
Abstract
Erythema elevatum diutinum (EED) is a form of chronic leukocytoclastic vasculitis, which is known to occur in human immunodeficiency virus (HIV)-positive patients. Mostly, in the setting of HIV, it presents as plaques, nodules and occasionally as vesicles. We present a case of EED manifesting as annular plaques in an HIV-positive man, which was predominantly acral in distribution, involving the face also. After starting on dapsone, it disappeared completely in three days.
Introduction
Erythema elevatum diutinum (EED) is a chronic leukocytoclastic vasculitis which can occur at any age but peaks in the sixth decade. 1 EED has been associated with many infections, hematological disorders, connective tissue disorders and inflammatory disorders.1–3 This case demonstrates an unusual morphology of EED presenting as annular plaques.
Case report
A 26-year-old man who was diagnosed human immunodeficiency virus (HIV)-positive six years ago (on antiretroviral therapy [ART] at the time of presentation: zidovudine, lamivudine and nevirapine) presented with multiple annular plaques over bilateral extensors of upper and lower extremities, buttocks, lower abdomen and face for six months' duration. On examination, the individual plaques were firm, annular with beaded margins, of variable size, round-to-oval in shape (Figure 1(a)) with central hyper-pigmentation and hemorrhagic crusting in a few lesions. Clinical differentials of granuloma annulare and insect bite hypersensitivity were considered and he was treated with potent topical steroids with mild improvement, but continued to have new crops of plaques associated with mild burning sensation.

Baseline clinical photograph showing dusky erythematous annular plaques with central hyperpigmentation over the extremities (a), complete resolution after three days of starting dapsone (b).
Evaluation
Routine blood, urine and stool investigations were within normal limits. Peripheral blood CD4+ cell count was 522 cells/mm3. Histopathology from multiple lesions showed neutrophilic and eosinophilic infiltrate in the upper and mid dermis with fibrosis (Figure 2(a)) along with features of leukocytoclastic vasculitis (Figure 2(b)).
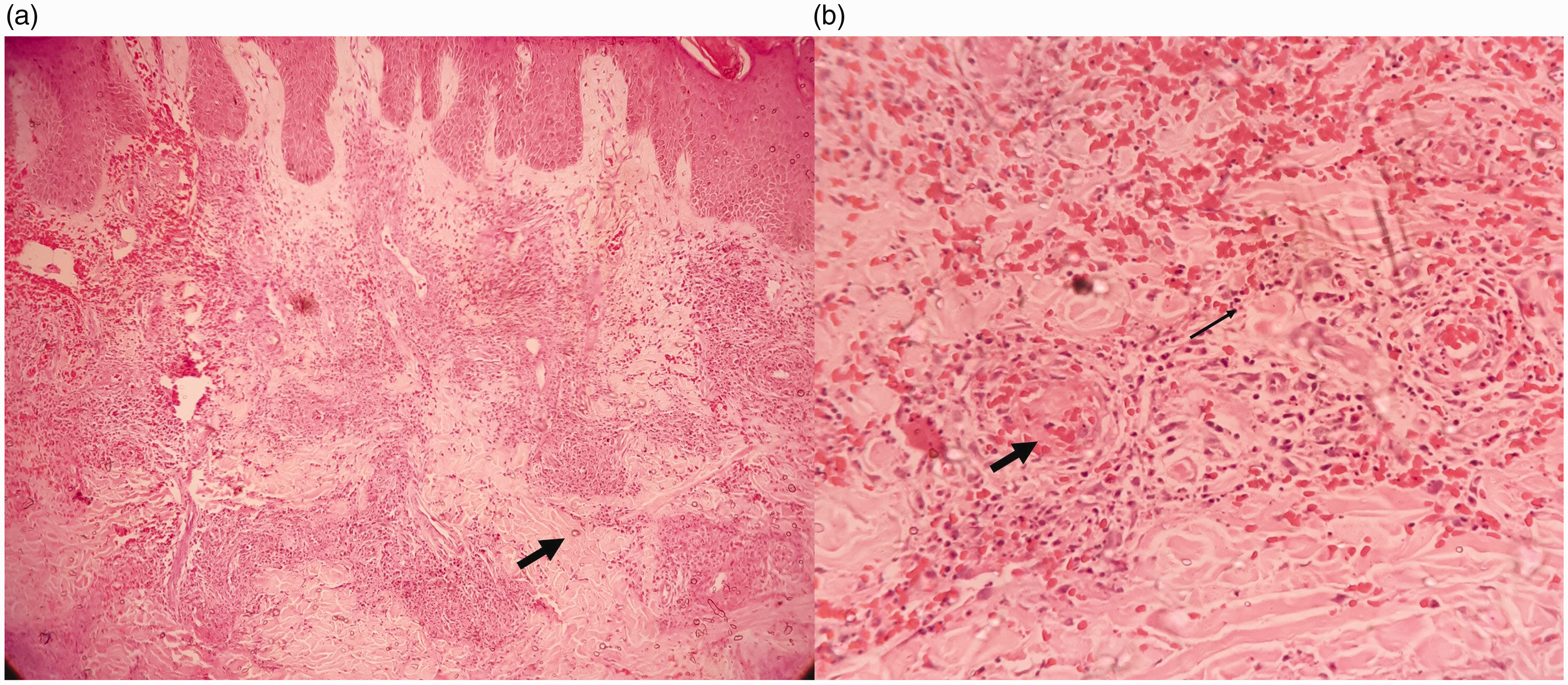
A 10× view showing dense upper and mid dermal, perivascular and interstitial infiltrate of neutrophils and few eosinophils along with vasculitis, mild fibrosis (thick arrow) and RBC extravasation (a), 40× view showing prominent fibrin deposition in vessel walls (thick arrow), along with prominent RBC extravasation and leukocytoclasia (thin arrow) (b).
In view of leukocytoclastic vasculitis along with fibrosis, a possible diagnosis of EED was suggested. Further investigations to look for paraproteinemia-like serum and urine electrophoresis were negative.
Treatment
He was started on dapsone 100 mg once daily. All the lesions subsided dramatically within three to four days and remained in remission at four months’ follow-up (Figure 2(b)). This dramatic response also favored the diagnosis of EED.
Discussion
EED is a rare form of chronic cutaneous small vessel vasculitis that usually manifests as papules, plaques and nodules over extensors of large and small joints.4,5 It is most commonly seen in the fourth to sixth decade, although it can present at any age. 2 The lesions are usually asymptomatic but can be associated with arthralgia. The differential diagnosis of EED includes granuloma annulare, bacillary angiomatosis, Kaposi’s sarcoma, etc. EED is currently thought to represent an arthus type reaction with immune complex deposition in vessels and subsequent inflammation. 6 It has been associated with a variety of underlying systemic disorders including autoimmune, inflammatory conditions and infections and hematological disorders, but HIV and immunoglobulin A (IgA) gammopathy are more commonly described.1–3 On histopathological examination, acute lesions of EED are characterized by leukocytoclastic vasculitis with little fibrin deposition. Chronic lesions demonstrate angiocentric eosinophilic fibrosis, capillary proliferation and infiltration of macrophages, plasma cells and lymphocytes with extracellular cholesterosis. EED is now recognized as one of the defined reactive dermatoses associated with HIV due to HIV antigen–antibody interaction. 6 However, in some cases, EED has been reported as the first clinical manifestation of HIV infection. 7 EED lesions in HIV infection have been described as nodular with palmar/plantar involvement with greater numbers of lesions occurring at an earlier age and poor responsiveness to dapsone.8,9 In addition, ART should be introduced in these cases, in association with dapsone. EED manifesting as annular plaques also has been reported in association with IgA gammopathy and post-streptococcal infection.10,11 To the best of our knowledge, this is the first case report of EED presenting as annular plaques in association with HIV.
Conclusion
EED can be a cutaneous manifestation of HIV and can present with unusual morphology like annular plaques. High index of suspicion and histopathological clues can help to reach the diagnosis. Therapeutic response to dapsone can be considered as an additional supporting feature.
Supplemental Material
STD874985 Supplemetal Material - Supplemental material for Unusual presentation of erythema elevatum diutinum in an HIV-positive man with dramatic response to dapsone
Supplemental material, STD874985 Supplemetal Material for Unusual presentation of erythema elevatum diutinum in an HIV-positive man with dramatic response to dapsone by Maninder Kaur, Alok K Sahoo and Somesh Gupta in International Journal of STD & AIDS
Footnotes
Consent
Written informed consent taken for patient information and images to be published.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.