
Abstract
Adolescent men who have sex with men (MSM) are at increased risk for sexually transmitted infections (STIs) and HIV; however, data documenting STI screening, STI burden, and associated risk factors for STIs are extremely limited. Using 2015 data from the National HIV Behavioral Surveillance among Young MSM, we examined self-reported STI screening and STI diagnosis of chlamydia, gonorrhea, or syphilis among sexually active adolescent MSM by selected characteristics. Analysis of STI diagnosis was limited to participants who reported an STI screening. Differences in STI screening and STI diagnosis and factors associated with screening and diagnosis were examined using bivariate and multivariable binomial regression models. Less than half of adolescent MSM reported having ever been screened for an STI. Among these, more than a quarter reported having ever been diagnosed with chlamydia, gonorrhea, or syphilis. STI screening was associated with visiting a healthcare provider in the past 12 months and having ever been tested for HIV. Having ever had an STI diagnosis was associated with the participant age of 18 years and having sex before 13 years old. Among adolescent MSM, STI screening was suboptimal and STI burden was significant. STI intervention and prevention programs are urgently needed to promote STI awareness, timely screening, and early diagnosis to interrupt transmission among this vulnerable population.
Keywords
Introduction
In the United States, reported cases of sexually transmitted infections (STIs) are on the rise. From 2015 to 2016, the numbers of reported infections increased 4.7% for chlamydia, 18.5% for gonorrhea, and 17.6% for syphilis. 1 In 2016, a record high of more than two million cases of three nationally reported STIs – chlamydia, gonorrhea, and syphilis – were reported and it is estimated that nearly 20 million new STIs occur every year, half of which occur among adolescents and young adults aged 15–24 years. 2 Gay, bisexual, and other men who have sex with men (collectively referred to as MSM) are at increased risk of many STIs, including primary and secondary syphilis and gonorrhea. In 2016, MSM accounted for 81% of male cases where the gender of the sex partner is known and over half of primary and secondary syphilis cases overall. 3 From 2010 to 2015, the estimated number of gonorrhea cases increased 151% among MSM, while it increased less than 40% among other populations. 2
Adolescent (aged 13–18 years) MSM are an emerging high-risk population. Research indicates that adolescent MSM are more likely to engage in risky sexual behaviors compared to their heterosexual counterparts.4,5 The 2017 National Youth Risk Behavior Survey found that adolescent MSM were more likely than those who had sexual contact with only females to have sexual intercourse before age 13 years and inject illegal drugs and less likely to have used a condom at last sex. 5 These behaviors are paired with the reality that adolescents as a whole are less likely to access and use quality prevention and clinical services.2,6 The combination of behavioral risk and sociocultural and structural factors makes adolescent MSM particularly vulnerable to STIs and HIV.7,8 Given the increased burden of STIs among MSM in the U.S., the Centers for Disease Control and Prevention (CDC) recommends annual STI testing for sexually active MSM, including adolescent MSM. 9 However, the data documenting the STI screening, STI burden, and associated risk factors of STIs among adolescent MSM are extremely limited. There is a need to understand and address the STI epidemic among adolescent MSM.
The objective of this analysis is to assess self-reported STI screening and diagnosis among sexually active adolescent MSM. We examined reported STI screening and diagnosis by selected characteristics to determine factors that are potentially associated with these two outcomes. Prevalence of self-reported STI diagnosis may serve as an estimate of the STI burden among adolescent MSM. Results of this analysis are critical to understand the STI epidemic among adolescent MSM and can provide guidance on prevention and intervention strategies among this particularly vulnerable population in the U.S.
Methods
In 2015, CDC conducted an HIV behavioral surveillance project, National HIV Behavioral Surveillance among Young Men Who Have Sex with Men (NHBS-YMSM), in three cities: Chicago, New York City, and Philadelphia. Young men eligible for participation in the study were (1) aged 13–18 years; (2) male at birth; (3) current residents of the participating metropolitan statistical areas; (4) able to complete the survey in English or Spanish; and (5) reported ever having sex with another male, self-identified as gay or bisexual, or indicated same-sex attraction. Details on sampling and recruitment methods have been published previously. 4
Participation in NHBS-YMSM was anonymous. A waiver of documentation of informed consent was requested and received for all three study sites. In addition, a waiver of parental permission for participants <18 years of age was requested and received in New York City (approved for 13–17 years of age), Philadelphia (approved for 14–17 years of age), and Chicago (approved for 16 and 17 years of age). All NHBS-YMSM activities, including the age categories in the waiver of parental permission, were determined by local institutional review boards and approved by CDC. NHBS-YMSM consenting participants underwent an in-person eligibility screener and if eligible, completed a behavioral assessment with a trained interviewer. Anonymous HIV testing was offered to all participants regardless of self-reported HIV infection status. Individuals were compensated for their participation in project activities, receiving approximately $25 for the behavioral survey and $25 for HIV testing.
Participants were included in this analysis if they had a complete, valid survey and reported ever having anal sex with male partners. During the interview, each participant was asked questions on whether during the past 12 months he had been tested by a doctor or other healthcare provider for an STI and if he had been told by a doctor or other healthcare provider that he had gonorrhea, chlamydia, or syphilis. Participants who reported having had an STI test were defined as having been screened. Participants were considered to have received an STI diagnosis if they reported being told by a doctor or other healthcare provider that they had the infection.
We described sociodemographic characteristics of adolescent MSM and those with an STI screening and with a diagnosis of chlamydia, gonorrhea, or syphilis, and at least one of the three STIs. To examine differences in and assess factors associated with STI screening and diagnosis by selected characteristics, we used bivariate and multivariable binomial regression models (PROC GENMOD in SAS v9.4). The initial multivariable model included all characteristics that were significant at 0.05 level in the bivariate models and the final multivariable model included factors that remained significant at 0.05 level. Analysis of STI diagnosis was limited to participants who reported STI screening. Further, because there was zero syphilis and gonorrhea diagnosis and only one chlamydia diagnosis in the 13–15 year-olds, we combined the age groups of 13–15 and 16–17 years into 13–17 years for the analysis of STI diagnosis.
Results
A total of 428 participants were included in the analysis (Table 1). Among them, 42.3% were recruited from Chicago, 37.9% from New York City, and 19.9% from Philadelphia; 9.3% were aged 13–15 years, 58.9% aged 16–17 years, and 31.8% aged 18 years; 42.9% identified as black, 37.9% as Hispanic/Latino, 15% as white, and 4.2% reported other or multiple race groups. The majority of the participants identified as homosexual (67.8%) or bisexual (31%). Almost half (45.3%) grew up in a two-parent household and (45.6%) had parents with a college degree or above. Of the sample, 27% reported household financial instability during the past 12 months, 29.9% had ever been kicked out of the house or run away, and 27.9% reported binge drinking during the past 30 days. Over half (60.3%) had ever tested for HIV. Almost all reported having health insurance (94.1%) and visiting a healthcare provider in the past 12 months (89.5%). Less than 1% ever injected drugs, 27.8% had sex before 13 years old, and 39.7% had four or more sex partners.
Selected demographic characteristics of adolescent men who have sex with men – National HIV Behavioral Surveillance among Young Men Who Have Sex with Men, three cities, 2015 (n = 428).
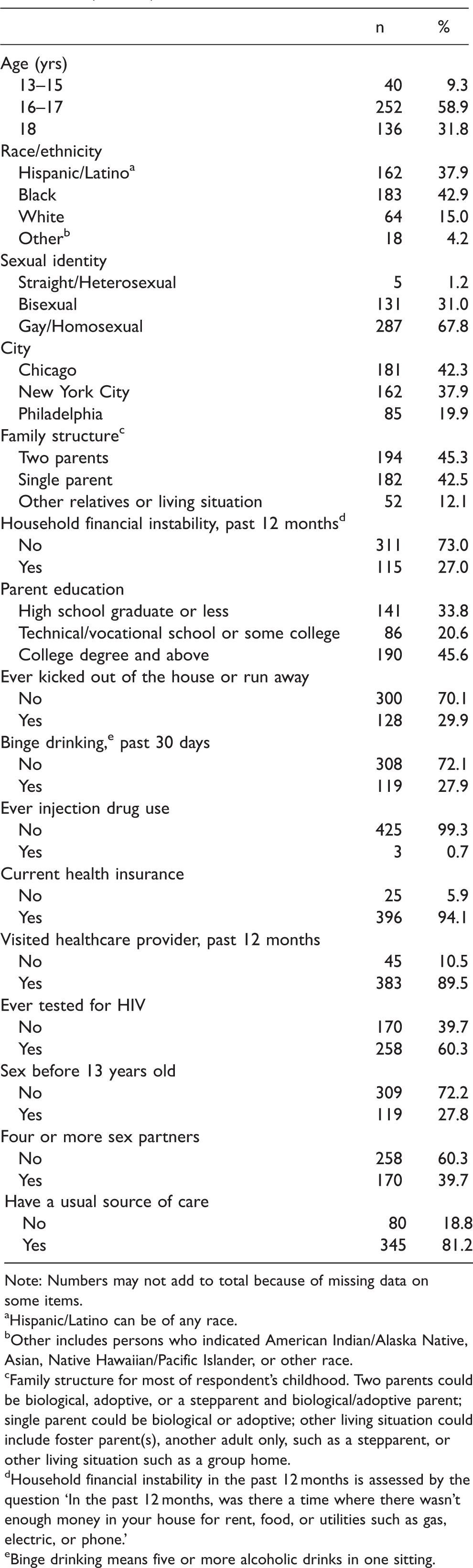
Note: Numbers may not add to total because of missing data on some items.
Hispanic/Latino can be of any race.
Other includes persons who indicated American Indian/Alaska Native, Asian, Native Hawaiian/Pacific Islander, or other race.
Family structure for most of respondent’s childhood. Two parents could be biological, adoptive, or a stepparent and biological/adoptive parent; single parent could be biological or adoptive; other living situation could include foster parent(s), another adult only, such as a stepparent, or other living situation such as a group home.
Household financial instability in the past 12 months is assessed by the question ‘In the past 12 months, was there a time where there wasn’t enough money in your house for rent, food, or utilities such as gas, electric, or phone.’
Binge drinking means five or more alcoholic drinks in one sitting.
There were 191 (44.6%) participants who reported an STI screening in the past 12 months (Table 2). STI screening was more common among participants aged 18 years versus 13–15 years (51.5% versus 22.5%, p = 0.0057), those who identified as black (50.8%, p = 0.0074) and Hispanic/Latino (46.3%, p = 0.0016) compared to white (25%), were recruited from Philadelphia versus Chicago (55.3% versus 37.6%, p = 0.0053), experienced household instability in the past 12 months (53.9% versus 41.2%, p = 0.0127), reported having ever been kicked out of the house or run away (57.8% versus 39%, p = 0.0002), visited a healthcare provider during the past 12 months (47.8% versus 17.8%, p = 0.0022), reported ever testing for HIV (63.6% versus 15.9%, p < 0.0001), had sex before 13 years old (57.1% versus 39.8%, p = 0.0009), and had four or more sex partners (56.5% versus 36.8%, p < 0.0001). The multivariable analysis showed that adolescent MSM who visited a healthcare provider in the past 12 months (aPR = 2.4, 95% CI: 1.3–4.4) and those who reported ever testing for HIV (aPR = 3.9, 95% CI: 2.7–5.5) were more likely to report an STI screening than those who did not. No other significant associations were identified in multivariable analysis.
STI screening among adolescent men who have sex with men – National HIV Behavioral Surveillance among Young Men Who Have Sex with Men, three cities, 2015.

aPR: adjusted prevalence ratio; STI: sexually transmitted infection.
Note: Numbers may not add to total because of missing data on some items.
Bivariate and multivariable analysis are through binomial regression models.
Hispanic/Latino can be of any race.
Other includes persons who indicated American Indian/Alaska Native, Asian, Native Hawaiian/Pacific Islander, or other race.
Family structure for most of respondent’s childhood. Two parents could be biological, adoptive, or a stepparent and biological/adoptive parent; single parent could be biological or adoptive; other living situation could include foster parent(s), another adult only, such as a stepparent, or other living situation such as a group home.
Household financial instability in the past 12 months is assessed by the question ‘In the past 12 months, was there a time where there wasn’t enough money in your house for rent, food, or utilities such as gas, electric, or phone.’
Binge drinking means five or more alcoholic drinks in one sitting.
Among 191 participants reporting STI screening in the past 12 months, 27 (14.1%) reported a chlamydia diagnosis, 30 (15.7%) reported a gonorrhea diagnosis, 15 (7.9%) reported a diagnosis of syphilis, and 49 (25.7%) reported a diagnosis of at least one of the three STIs (Table 3). A higher percentage of a chlamydia diagnosis was reported among participants identifying as black than Hispanic/Latino (20.4% versus 8%, p = 0.0338), participants recruited from Philadelphia versus New York City (29.8% versus 5.3%, p = 0.0012), who grew up in a two-parent household compared to single-parent household (19.6% versus 8%, p = 0.0445), those who had ever been tested for HIV (16.5% versus 0%, p = 0.0028), who reported having sex before 13 years old (27.9% versus 6.5%, p = 0.0002), and who had four or more sex partners (20.8% versus 7.4%, p = 0.0122). A higher prevalence of gonorrhea diagnosis was reported among participants recruited from Philadelphia (21.3%, p = 0.0227) and Chicago (22.1%, p = 0.0133) versus New York City (6.6%), those who reported ever being kicked out of the house or run away (25.7% versus 9.4%, p = 0.0039), and who reported having sex before 13 years old (25% versus 10.6%, p = 0.0104). None of the factors was associated with reported syphilis diagnosis, potentially because of the small number in syphilis diagnosis. For a diagnosis of at least one of the three STIs, a higher prevalence was reported among 18 year-olds than younger participants (35.7% versus 19.8%, p = 0.0156), and those identifying as black as compared to Hispanic/Latino (35.5% versus 16%, p = 0.0078), recruited from Philadelphia (36.2%, p = 0.0041) and Chicago (32.4%, p = 0.0087) versus New York City (13.2%), who grew up in a two-parent household as compared to a single-parent household (34.8% versus 16%, p = 0.0098), whose parent’s education level was high school graduate or less compared to college degree and above (31.4% versus 15.6%, p = 0.0277), who reported having ever been kicked out of the house or run away (33.8% versus 20.5%, p = 0.041), and who reported having sex before the age of 13 years (41.2% versus 17.1%, p = 0.0003). Adolescent MSM aged 18 years (aPR = 2.0, 95% CI: 1.3–3.1) and those who reported having sex before age 13 (aPR = 2.6, 95% CI: 1.6–4.1) were more likely to report a diagnosis of at least one of the three STIs than other adolescent MSM. No other significant associations were identified in multivariable analysis.
Chlamydia, gonorrhea, and syphilis diagnoses among adolescent men who have sex with men who received STI screening in the past 12 months – National HIV Behavioral Surveillance among Young Men Who Have Sex with Men, three cities, 2015 (total n = 191).
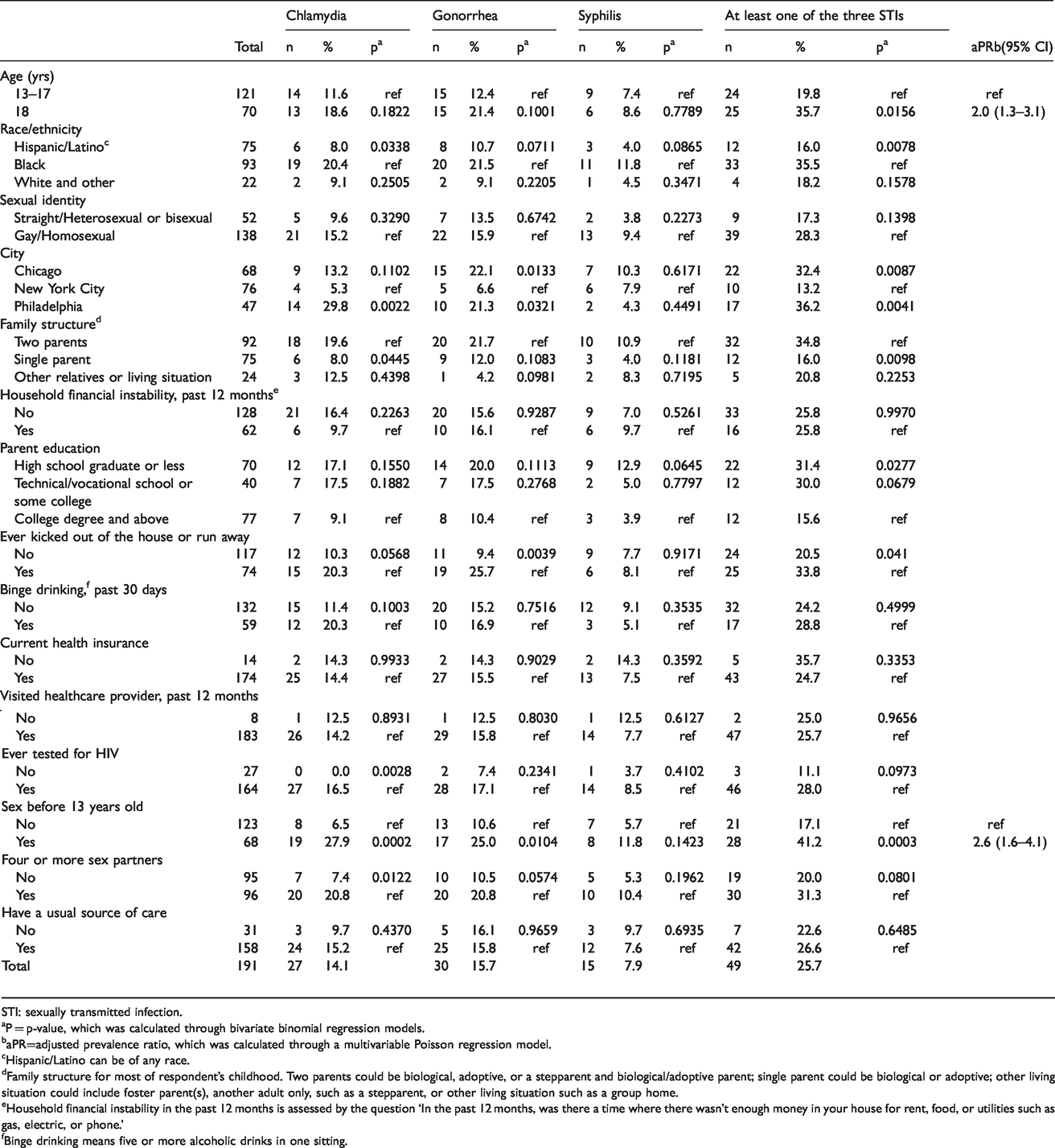
STI: sexually transmitted infection.
P = p-value, which was calculated through bivariate binomial regression models.
aPR=adjusted prevalence ratio, which was calculated through a multivariable Poisson regression model.
Hispanic/Latino can be of any race.
Family structure for most of respondent’s childhood. Two parents could be biological, adoptive, or a stepparent and biological/adoptive parent; single parent could be biological or adoptive; other living situation could include foster parent(s), another adult only, such as a stepparent, or other living situation such as a group home.
Household financial instability in the past 12 months is assessed by the question ‘In the past 12 months, was there a time where there wasn’t enough money in your house for rent, food, or utilities such as gas, electric, or phone.’
Binge drinking means five or more alcoholic drinks in one sitting.
Discussion
We examined self-reported STI screening in the past 12 months and diagnosis among adolescent MSM in order to advance our understanding of STI testing and prevalence among this population in the U.S. We found that less than half of adolescent MSM reported ever being screened for STIs and among those who were screened, more than a quarter reported having had a diagnosis of at least one of the three STIs examined (i.e. chlamydia, gonorrhea, and syphilis). STI screening in the past 12 months was associated with visiting a healthcare provider in the past 12 months and having ever been tested for HIV. A diagnosis of chlamydia, gonorrhea, or syphilis in the past 12 months was independently associated with participant’s age and having sex before 13 years old.
CDC recommends at least annual screening for chlamydia, gonorrhea, and syphilis for sexually active MSM and more frequent screening (e.g. every 3–6 months) for MSM who have multiple or anonymous partners. 9 However, less than half of the adolescent MSM in this sample reported ever being screened for an STI. Therefore, it is likely that STI screening in the past 12 months is substantially lower. Results of a national survey of youth aged 15–25 years indicated that only 6.1% of males received an STI test in the past 12 months. 10 In comparison, 2014 data showed that 56% of MSM aged 25–29 years reported a syphilis screening in the past 12 months. 11 These results suggest that STI screening among adolescent MSM is suboptimal and programs are needed to increase STI screening among this population. Furthermore, many of the YMSM included in our analysis engage in risk behaviors that may increase their risks of both HIV and STIs (e.g. larger numbers of sex partners, binge drinking).
Many STIs have no associated symptoms. High prevalence of frequently asymptomatic STIs suggests the importance of proactive screening by healthcare providers. In our analysis, 90% of participants visited a healthcare provider in the past 12 months, but only 48% of them reported an STI screening. Engaging clinicians to implement proactive STI testing might be an effective way to increase STI screening among adolescent MSM. Because STI screening recommendations are based on behavior and not sexual orientation or identity and certain STI tests can be specific to anatomic sites, it is critical for clinicians to take a sexual history to help ensure that those at greatest risk are being appropriately screened and tested. Increasing comfort and skill of sexual history taking among clinical providers that see adolescent MSM patients may have a positive impact on screening for STIs and subsequent treatment for identified infections.
Among adolescent MSM who reported STI screening, more than one in four participants reported ever been infected with chlamydia, gonorrhea, or syphilis. Infection with an STI can facilitate the subsequent transmission or acquisition of HIV.12–14 Therefore, effective prevention programs are needed to increase early diagnosis and interruption of disease transmission among adolescent MSM. As these are school-aged adolescents, programs like school-wide youth sexual health education programs, programs that work with gay alliance clubs to raise HIV and STI awareness, and school-based HIV and STI testing events could be considered for STI prevention among adolescent MSM.
Our multivariable analysis indicates that adolescent males who had sex before 13 years old were more likely to report a diagnosis of at least one of the three STIs in the past 12 months than those who did not. This result supports other findings that YMSM are at an increased risk for STIs due to risk behaviors. 6 Studies show that supportive friendships and parental connectedness decrease the likelihood of sexual risk behavior among adolescents and family connectedness significantly decreases the odds of acquiring HIV.15,16 Therefore, it is important to engage parents and educate them on how to provide a supportive environment and use family-based interventions to help reduce risky sexual behaviors among adolescent MSM.
This analysis has the following limitations. First, the NHBS-YMSM study is a convenience sample recruited from three cities. Participants may not be representative of all sexually active adolescent MSM aged 13–18 years in the U.S. Second, data on STI screening and diagnosis and selected characteristics were self-reported and may be subject to reporting bias. Previous studies have found over-reporting for STI screening and under-reporting for STI diagnosis.17,18 We are unable to assess the scope of the reporting bias. Third, because one of the original objectives of the NHBS-YMSM was to determine the most effective and feasible sampling methods to reach adolescent MSM, participants were recruited through different sampling methods: venue-based sampling in New York City only, respondent-driven sampling in all three participating cities, and Facebook sampling in Philadelphia and Chicago. Data are not weighted to account for the complex sampling methodologies required to locate, recruit, and interview participants.
In summary, among sexually active adolescent MSM, STI screening was suboptimal and STI burden is significant. STI intervention and prevention programs are urgently needed to promote STI awareness, timely screening, and early diagnosis to interrupt transmission among this vulnerable population.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The findings and conclusions in this paper are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by funding of NHBS by the CDC (PS11-001).