
Abstract
Syphilis and human immunodeficiency virus (HIV) co-infection is expected to play a role in HIV-1-related immunodeficiency progression; however, studies involving syphilis/HIV co-infection have not been conclusive. We investigated the factors associated with co-infection of syphilis and HIV and to assess the effect of syphilis on HIV progression in the context of HIV-1 diversity in an observational cohort of 246 newly-diagnosed HIV-infected but antiretroviral therapy-naive men who have sex with men enrolled in Guangzhou, China between 2008 and 2012. CD4+ cell counts of all the participants were measured from the time of diagnosis until 2015 with an average of 32 ± 18 months. Logistic analysis indicated that patients with syphilis/HIV co-infection were more likely to be older with an adjusted odds ratio (AOR) of 2.48 (95% CI: 1.28–4.80) for those aged between 31 and 40 years and 3.20 (1.11–9.22) for those aged ≥40 years as compared to 16–30 year-olds. The AOR of patients infected with HIV-1 CRF07_BC as compared to CRF01_AE was 2.14 (95% CI: 1.01–4.53). Co-infection of syphilis and HIV was associated with lower baseline CD4+ cell count (0.45, 95% CI: 0.22–0.94), but was not associated with HIV disease progression (HR: 1.03; 95% CI, 0.86–1.23) based on Kaplan–Meier analysis. Our results provide new evidence about the interaction between syphilis and HIV and indicate differential rates of immunodeficiency progression as a function of HIV-1 genetic diversity.
Introduction
Co-infection with human immunodeficiency virus (HIV) and syphilis is becoming more frequent since they share a common mode of transmission, particularly among men who have sex with men (MSM). 1 In the United States, syphilis continues to be a growing epidemic among HIV-infected MSM in the past two decades. 2 MSM accounted for 58% of all primary and secondary syphilis cases, and 47% of MSM with syphilis had HIV in 2016. 3 Since 2000, more syphilis cases have been identified in MSM in Europe due to the incorporation of serologic testing for syphilis in routine monitoring of HIV-positive MSM.4,5 Thus, as of 2016, approximately 63% of new syphilis cases in Europe were among MSM. 6 In China, a nation-wide survey between 2008 and 2009 revealed that 4.9 and 11.8% of the MSM population were infected with HIV and syphilis, respectively. Furthermore, 12.5% of syphilis-positive MSM were HIV-positive. 7 The co-infection of HIV and syphilis is also common in other Asian countries with a prevalence of syphilis ranging from 5 to 33% among HIV-infected MSM.8–10
The interaction of HIV and syphilis is complicated and not fully understood. Syphilis appears to facilitate acquisition and transmission of HIV due to the high incidence of genital ulcers, and probably the immunoregulatory effects of Treponema pallidum (TP).11–13 Furthermore, syphilis co-infection might adversely affect the course of HIV infection. Buchacz et al. 14 found that in a retrospective study of 52 men in San Francisco, syphilis induced a 0.22 log increase in HIV RNA and a fall of CD4 cell count by 62 cells/mm3. Similar results have been reported among patients co-infected with HIV and syphilis, in particular among primary and secondary syphilis patients. 15 However, it has also been previously reported that among syphilis/HIV co-infected MSM, syphilis induces a relative non-CD4+ T cell-specific lymphopenia and only resulted in an increase of HIV viral load (VL) in 10.7% of the studied patients. 16 In addition, there is less information on the effects of syphilis on HIV disease progression. A recent study has shown that syphilis did not affect the time of HIV infection to the acquired immunodeficiency syndrome (AIDS)-defining conditions in a US military cohort of 2239 HIV-infected persons. 17 Our results and Vasan et al.’s 18 report showed that HIV-1 genotypes were associated with disease progression. Therefore, in the current study, we sought to determine the risk factors associated with HIV/syphilis co-infection in a newly diagnosed HIV-infected MSM cohort population and to address the role of syphilis in HIV immunodeficiency progression in the context of HIV-1 diversity.
Methods
Study population and demographic data
This retrospective observational study included 246 newly-diagnosed cases of HIV-1 and/or syphilis-infected MSM from Guangzhou Center for Diseases Prevention and Control (CDC) in China between January 2008 and December 2012. The subjects were diagnosed in the CDC-certified clinics or hospitals and follow-up examinations were done from June 2008 to February 2015 with patients visiting every 3–6 months. China’s National Free Antiretroviral Treatment Program provides free-of-charge care to HIV-infected subjects including consulting, CD4 cell measurements every 3–6 months, and antiretroviral therapy (ART) in those with CD4 cell count <350 cells/mm3 before June of 2016 and since then in all individuals living with HIV-1 infection regardless of clinical and immunological status. For cross-sectional analysis of risk factors for HIV/syphilis co-infection, all the HIV-infected subjects who met the following criteria were included: (1) contracted HIV through homosexual transmission, (2) had not received ART, (3) were 16 years or older. For longitudinal analysis to evaluate the effect of syphilis on HIV immunodeficiency progression, subjects also satisfied two other requirements in addition to the above-stated requirements: (1) baseline CD4+ T cell counts were higher than 200 cells/mm3 at enrollment; and (2) at least two measurements of CD4+ T cell count were available during follow-up. Demographic and laboratory testing data were collected from the medical charts of Guangzhou CDC or from China Information System for Disease Control and Prevention. Informed consent forms were obtained. This study was approved by the Institutional Review Board of Guangzhou CDC (No. 2017030).
Laboratory analysis
HIV infection was determined by means of enzyme-linked immunosorbent assay (BioMérieux, Marcy I’Etoile, France) and confirmed by Western blot analysis (MP Diagnostics, Geneva, Switzerland). 19 CD4+ T cell count was measured by BD Tritest™ CD4/CD8/CD3 Trucount Tubes (Becton Dickinson, Franklin Lakes, USA). 19 HIV-1 genotypes were determined based on phylogenetic analyses of partial pol sequences as previously reported. 20 Syphilis was diagnosed with toluidine red unheated serum test (TRUST, Wantai Biological Pharmacy, Beijing, China) and TP particle agglutination assay (TPPA, Lizhu Biological Medicine, Zhuhai, China). Previous syphilis infection was defined as TRUST−, TPPA+ whereas active syphilis was defined as both TRUST and TPPA positive. In our study, syphilis was defined as TPPA+. HIV-infected patients who were seropositive for syphilis at the time of HIV-1 diagnosis were classified as syphilis and HIV co-infection.21,22
Outcome measurement
HIV disease progression was measured by two endpoints: (1) immunological progression, which was defined as the decrease of CD4+ T cell count from ≥350 to <350 cells/mm3, and (2) immunodeficiency, i.e. CD4+ T cell count of fewer than 200 cells/mm3 according to U.S. CDC criteria or WHO standards. 23 The time of immunological progression was estimated as the mid-point between the last date of CD4+ T cell count ≥350 cells/mm3 and the first date of CD4+ T cell count <350 cells/mm3. The time of immunodeficiency was estimated as the mid-point between the last date of CD4+ T cell count ≥200 cells/mm3 and the first date of CD4+ T cell count <200 cells/mm3. Subjects were censored if they were lost to follow-up, died, initiated ART, or failed to progress to the endpoint at the date of the last recorded visit, whichever occurred first.
Statistical analysis
SPSS version 22.0 (SPSS Inc., Chicago, IL, USA) was used to perform the statistical analysis. Baseline characteristics were analyzed by Chi square test or Fisher’s exact test for categorical variables. The independent variables including age, marital status, education level, STI history, number of sexual partners, HIV-1 genotype, baseline CD4+ cell count, and the time of HIV diagnosis were analyzed by Chi square test or Fisher’s exact test. Missing data were imputed using multiple imputations. Risk factors for syphilis/HIV co-infection were further confirmed by logistic regression models. Candidate variables that reached p-value of <0.1 on univariate analysis or have been reported involving syphilis co-infection in previous literature were sequentially included in a binary multivariate model to estimate the association with syphilis/HIV co-infection. The models were built using the maximum likelihood ratio test based on the stepwise forward method. Kaplan–Meier survival curve analysis and the log-rank test were used to compare survival curves with corresponding 95% confidential interval (CI). Cox proportional hazards regression analysis was adapted to estimate potential risk factors of immunological and immunodeficiency progression.
Results
General characteristics of the study population
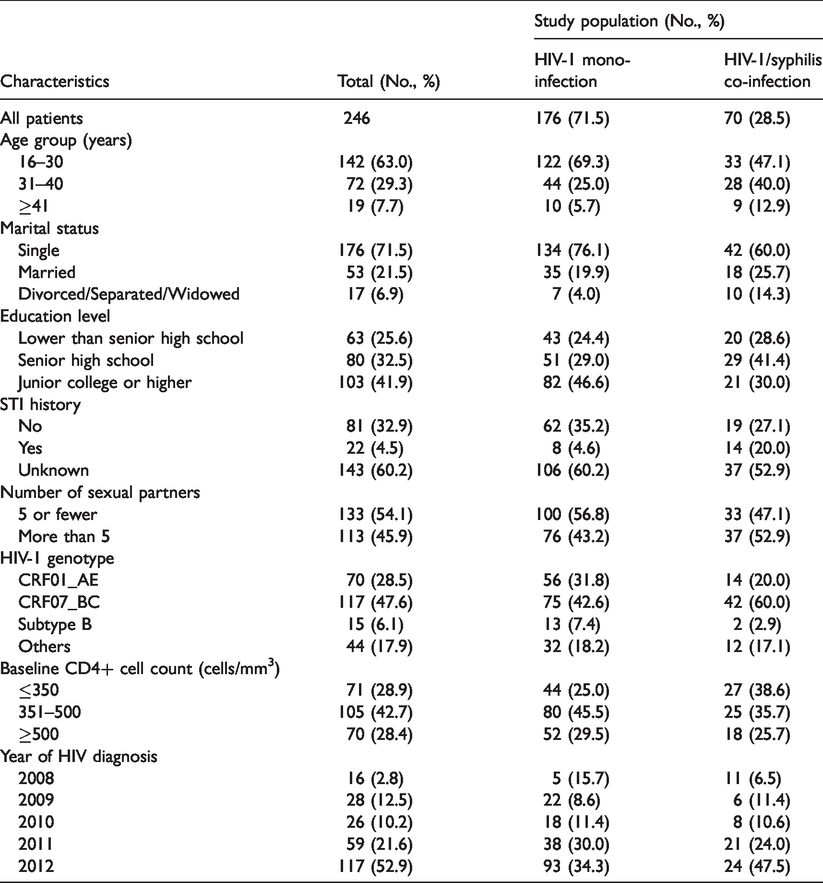
A total of 246 HIV-infected MSM were included in our study. Among them, 70 (28.5%) were seropositive for syphilis and were considered as co-infected with HIV and syphilis. Majority of the participants were between 16 and 30 years old (63.0%) and unmarried (71.5%). Approximately 41.9% of them had received basic education up to junior college. About 45.9% had more than five sexual partners whereas 4.5% had a history of sexually transmitted infections (STIs). In addition, 28.9% had a CD4+ T cell count of ≤350 cells/mm3. CRF01_AE and CRF07_BC were the dominant HIV-1 genotypes and accounted for 28.5 and 47.6%, respectively (Table 1). When comparing MSM with HIV single infection alone and HIV/syphilis co-infection, statistically significant differences were observed with respect to age, marital status, and STI history and year of HIV diagnosis (Table 1, P < 0.05). In addition, marginal differences were observed for education level and HIV-1 genotypes (Table 1).
Demographic characteristics of HIV-infected MSM included between 2008 and 2012 in Guangzhou, China.
Factors associated with HIV and syphilis co-infection
The risk factors associated with HIV/syphilis co-infection were further analyzed by logistic regression analysis (Table 2). Both univariate and multivariate analyses indicated that age, STI history, HIV-1 genotype, and baseline CD+ T cell count were associated with HIV/syphilis co-infection. The age of the patient was associated with HIV/syphilis co-infection, with an adjusted odds ratio (AOR) of 2.48 (95% CI: 1.28–4.80) for those aged between 31 and 40 years and 3.20 (1.11–9.22) for those >40 years when compared to the 16–30-year age group. Among those with a history of STIs, a high AOR of 6.56 (95% CI: 2.21–19.53) was observed for HIV/syphilis co-infection. HIV-1 CRF07_BC infection (AOR 2.14; 1.01–4.53) was also associated with HIV/syphilis as compared to CRF01_AE. In addition, a baseline CD4+ T cell count of >350 cells/mm3 had an approximately 2.2-fold lower risk of HIV/syphilis co-infection compared to baseline CD4+ T cell count of ≤350 cells/mm3 (0.45; 0.22–0.94) (Table 2).
Factors associated with syphilis/HIV-1 co-infection among MSM between 2008 and 2012 in Guangzhou, China.
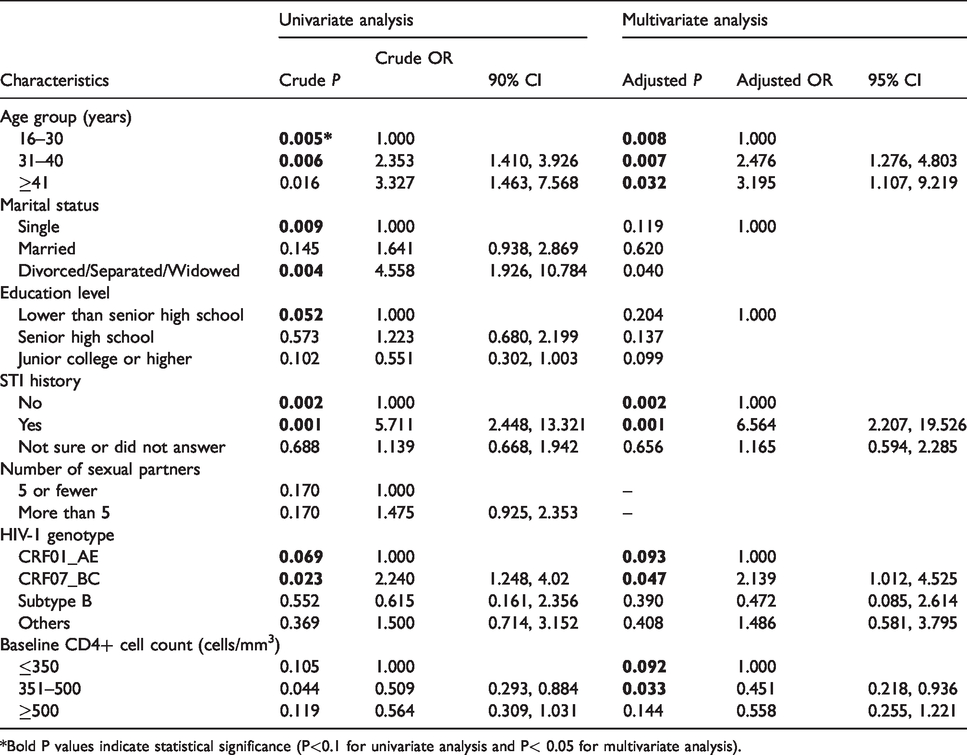
*Bold P values indicate statistical significance (P<0.1 for univariate analysis and P< 0.05 for multivariate analysis).
Factors associated with immunological or immunodeficiency progression
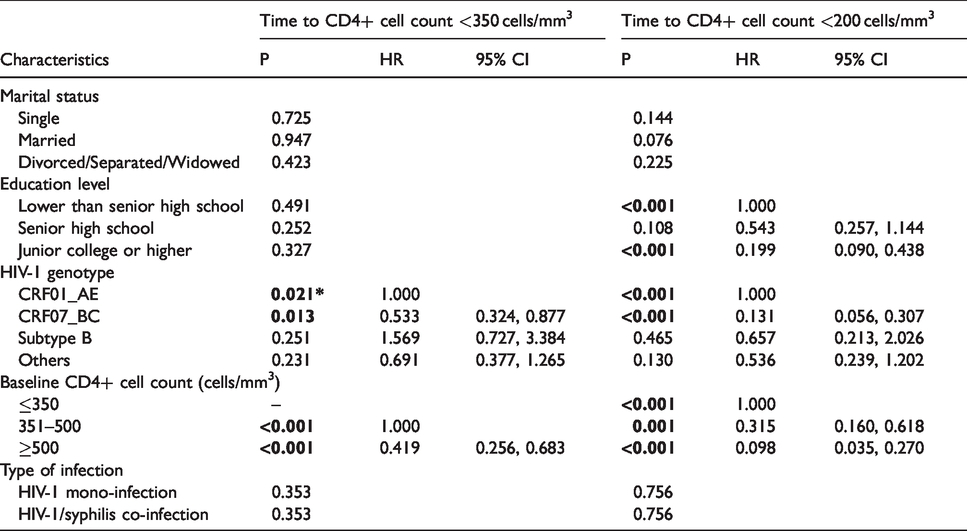
Immunological studies among participants were followed up for 32 ± 18 months. Both univariate and multivariate Cox regression analysis indicated that baseline CD4+ T cell count and HIV-1 genotype were associated with immunological progression (i.e. decrease of CD4+ T cell count from >350 to <350 cells/mm3, p < 0.01, Tables 3 and 4). Compared with those with baseline CD4+ T cell count of 351–500 cells/mm3, subjects with baseline CD4+ T cell count >500 showed 2.4-fold lower risk of developing immunological progression (AOR = 0.42; 95% CI 0.26–0.68, Table 4). In addition, infection of HIV-1 CRF_07BC showed 1.9-fold lower risk of immunological progression than CRF01_AE (0.53; 0.32–0.88, Table 4). During the period of observation, subjects with HIV-1 infection alone developed immunological progression more frequently than those co-infected with HIV and syphilis (52.6% versus 39.5%), but the difference was not significant (P = 0.184, Table 3). Furthermore, Cox regression analysis did not find a statistically significant association between HIV/syphilis co-infection and immunological progression (P = 0.353, Table 4). Kaplan–Meier curve analysis also showed no difference in the rates of progression between the two groups (HR, 0.70; 95% CI, 0.43–1.13) (Figure 1(a)).
Univariable Cox regression analysis for the time to immunological progression or immunodeficiency in Guangzhou, China during 2008–2015.
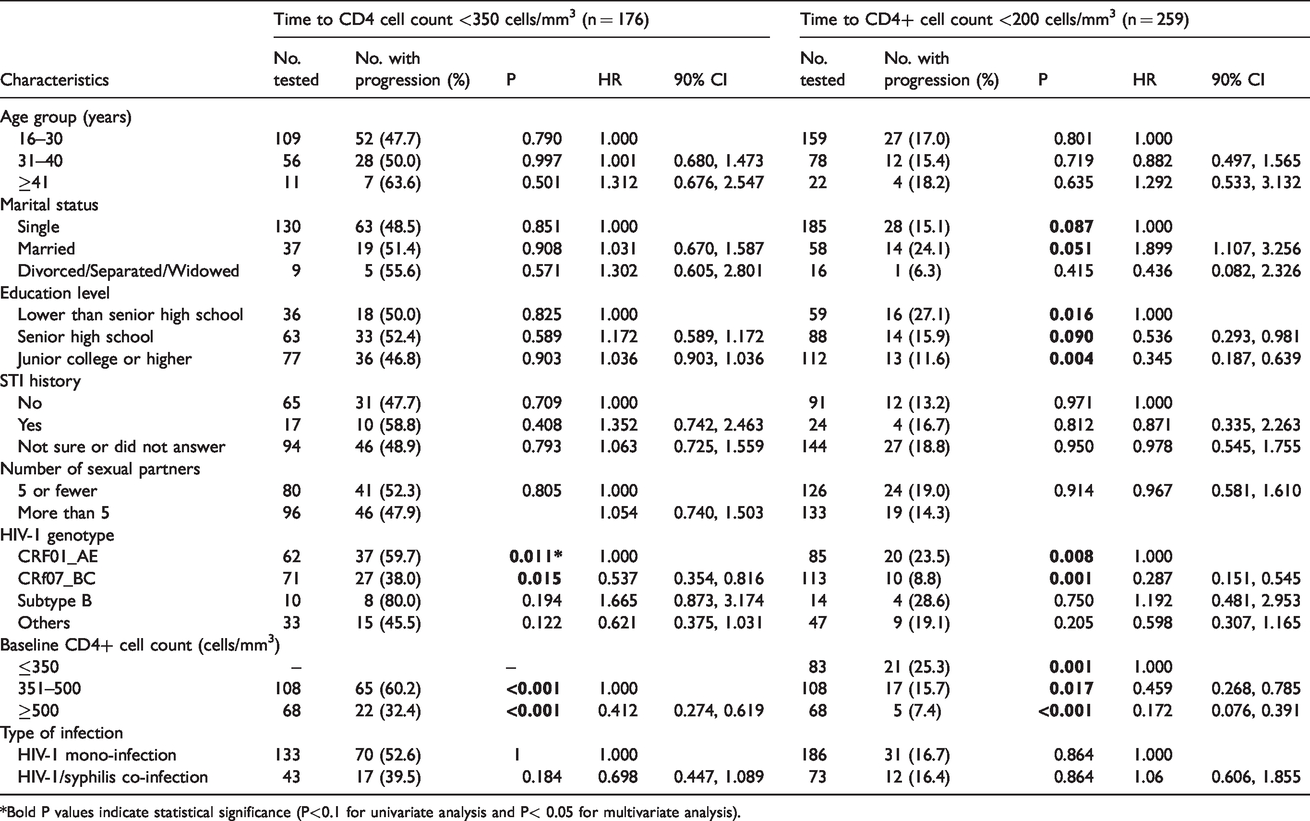
*Bold P values indicate statistical significance (P<0.1 for univariate analysis and P< 0.05 for multivariate analysis).
Multivariable Cox regression analysis for time to immunological progression or immunodeficiency in Guangzhou, China during 2008–2015.

Kaplan–Meier analysis of time from HIV diagnosis to immunological progression (a) and immunodeficiency (b). Immunological progression or immunodeficiency was defined as CD4 <350 cells/mm3 or <200 cells/mm3, respectively. The date of HIV diagnosis was defined as time point zero. Tick marks indicate participants with censored data. P values were calculated by the log-rank test.
Similar results were obtained for the analysis of immunodeficiency, i.e. CD4+ T cell count of <200 cells/mm3. Kaplan–Meier analysis (Figure 1(b)) showed no significant difference with respect to the rate of immunodeficiency progression (HR, 1.03; 95% CI, 0.86–1.23) between subjects with HIV infection alone and HIV/syphilis co-infection. Furthermore, multivariable Cox regression analysis indicated that slower immunodeficiency progression was associated with higher baseline CD4+ T cell count (0.10; 0.04–0.27 for ≥500 cells/mm3; and 0.32; 0.16–0.62 for ≥350 cells/mm3) and HIV-1 CRF07_BC (0.13; 0.06–0.31) but not HIV/syphilis co-infection (P = 0.756, Table 4).
To avoid the influence of HIV-1 genotypes on disease progression, we repeated Kaplan–Meier analysis according to HIV-1 genotypes and did not find any difference of disease progression between HIV infection alone and HIV/syphilis co-infection (Figure S1). It was only among subjects with HIV infection alone that CRF01_AE but not CRF07_BC was associated with immunodeficiency progression (OR = 3.6, 95% CI 1.414, 9.166, P = 0.003) in a case–control study (Table S1) and Kaplan–Meier analysis (p < 0.001, Figure S2).
Discussion
In our study, we identified 11.4% of HIV-infected MSM with confirmed syphilis infection. The seropositive rate of syphilis was lower than the prevalence of 33.0% among HIV-1-infected MSM reported in seven Chinese cities in 2008 but higher than the syphilis prevalence of 2.7% in the general population observed in a meta-analysis in China. 24
The risk factors for co-infection of HIV and syphilis identified in our study such as the age of patients over 30 years, having a history of STIs, and lower baseline CD4+ T cell count were consistent with a previous study. 25 Moreover, we found that HIV and syphilis co-infection was high among subjects infected with HIV-1 CRF07_BC but not CRF01_AE. It has been reported that TP can up-regulate the expression of the CCR5 co-receptor. 12 HIV-1 subtype C exhibits higher infectiousness than subtypes A, B, and D due to dependence at the CCR5 level. 26 CRF07_BC carries envelope derived from subtype C 27 and is almost all CCR5 tropic. 28 It may be more efficient in infecting CCR5-expressing cells. In addition, dendritic cells (DCs) can be activated by TP and selectively transmit R5-tropic viral isolates of HIV-1 as demonstrated in previous studies.29,30 CRF07_BC and CRF01_AE were the two major viruses among HIV-infected MSM in China. 31 These results indicated that DCs in the genital mucosa may promote infection of CD4+ T-cells by R5-tropic viruses, resulting in patients with syphilis more likely to be co-infected with HIV-1 CRF07_BC rather than CRF01_AE. This may explain the association between syphilis and HIV-1 CRF07_BC infection observed in our study.
Although syphilis may affect CD4+ T cell count and HIV VL, the influence is transient. The decreased CD4+ T cell counts are reversed after antibiotic treatment, suggesting that syphilis may not affect the progression of HIV infection. Our results further confirmed a previous finding that syphilis does not affect the progression to immunodeficiency or AIDS-defining conditions. 17 Furthermore, our study proved that HIV immunodeficiency progression was associated with HIV-1 genotypes but not syphilis. HIV-1 CRF01_AE infection was 7–8-fold more likely to result in immunodeficiency than CRF07_BC (Table 4). These results are consistent with previous findings that CRF01_AE is associated with higher VL, shorter survival, and faster progression to AIDS due to a greater frequency of X4 tropism.33-36 Furthermore, previous studies have reported that CRF07_BC showed slower progression compared to other subtypes partly due to a signature seven amino-acid deletion in the p6Gag domain. CRF07_BC with the above deletion mutation replicates less efficiently in PBMCs and shows decreased virus release and poor infectivity.37,38 However, we must emphasize that the association between CRF07_BC genotype and HIV/syphilis may be regionally dependent since CRF07_BC is mainly an epidemic of mainland China and Taiwan.
Our study was subject to limitations: (1) Syphilis diagnosis was based on serological testing and not upon clinical signs or symptoms. The laboratory diagnosis of syphilis may not be sensitive enough in all cases. In our study, syphilis was defined as positive for Treponema-specific antibody testing and hence missing cases of early syphilis may exist, in particular when the nontreponemal screening test still is nonreactive. (2) The study was one a center, retrospective study. Exact HIV and syphilis seroconversion dates were usually unavailable; therefore, the time of infection to immunological progression or immunodeficiency cannot be estimated accurately. (3) We used the surrogate marker of CD4+ T cell count rather than outcomes such as AIDS-defining illness, mortality, or opportunistic infections as endpoints due to the relatively short period of follow-up. However, HIV-1 infection mainly results in immunodeficiency and CD4+ T cell count is a reliable indicator of immune function. (4) We were unable to monitor HIV VLs for the ART-naive individuals although Sogkas et al. 16 reported that changes in HIV-1 VLs are observed only in a minority of patients and that syphilis does not affect the course of HIV infection. In addition, we did not evaluate the influence of opportunistic infections or co-infection with tuberculosis, hepatitis B virus, or hepatitis C virus. This may have influenced the clinical outcomes of this study.
In conclusion, our study demonstrated that co-infection of syphilis and HIV among MSM was more common in older people infected with HIV-1 CRF07_BC in China. Co-infection with syphilis might not affect HIV-related immunodeficiency progression. Our results provide new evidence about the interaction of syphilis and HIV and indicate differential rates of immunodeficiency progression as a function of HIV-1 genetic diversity.
Supplemental Material
STD860618 Supplemental Material1 - Supplemental material for Syphilis infection does not affect immunodeficiency progression in HIV-infected men who have sex with men in China
Supplemental material, STD860618 Supplemental Material1 for Syphilis infection does not affect immunodeficiency progression in HIV-infected men who have sex with men in China by Liping Huang, Weibin Cheng, Zhigang Han, Yuanhao Liang, Hao Wu, Haiying Wang, Huifang Xu and Shixing Tang in International Journal of STD & AIDS
Supplemental Material
STD860618 Supplemental Material2 - Supplemental material for Syphilis infection does not affect immunodeficiency progression in HIV-infected men who have sex with men in China
Supplemental material, STD860618 Supplemental Material2 for Syphilis infection does not affect immunodeficiency progression in HIV-infected men who have sex with men in China by Liping Huang, Weibin Cheng, Zhigang Han, Yuanhao Liang, Hao Wu, Haiying Wang, Huifang Xu and Shixing Tang in International Journal of STD & AIDS
Supplemental Material
STD860618 Supplemental Material3 - Supplemental material for Syphilis infection does not affect immunodeficiency progression in HIV-infected men who have sex with men in China
Supplemental material, STD860618 Supplemental Material3 for Syphilis infection does not affect immunodeficiency progression in HIV-infected men who have sex with men in China by Liping Huang, Weibin Cheng, Zhigang Han, Yuanhao Liang, Hao Wu, Haiying Wang, Huifang Xu and Shixing Tang in International Journal of STD & AIDS
Footnotes
Acknowledgement
We would like to thank Dr Emmanuel E. Dzakah for his critical review of this paper.
Authors’ contribution
ST and HX designed the study. ZH, WC, and HW collected the data. ZH and HW performed the sequencing and anti-HIV testing. LH and YL analyzed and interpreted the data. LH and YL made the tables and figures. LH and ST wrote the report. All authors reviewed, revised, and approved the final report. LH and WC contributed equally to this work.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Bureau of Science and Information Technology of Guangzhou Municipality (Project No. 201704020219, 201707010184, and 201604020011).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.