorganisms of the genital tract as a strategy to reduce the risk of concomitant coinfections that potentiate their pathogenic mechanisms and increase the risk of generating adverse clinical outcomes, such as cervical dysplasia or obstetric complications.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the National Council on Science and Technology (CONACYT) (Grant number 2011-01-167762).