
Abstract
To maximize the public health benefits of voluntary medical male circumcision (VMMC) in real-world settings, sexual abstinence is recommended for six weeks following VMMC to ensure complete wound healing. We determined the frequency and predictors of early resumption of sex among a cohort of HIV-negative, sexually active men 18–49 years who underwent VMMC within a public-sector clinic in Botswana. Multivariate robust Poisson regression methods were used to identify predictors of having any sexual intercourse in the last six weeks since undergoing VMMC. In total, 433/519 (83%) men had data available on sexual activity at six weeks post-VMMC. Median age was 27 years, 57% had a higher than secondary education, 72% were employed, and 9% were married. Overall, 122/433 (28%) men had sexual intercourse within the six weeks since VMMC, of whom 36% reported inconsistent condom use. Compared to men ≥34 years, men aged <30 years (adjusted risk ratio [aRR] = 1.71, 95% CI 0.95–3.08) and men 30–34 years had a two-fold higher likelihood of resuming sexual activity early in multivariate analyses (aRR = 2.31, 95% CI 1.26–4.25, Wald p = 0.018). Employed men were more likely to resume sexual activity early than unemployed men (aRR = 1.58, 95% CI 1.02–2.44, p = 0.039). Additional interventions are needed to encourage abstinence until complete wound healing.
Introduction
Voluntary medical male circumcision (VMMC) reduces HIV acquisition in heterosexual men by approximately 60% with sustained effect years after the procedure, as demonstrated by a robust evidence base that includes three landmark randomized clinical trials (RCTs) and over 40 observational studies. 1 This one-time, safe, highly cost-effective, biomedical HIV prevention intervention also decreases the risk of men acquiring other sexually transmitted infections (STIs), including genital ulcer disease, syphilis, herpes simplex virus type 2, and human papillomavirus (HPV).2–4 Female partners of men who undergo VMMC also benefit by experiencing reduced rates of syphilis, HPV, bacterial vaginosis, and trichomoniasis.4,5 Promotion of VMMC in 14 African countries, prioritized for their generalized HIV epidemics and low male circumcision rates, resulted in more than 18.6 million men becoming circumcised.6–9 By 2017, those VMMCs averted an estimated 230,000 new HIV infections. 10 With global goals targeting 27 million more VMMCs by 2021, translating to 90% of males aged 10–29 years being circumcised in priority settings, VMMC is projected to prevent more than one million HIV infections by 2030. 11
The World Health Organization recommends sexual abstinence for six weeks following VMMC to ensure complete wound healing and reduce potential complications. 12 Resumption of sexual activity prior to complete wound healing may increase the risk of acquisition of HIV infection among recently circumcised HIV-negative men and may increase the risk of HIV transmission to female partners of recently circumcised HIV-positive men.13–15 Ideally, medical inspection should be conducted for confirmation that wound healing is complete, though logistical challenges prohibit this approach in programmatic settings. 12 In the three RCTs demonstrating VMMC efficacy,16–18 3.9–22.5% of participants reported early resumption of sexual activity. 19 Post-RCT implementation evaluations in Kenya, Zambia, and Tanzania found that sexual activity before complete wound healing was common, with up to 50% of men reported resumption of sexual activity within six weeks of undergoing VMMC.14,20–22 Modeling demonstrations which incorporate these data suggest that early resumption of sexual activity post-VMMC could reduce the potential population-level impact of VMMC scale-up.14,23,24
To maximize safety and ensure the public health benefits of VMMC in real-world settings, abstinence needs to be effectively promoted during the six-week period following VMMC. Identifying men most likely to resume sexual activity prior to complete wound healing could help target enhanced interventions and intensified counseling efforts. We determined the frequency and predictors of early resumption of sexual activity among a cohort of adult men who underwent VMMC within a programmatic delivery setting in Botswana.
Methods
Study design and participants
We analyzed data from a cohort study among HIV-negative, sexually active men aged 18–49 years who underwent VMMC through Botswana’s National Safe Male Circumcision program at two government-run clinics in Gaborone, Botswana. The parent study enrolled men between November 2013 and April 2015 and was designed to prospectively assess sexual behaviors and adverse events following VMMC. 25 Parent study procedures have been previously described in detail. 25 Briefly, the study was collaboratively conducted by the Botswana Ministry of Health (MOH) and the International Training and Education Center for Health, a collaboration between the University of Washington and University of California, San Francisco. Recruitment and enrollment of study participants occurred before undergoing VMMC but after individuals completed group education about the risks and benefits of VMMC, received individual counseling with clinic staff (including HIV testing), and provided written informed consent for VMMC. At enrollment, study staff collected information on demographic, clinical, relationship, and sexual behavior characteristics. All clinical VMMC activities were conducted per Botswana MOH guidelines at no cost to participants and were not part of study procedures. 26
Ethical approvals were obtained by the Health Research and Development Committee at the Botswana MOH and the University of Washington Institutional Review Board. All participants provided written informed consent for participation in the study in addition to the consent obtained by clinic staff for the circumcision procedure.
Data collection procedures
After circumcision, follow-up visits were scheduled in alignment with the Botswana MOH guidelines for adult VMMC (two days, seven days, six weeks, three months, one year). 26 At study visits, participants were asked to self-administer a questionnaire about wound care, patient satisfaction of the procedure, and resumption of sexual activities. Each study participant was provided with a wallet-size reminder card noting the date of each follow-up visit. In advance of each visit, study staff telephoned participants to remind them of the upcoming visit. At each follow-up visit, study staff performed a physical examination, including inspecting the circumcision site, and assessing for signs of STIs. Participants received BWP100 (approximately USD$8 at study initiation) at each follow-up visit as reimbursement for time and travel costs. In the event of a missed visit, study staff made telephone calls to reschedule the appointment.
Statistical analysis
The current analysis on earlier resumption of sex was restricted to men who had data available from six weeks post-VMMC, an approach comparable to previously published studies on early resumption of sexual activity.20,21,27 We identified differences between men with and without sexual activity data available at six weeks post-VMMC using Chi square test for proportions and Kruskal–Wallis for continuous measures. The primary outcome of the current analysis was early resumption of sex, defined as any sexual intercourse in the six weeks following the VMMC procedure (yes/no). Descriptive statistics were used to summarize the frequency, timing, and characteristics of early sexual activity resumption. We tested the following enrollment characteristics as potential predictors of early sexual activity resumption: demographic information (age, education, relationship status, employment, electricity in household), behavior (alcohol consumption, age of sexual debut, number of sexual partners [lifetime, last 12 months], relationship type [regular/casual], history of buying sex, and condom use), and primary motivation for VMMC (HIV prevention versus other reasons). Variables were identified as predictors using univariate Poisson regression models with robust error variance, an approach used when the outcome prevalence is not rare (e.g. >10%).28,29 Variables significant at p < 0.10 were included in the multivariate Poisson models. We decided a priori to adjust all multivariate models by age and employment based on prior studies which identified these variables as predictors of early resumption of sexual activity following VMMC. 20 Additionally, we conducted an exploratory analysis to identify predictors of very early resumption of sex by repeating our primary models using the outcome of any sexual intercourse within three weeks following the VMMC procedure (yes/no). We used Stata 15/SE (Stata Corporation, College Station, TX) to perform statistical analyses.
Results
Baseline characteristics
In total, 519 who were enrolled in the parent study underwent VMMC (Figure 1). Median age was 27 years (interquartile range [IQR] 23–31), 57% had completed secondary education or higher, and 86% had electricity in the household. The most common relationship status was dating and not living together with partners (53.4%) followed by dating and living together (18.9%); being married was less common (8.6%). Over one-third (37%) of men reported having ≥6 drinks at one time at least four times in a month. The median age of sexual debut was 19 years (IQR 17–20), 20% of men reported having ≥2 sexual partners in the last month, and 21% reported ≥10 lifetime sexual partners. Almost one-half (47%) reported that HIV prevention was their primary reason for becoming circumcised.

Study flowchart for men who underwent VMMC and were enrolled in the parent study between November 2013 and October 2015.
Overall, 433/519 (83%) men had data available on sexual activity at six weeks post-VMMC (Figure 1); 70/519 (14%) men did not return for a six-week visit and 16/449 (4%) who did return did not have data on sexual activity. Compared to men without six weeks post-VMMC sexual activity data available, men with data available were more frequently employed (72% versus 62%, p = 0.047) and more frequently had a casual sexual partner (91% versus 81%, p = 0.017). There were no differences in any other baseline characteristics between those who did and who did not have six-week sexual activity data available (Table 1).
Baseline characteristics of HIV-uninfected men who underwent VMMC, by availability of sexual activity data at six weeks post-VMMC.

IQR: interquartile range; VMMC: voluntary medical male circumcision.
*p < 0.05.
Early resumption of sexual activity
Among men with data available on sexual activity at six weeks post-VMMC (n = 433), 122 (28%) reported having sexual intercourse within the last six weeks (Figure 2). Of those who resumed sexual activity (n = 122), over one-half (52%) reinitiated sex in the first four weeks after undergoing VMMC (Figure 2). The median number of sex acts since VMMC was two (IQR 2–4, absolute range 1–14), and 34% initiated sex themselves; 11 and 55% reported it was a partner who initiated sex or that it was mutual, respectively. Most men who resumed sexual activity engaged in vaginal sex (116/122, 95%); among those who had vaginal sex, 42/116 (36%) reported not wearing a condom every time. Frequency was lower for engaging in oral sex (21/122, 17%) and anal sex (5/122, 4%); 20/122 (16%) engaged in more than one type of sex (vaginal, oral, and/or anal) and 4/122 (3%) engaged in all three types.
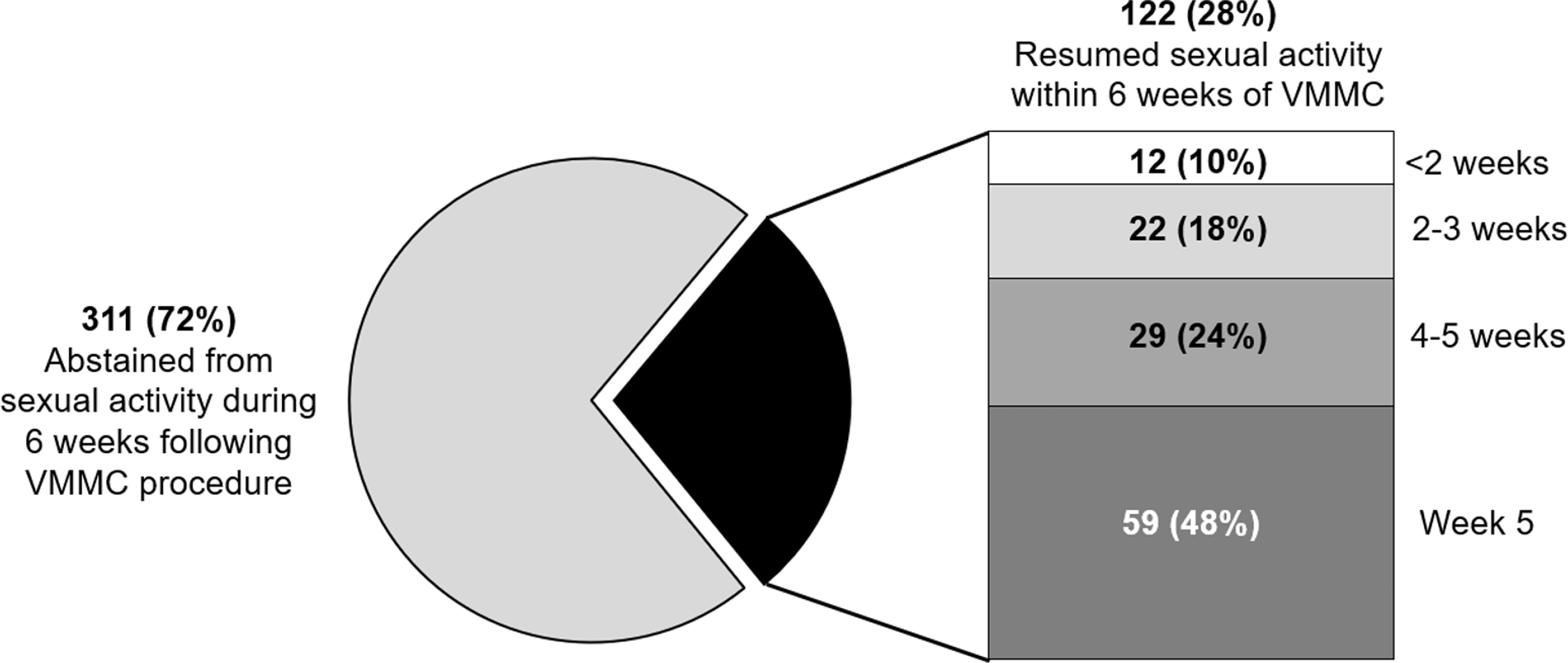
Early resumption of sexual activity following VMMC procedure (n = 433). VMMC: voluntary medical male circumcision.
In univariate analyses, younger age, being employed, having a regular partner, and inconsistent condom use with regular partners were associated with early resumption of sexual activity (Table 2). Being married was not associated with early resumption of sexual activity in univariate analyses (risk ratio [RR]=1.09, 95% CI 0.65–1.84, p = 0.739) nor was living with a partner (RR = 1.21, 95% CI 0.86–1.69, p = 0.266). Compared to men ≥34 years, men aged <30 years (adjusted risk ratio [aRR] = 1.71, 95% CI 0.95–3.08) and men 30–34 years had a two-fold higher likelihood of resuming sexual activity early in multivariate analyses (aRR=2.31, 95% CI 1.26–4.25, multivariate Wald p = 0.018). Employed men were more likely to resume sexual activity early than unemployed men, adjusting for age (aRR = 1.58, 95% CI 1.02–2.44, p = 0.039). After adjustment for age and employment, men who reported inconsistent condom use with regular partners at baseline were also more likely to resume sexual activity (aRR = 1.51, 95% 1.01–2.26, p = 0.045). We did not detect significant associations with any other characteristics in multivariate analyses (Table 2). In an exploratory analysis to identify predictors of very early resumption of sex, we found that employed men were over three times more likely to resume sex within three weeks post-VMMC procedure after adjusting for age (aRR = 3.45, 95% CI 1.27–9.41, p = 0.016). No other characteristics were associated with very early resumption of sex (data not shown).
Predictors of sexual activity resumption before six weeks following VMMC among adult men in Botswana (n = 433). a

Adj: adjusted; RR: risk ratio; VMMC: voluntary medical male circumcision.
*p < 0.05; Wald test p-value for categorical variables.
aIncludes men who had data available on resumption of sexual activity at six weeks post-VMMC procedure.
All multivariate models adjusted for age and employment.
Includes married men who live or do not live with their wives.
Includes married men who live with their wives or unmarried men who live with their partner.
Discussion
In this longitudinal study of men who became circumcised within a programmatic VMMC setting in Botswana, we found that nearly one-third of men resumed sexual activity prior to the recommended six weeks post-procedure. Men ≤34 years and those who were employed were more likely to resume sexual activity early in our study. We also found that inconsistent condom use with regular partners prior to VMMC was predictive of early resumption of sexual activity. Unlike previous implementation evaluations, we did not find that being married or living with a partner was predictive of early sexual activity resumption. 20 Our results have implications for VMMC within real-world settings and highlight considerations for health policy-makers and planners as VMMC continues to roll out across African countries with high HIV burden. Our study also contributes to the limited data on programmatic VMMC outcomes outside of countries where the initial VMMC randomized trials and subsequent follow-on studies were conducted.
Scale-up of VMMC has been associated with decreasing HIV burden at the population level 30 and is a core component of the Joint United Nations Programme on HIV/AIDS (UNAIDS) strategy for ending HIV by 2030. 11 However, early resumption of sexual activity post-VMMC procedure could reduce the potential impact of VMMC on population HIV incidence.14,23,24 Similar to other post-RCT studies from Kenya, Zambia, and Tanzania,14,20–22 we found that nearly one-third of men who became circumcised resumed sex within six weeks of undergoing VMMC, of whom 28% had sex within three weeks of the procedure. These data suggest that existing pre-VMMC counseling to abstain from sex for six weeks post-procedure may not be effective for all men. Given the high frequency of early resumption of sexual activity in real-world settings, additional strategies are needed to support men in remaining abstinent through wound healing to maximize the public health benefits of VMMC.
In studies among Kenyan men who underwent VMMC within programmatic settings, risk factors for early resumption of sex included being married or living with a partner, older age, being employed, engaging in risky sexual behavior, and concerns about losing sexual partners.20,21,27 Similar to previous studies from other countries, we found that employed men and those who engaged in condomless sex with regular partners were more likely to resume sex early, including within three weeks following VMMC. These findings suggest that men who may have financial resources available to access sex and those who engage in riskier sex are more likely to resume sex early which may be particularly disadvantageous to VMMC programs as these characteristics are also associated with HIV risk among African men. 31 Unlike previous studies from Kenya,20,21,27 we did not find marriage to be associated with resuming sex early, though the frequency of marriage was appreciably lower in our study population (<10% versus ∼30%) which is representative of Batswana men overall. 32 In contrast to prior studies, we found that younger age was associated with resuming sex early and men aged 30–34 years were twice more likely to have sex early than older men. Our findings suggest that interventions targeting men at highest risk for resuming sex early in VMMC programs should be tailored to the local context.
One strategy to reduce complications associated with early resumption of sex is to focus efforts on performing VMMC prior to sexual debut. However, current VMMC strategies target sexually active men in several HIV high-burden settings, including Botswana. 6 Limited evidence exists on effective approaches for encouraging sexual abstinence during wound healing among adult men post-VMMC. 33 Only one prior study in Kenya tested an intervention to promote post-VMMC abstinence using a text message-based platform; no statistical difference in early resumption of sex was found between study arms. 21 In a prior qualitative study, we found a lack of awareness of the increased risk of HIV acquisition during the wound healing period among Batswana men. 34 In our current study, nearly half of men reported HIV prevention as the primary reason for undergoing VMMC. Future intervention studies aiming to promote post-VMMC abstinence should emphasis HIV prevention messaging during wound healing and incorporate qualitative findings about how norms and attitudes drive men’s health promoting HIV preventative behaviors.35,36
Our study has limitations. Recruitment was based on normal provision of VMMC services by the Botswana MOH; however, we only enrolled men at sites in Gaborone (an urban center), who may not be representative of Batswana men undergoing VMMC in more rural settings. Our study focused on surgical VMMC as this is the most common circumcision in Botswana. Wound healing with nonsurgical devices can be longer than six weeks and thus our results on early resumption of sexual activity may not be translatable to nonsurgical circumcision approaches. 37 Not all men returned for follow-up and/or had data on sexual activity available at six weeks post-VMMC. This may bias our estimate of the overall prevalence and predictors for early resumption of sex that we identified. We detected minimal baseline behavioral differences between men with and without six-week data available, though employment status differed by availability of six-week data and was predictive of early sex resumption. It is possible that men whose data were missing more or less likely to resume sex early which could bias our results. We were unable to conduct a time-to-event analysis as we assessed timing of resumption of sex only at six weeks post-VMMC. Future studies should consider ascertaining the number of days to having sex after the VMMC procedure and more intensive follow-up tracing procedures including home visits to ascertain more complete data.
To date, VMMC programs have primarily focused on implementation and increasing the number of men undergoing VMMC. However, as reducing HIV transmission is paramount, there is a need to effectively promote abstinence among recently circumcised men to realize the UNAIDS goal of ending HIV by 2030.11,33 Similar to prior studies in other settings, our data show that a significant proportion of men who undergo VMMC resume sex prior to six weeks. As VMMC continues to roll out, additional interventions are needed to encourage abstinence until complete wound healing to maximize the benefits of VMMC.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the President’s Emergency Plan for AIDS Relief (PEPFAR), through grant number U91HA06801 from the U.S. Department of Health and Human Services, Health Resources and Services Administration (HRSA), HIV/AIDS Bureau’s Global Health Systems Branch.