
Abstract
Clinical correlates and CD4 cell count are used to predict HIV virological failure among children living with HIV in resource-limited settings, but there are limited data on their prediction of treatment failure compared to viral measurement. Using HIV viral load as a gold standard, sensitivity and specificity of longitudinal CD4 responses and clinical changes were defined in children living with HIV on antiretroviral therapy (ART) for ≥6 months in Kenya. Prevalence and correlates of virological failure were determined using log-binomial regression with robust standard error. Among 223 children who were followed for 12 months, median age in years at HIV diagnosis, ART initiation, and study enrollment were 3.3, 3.6, and 7.5, respectively. Older children at HIV diagnosis and ART initiation were less likely to experience virological failure. Immunological and clinical failure had low sensitivity (0 and 2%, respectively) to identify virological failure. Among those with virological failure, there was no indication from immunological markers and only two (2%) indicated with clinical markers. Clinical and immunological monitoring of HIV were insensitive and poor predictors of virological failure, emphasizing the importance of routine virological monitoring to inform ART treatment decisions for children living with HIV.
Keywords
Introduction
An estimated 1.8 million children worldwide were living with HIV at the end of 2017, more than 70% of whom live in sub-Saharan Africa. 1 Among these, an estimated half a million children living with HIV are on antiretroviral therapy (ART), a number that will increase as scale-up and access to treatment programs improve.
The World Health Organization (WHO) continuously updates their guidelines on diagnosing treatment failure in children living with HIV. In 2013, the WHO published updated Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection. 2 HIV viral load (VL) testing was recommended, when available, to monitor the response to ART and diagnose treatment failure in both children and adults, and the threshold for virological failure was lowered to 1000 HIV RNA copies/ml from the 2010 Guideline threshold of 5000 copies/ml. 3 CD4 cell count and clinical monitoring were recommended when VL testing is not routinely available, as is common in many low resource areas. This recommendation was carried over to the 2016 WHO Consolidated Guideline. 4
A 2014 review of immunological and clinical sensitivity and specificity to detect treatment failure identified 14 published manuscripts in adults that assessed the WHO 2010 Guidelines and demonstrated low sensitivity and predictive value to detect high HIV virus levels in adult populations.5–10 However, the value of clinical correlates and CD4 levels to predict HIV virological failure is less well defined for children living with HIV under 15 years of age.5,11,12 The review includes only three pediatric manuscripts that compared immunological and clinical monitoring to VL testing, and all of them used a VL threshold of 5000 copies/ml to define treatment failure.13–15 This is a higher threshold than the 1000 copies/ml that the WHO used in their 2013 and 2016 guidelines to define virological failure.2,4
The study presented here assessed the sensitivity and specificity of immunological and clinical failure measurements to predict virological failure, and determined the prevalence and correlates of virological failure in a cohort of children living with HIV in Nairobi, Kenya.
Methods
Study design and procedures
This is a nested retrospective cohort study. The parent study took place at Kenyatta National Hospital from 2011 to 2014 and followed children living with HIV who were taking combination ART, over a two-year period to evaluate levels of immunity against measles and response to measles revaccination.16,17 Child eligibility criteria for the parent and nested study included HIV-1 infection confirmed by ELISA and/or PCR, treatment with ART for a minimum of 6 months, age between ≥15 months and 12 years, and a CD4% ≥15. The Kenyatta National Hospital Ethics and Research Committee and University of Washington Institutional Review Board approved the study.
Laboratory assays
Blood draws for CD4%, CD4 cell count, and HIV VL were obtained at enrollment and 12 months after enrollment. CD4% was determined in real time by the University of Nairobi Paediatrics Laboratory using internal quality controls (FACSCalibur, BD Biosciences, USA). To determine HIV VL, plasma samples were frozen and shipped to Seattle, USA on dry ice and stored at −80°C until use. HIV-1 RNA levels were measured in bulk at the end of the study using a prototype HIV-1 VL assay (Gen-Probe/Hologic, San Diego, CA), which has been validated on the HIV subtypes prevalent in Kenya. 18
Definition of clinical, immunological, and virological failure
In this analysis, we defined treatment failure after at least six months of ART in close accordance with 2016 WHO guidelines, 4 including (1) clinical failure as defined by a new or recurrent clinical event that indicates advanced immunodeficiency (WHO clinical stage 3 and 4 clinical condition, with the exception of tuberculosis); (2) immunological failure in children younger than five years as defined by a persistent CD4 level below 200 cells/mm3, or for children older than five years, persistent CD4 levels below 100 cells/mm3; or (3) virological failure defined as a plasma VL above 1000 copies/ml based on two consecutive VL measurements at least three months apart. Our analysis differs slightly from 2016 WHO Guidelines in two ways. First, our analysis includes children over the age of ten, a group that the WHO Guidelines consider adolescents. Clinical failure criteria in adolescents are defined by a new or recurrent clinical WHO stage 4 only event, and immunological and virological failure criteria are the same. Second, the 2016 WHO Guidelines state that any virological failure is defined after two consecutive measurements in three months, which was not feasible in our retrospective cohort design.
Statistical analyses
Data from study questionnaires and laboratory tests were entered into a Microsoft Access Database then checked, cleaned, and analyzed using Stata (Stata Statistical Software: 14. College Station, TX). Clinical and immunological failure was compared to virological failure to calculate sensitivity, specificity, and predictive values. Univariate correlates of virological failure were determined using log-binomial regression with robust standard error. 19 The correlates of virological failure assessed were child’s gender, clinical stage at HIV diagnosis, age at HIV diagnosis, exposure to single-dose nevirapine, age at enrollment, and time on ART at enrollment. The caregiver correlates of child virological failure assessed were biological relationship to child, and death of either or both parents.
Results
In total, 223 (95%) of 235 children in the parent study 17 had plasma HIV RNA measurements both at study enrollment and 12 months’ follow-up, and were included in this nested study. Just under half were female (n = 107, 47%). At enrollment, 44 (20%) were under five years of age, 134 (60%) were five to under ten years, and 45 (20%) were ten years and older. Child age ranged from 1.5 to 11.9 years and the median age was 7.5 years (interquartile range [IQR] 5.5–9.5). Median age in years at the time of HIV diagnosis was 3.3 (IQR 1.6–4.8), median time between HIV diagnosis and ART initiation was one month (IQR 0.5–5), and median age at ART initiation was 3.6 years (IQR 1.8–5.3).
At enrollment, 11 (5%) had a new or recurring clinical event indicating advanced or severe immunodeficiency (WHO clinical stage 3 or 4) that occurred within six months of the study visit and met the criteria for clinical failure. The median CD4 cell count in the overall cohort was 1017 cells/mm3 (IQR 782–1372); no children under the age of five had CD4 < 200 cells/mm3, the threshold for failure in this age group. No children over the age of five had CD4 < 100 cells/mm3, the threshold for failure in this older group; and 51 (23%) had plasma HIV RNA >1000 copies/ml (Table 1). Two measurements were needed to determine immunological and virological failure, thus we were unable to characterize these types of failure at enrollment.
Descriptive characteristics for 223 children living with HIV on antiretroviral therapy (ART) in Nairobi, Kenya at the time of HIV diagnosis, time of ART initiation, time of study enrollment, and after 12 months of study follow-up.
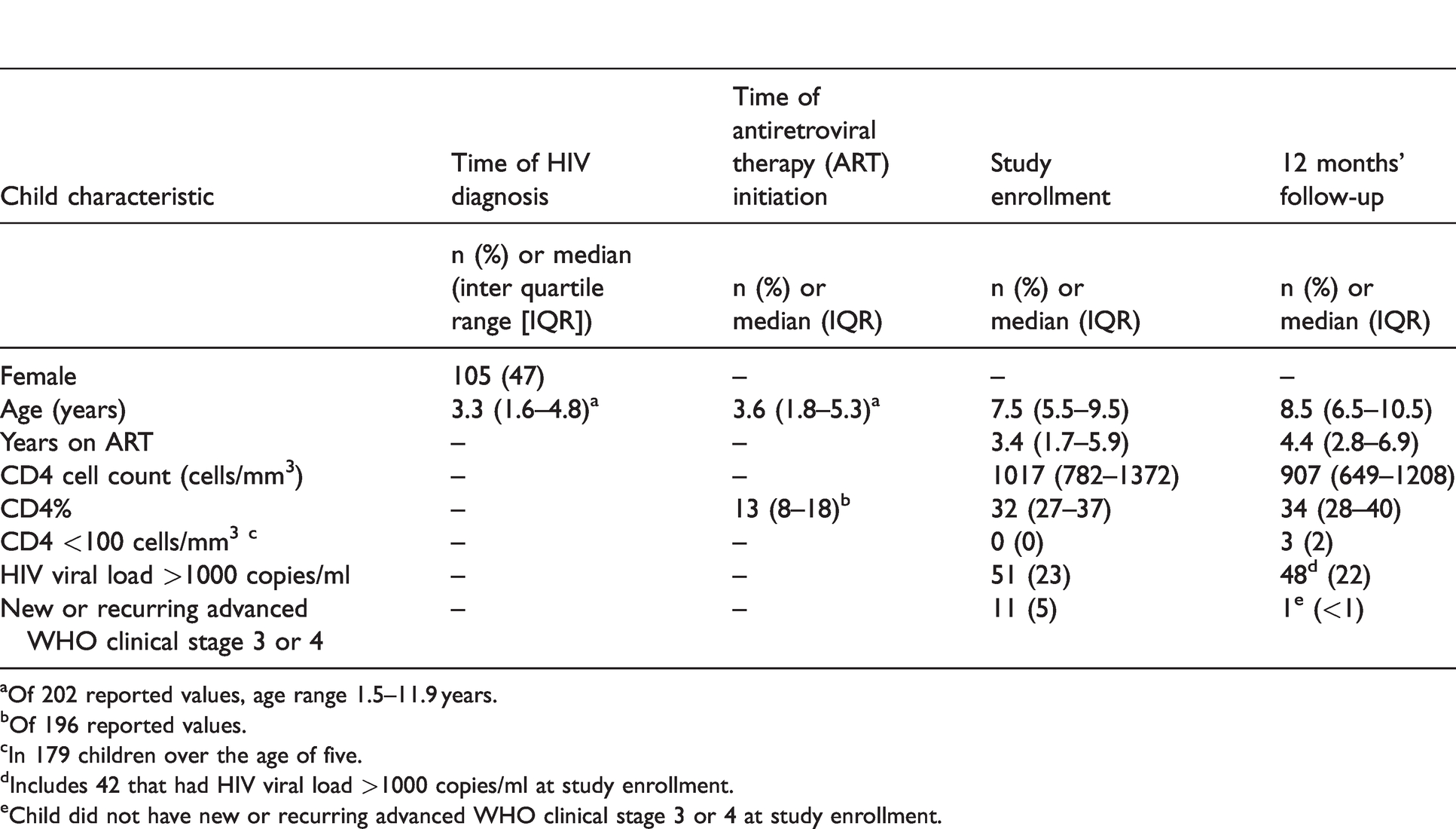
aOf 202 reported values, age range 1.5–11.9 years.
bOf 196 reported values.
cIn 179 children over the age of five.
dIncludes 42 that had HIV viral load >1000 copies/ml at study enrollment.
eChild did not have new or recurring advanced WHO clinical stage 3 or 4 at study enrollment.
The majority of children had primary caregivers who were biologically related to them (n = 216, 97%) and 74% had their mother as primary caregivers. Additionally, 60% of primary caregivers had at least a secondary school education, 17% of participants’ mothers were deceased, 12% had deceased fathers, 9% did not know whether their fathers were alive, 3% were orphans, and 6% had deceased mothers with unknown fathers.
At one year of follow-up, one child (<1%) was classified as having advanced WHO clinical stage 3 or 4; median CD4 cell count was 907 cells/mm3 (IQR 649–1208); no children under the age of five had CD4 < 200 cells/mm3; three (2%) children over the age of five had CD4 < 100 cells/mm3; and 48 (22%) had HIV plasma RNA >1000 copies/ml, 42 (19%) of whom also had HIV plasma RNA >1000 copies/ml at enrollment (Table 1).
Treatment failure
After one year of follow-up, 1 child (<1%) of 223 met criteria for clinical failure since enrollment. He advanced from WHO clinical stage 2 at enrollment to stage 3 after approximately four months due to severe pneumonia requiring multiple hospital visits. This same child had a CD4 of 968 cells/mm3 at enrollment and 753 cells/mm3 at 12 months, and a HIV VL of 4023 copies/ml at enrollment and 36,796 copies/ml at 12 months.
No children showed evidence of immunological failure over the study period. Specifically, none of the 44 children under the age of five had CD4 levels below 200 cells/mm3 or ≤10% at either enrollment or 12 months after enrollment. None of the 179 children over the age of five had CD4 levels below 100 cells/mm3 at enrollment, although three (2%) had CD4 levels below 100 cells/mm3 at 12 months. Of these three children, one had an undetectable level of HIV VL and two had HIV VL results over 1000 copies/ml at 12 months.
However, 42 of 223 (19%) children met criteria for virological failure at one year of follow-up. Of the 44 children under the age of five, 10 (23%) had persistent HIV VL levels over 1000 copies/ml at both enrollment and 12 months. Of the 179 children over the age of five, 32 (18%) had persistent HIV VL over 1000 copies/ml at both enrollment and at 12 months. Two children who met criteria for virological failure at one year also met criteria for clinical failure at study enrollment.
Sensitivity, specificity, and predictive value of clinical and immunological failure
While 42 (19%) children met virological failure criteria, no children met immunological failure criteria, and only one child met clinical failure criteria. The sensitivity of immunological failure to diagnose virological failure was 0%, with a specificity of 100%, and negative predictive value (NPV) of 81%. One child met WHO stage clinical failure and virological failure criteria, while 41 children with virological failure did not demonstrate clinical failure. The sensitivity of clinical failure for virological failure was 2%, specificity was 100%, positive predictive value (PPV) 100%, and NPV of 82% (Table 2).
Sensitivity, specificity, positive predictive value, and negative predictive value of immunological and clinical failure compared to virological failurea,b in children living with HIV on antiretroviral therapy in Nairobi, Kenya.
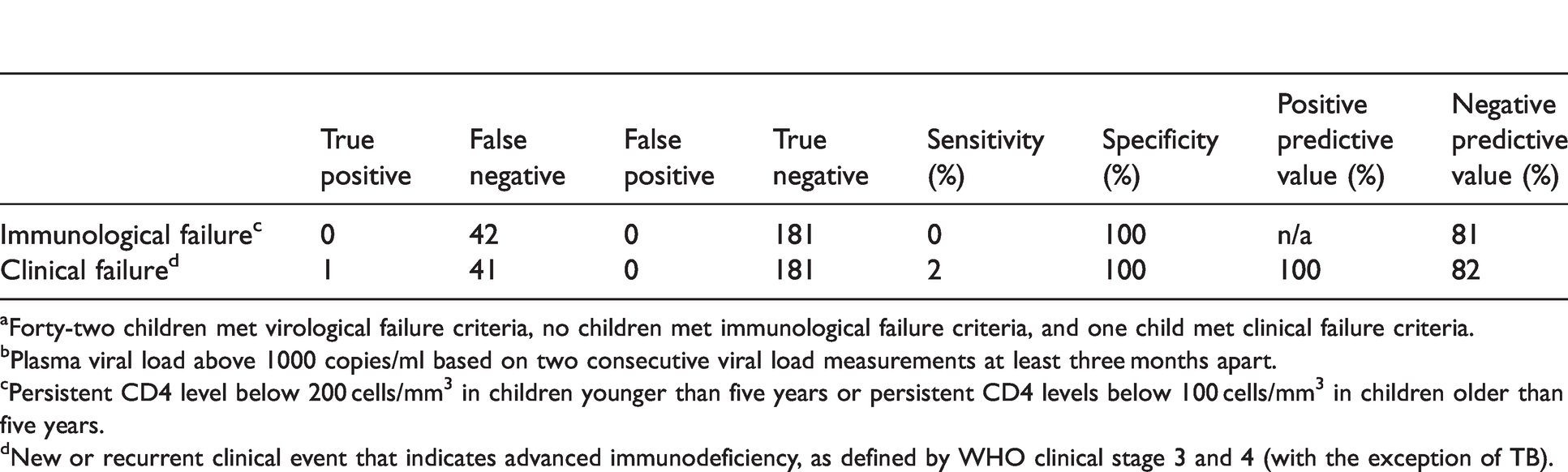
aForty-two children met virological failure criteria, no children met immunological failure criteria, and one child met clinical failure criteria.
bPlasma viral load above 1000 copies/ml based on two consecutive viral load measurements at least three months apart.
cPersistent CD4 level below 200 cells/mm3 in children younger than five years or persistent CD4 levels below 100 cells/mm3 in children older than five years.
dNew or recurrent clinical event that indicates advanced immunodeficiency, as defined by WHO clinical stage 3 and 4 (with the exception of TB).
Correlates of virological failure
Of the 206 children with available data on age at HIV diagnosis, 39 (19%) experienced virological failure during the study. For every one year increase in age at the time of HIV diagnosis, children were 16% less likely to experience virological failure during the study (relative risk [RR]=0.84, 95% confidence interval [CI] 0.74–0.96, p = 0.010). Similarly, of the 204 children with available data on age at HIV initiation, 38 (19%) experienced virological failure during the study. For every one year increase in age at the time of ART initiation, children were 12% less likely to experience virological failure during the study (RR = 0.88, 95% CI 0.77–0.99, p = 0.035). There were no statistically significant associations between HIV virological failure and gender, WHO clinical stage at HIV diagnosis, exposure to single-dose nevirapine, age at enrollment, or time on ART at enrollment. Nor were there statistically significant associations between HIV virological failure and caregiver biological relationship to child, or death of either or both parents (Table 3).
Correlates of virological failure in children living with HIV on antiretroviral therapy in Nairobi, Kenya.
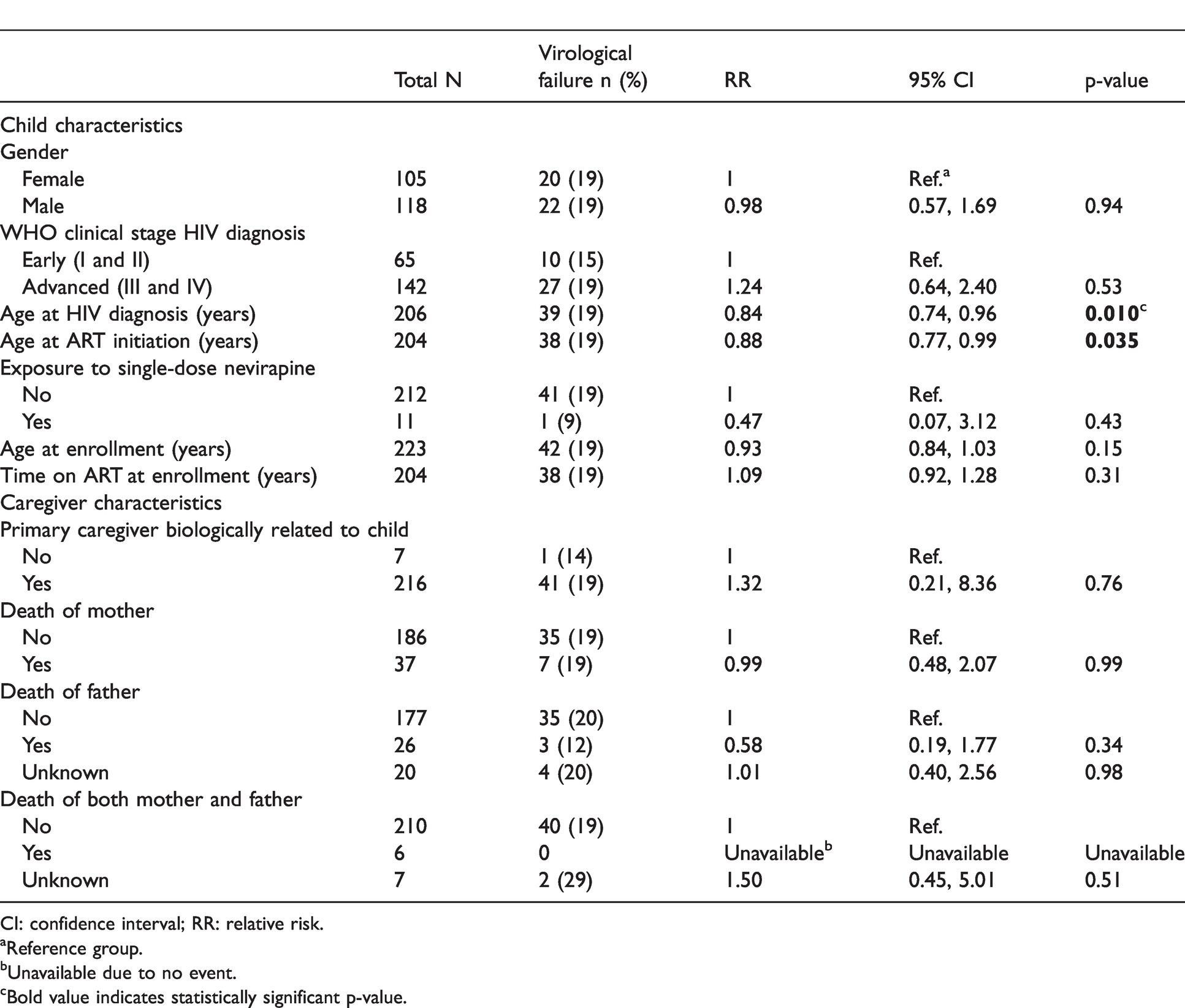
CI: confidence interval; RR: relative risk.
aReference group.
bUnavailable due to no event.
cBold value indicates statistically significant p-value.
Discussion
In this longitudinal study of Kenyan children living with HIV, nearly 20% met virological failure criteria though the majority (98%) did not meet any immunological and clinical criteria. Furthermore, measurement of immunological and clinical failure had low sensitivity to identify virological failure. Finally, children who were older at the time of HIV diagnosis and ART initiation were less likely to experience virological failure during the study.
Our finding that immunological criteria had low sensitivity to predict virological failure in children living with HIV on ART is similar to previous studies. Three published studies have compared immunological criteria to virological failure in children living with HIV.13–15 Two manuscripts described one South African cohort of children living with HIV that were on ART for more than one year, and found that immunological criteria had a sensitivity of 6 and 7% compared to virological failure, as defined by an HIV VL of >400 copies/ml and >5000 copies/ml, respectively, measured six months apart.13,14 This is slightly higher than our finding of 0% sensitivity when virological failure was defined as multiple measurements of HIV VL >1000 copies/ml. Both previous studies had a larger sample size, more than 2000 study participants each, to capture events. A third published study from Cambodia found a sensitivity of immunological criteria to detect virological failure, as defined as HIV VL >5000 copies/ml over multiple measurements, of 5%. 15 Specificity was 99% or higher in all three previous studies, similar to ours. While we were unable to determine PPV of immunological criteria, all three published studies found PPV between 20 and 64%. This is of concern, since use of CD4 immunological criteria as a marker for virological failure may lead to unnecessary change in ART regimens in patients who are truly virologically suppressed. 20
In the absence of routine HIV VL testing, and with the knowledge that CD4 and changes in clinical criteria are poor predictors of virological failure, other correlates may be useful in identifying children at high risk of virological failure. We found that children who were older at the time of HIV diagnosis and ART initiation were less likely to experience virological failure during the study. Many children in our study were born in the early 2000s, before HIV testing of infants and children of HIV-infected mothers was scaled up in Kenya. Older children may be different from younger children because they were healthy enough to survive to an age where they could be tested and treated for HIV, compared to the younger children who became sick at a younger age. It is possible that older children were infected with a less fit virus or had a more robust immune response in infancy and were able to control HIV early on in life, and maintain that control after treatment with ART. 21 It is also possible that drug formulations and weight-based prescribing patterns that make treatment of younger children challenging are less problematic in older children.
The 2016 Guidelines on Use of Antiretroviral Drugs for Treating and Preventing HIV Infection in Kenya recommend HIV VL testing of all HIV-infected patients at 6 and 12 months after ART initiation, and annually thereafter if HIV VL <1000 copies/ml. 22 CD4 cell count determination is recommended only at initiation of ART and then if a patient develops treatment failure in order to assess risk of opportunistic infection. Scale-up of programs that meet the recommendation is varied across the country, 23 as there are many barriers to routine VL monitoring. These include technological and economic obstacles, such as high cost of testing, insufficient laboratory capacity to perform tests, and limited storage of samples. 20
This study benefits from longitudinal follow-up and collection of clinical failure criteria. However, we are limited by a smaller sample size, and we observed a smaller number of events than previous studies that assessed immunological failure criteria. Thus, we were unable to calculate PPV of immunological failure criteria to predict virological failure. This study assessed an older cohort of children who were born in the early 2000s and were nearing adolescence at the beginning of the study, thus results may not be generalizable to younger children or those diagnosed early in life. The clinical failure criteria that we applied to the older children over the age of ten were more conservative than the 2016 WHO Guidelines, though no children over the age of ten experienced clinical failure by either definition. We chose to include children over the age of ten since virological failure monitoring in early adolescence remains a key strategy in HIV prevention, and virological failure is common in this age range. 24
This study provides additional evidence to a growing body of research, and current WHO guidelines, which suggests that clinical and immunological monitoring of HIV disease in children is insensitive and a poor predictor of virological failure. It is one of a few studies assessing a pediatric population that compares immunological and clinical monitoring to virological failure, and the only one, to our knowledge, to utilize the 2016 WHO Guideline VL threshold of 1000 copies/ml to define virological failure. Scale-up and access to routine virological monitoring is challenging in resource-limited countries, but could improve classification of HIV progression and decisions about modifying ART treatment to improve the health of children living with HIV.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the Institute of Allergy and Infectious Disease of the National Institutes of Health (K24AI087399, K24 AI071113). LPN received support from the National Center for Advancing Translational Sciences of the National Institutes of Health (TL1TR000422) and the UW Thomas Francis Jr. Global Health Fellowship.