
Abstract
HIV prevention efforts have historically focused on people aged 15–49 years, despite mounting evidence of risk behavior and increased disease burden among older adults. We analyzed survey data from 600 adults aged ≥50 years in the Rombo District of Tanzania. Logistic regression models were performed to evaluate individual and partner-level factors associated with HIV testing and counseling (HTC) uptake. In this sample, more than half of participants were sexually active and condom use was rare, but only 57% had ever been tested for HIV. Ten were HIV infected (1.7%); this prevalence was approximately one-third that observed among the general population in Tanzania (4.7%). Individual factors associated with increased HTC uptake included younger age, female gender, greater educational attainment, and having health insurance. Partner factors associated with increased HTC uptake included lower partner age and higher partner education. This population demonstrated substantial HIV risk, warranting tailored interventions to raise awareness and increase HTC uptake.
Keywords
Introduction
The UNAIDS ‘90–90–90’ goals call for HIV ‘treatment for all’ by improving rates of identification, care engagement, and viral suppression among all people living with HIV.1 Identification of HIV is crucial, as it is estimated that 50–70% of new HIV infections arise from sexual contact with individuals who are unaware of their HIV status. 2
Therefore, HIV testing and counseling (HTC) uptake is a vital step for entry into HIV care and linkage to antiretroviral therapy (ART). Participation in HTC is associated with earlier diagnosis, improved ART adherence, and improved HIV outcomes among those who test positive, and reduced sexual risk behavior and enhanced HIV knowledge among those who test negative.3–5 In Tanzania, a facility-based HTC approach (stand-alone HIV testing facilities and health clinics) was implemented at the beginning of the HIV pandemic. In order to increase access and uptake of HTC, other innovative approaches were introduced including home-based HTC, mobile or outreach HTC, and later HIV self-testing.6–11
Although there has been increased global attention to HTC, current HIV prevention strategies have mainly focused on persons between the ages of 15 and 49 years.12,13 Data and programs targeting older adults are scarce, particularly in sub-Saharan Africa.14,15 This is despite the fact that 17% of newly diagnosed cases occurred among individuals over the age of 5016 and global prevalence more than doubled among this demographic from 1995 to 2013.17 The limited attention to older adults is perhaps due to common misconceptions about reduced sexual activity among older individuals or assumptions that sexual activity in this group is limited to monogamous, heterosexual relationships. 18 However, individuals in this age group are prone to engaging in HIV risk behaviors, including low use of condoms, casual sex, and sex with multiple partners. 15
Factors associated with HTC uptake in individuals 15–49 years old have been well documented, including in sub-Saharan Africa.19,20 They include individual factors such as education, relationship factors such as desiring to be tested before marriage, health system factors such as encouragement by a health worker, and community or society-level factors such as stigma and exposure to media. However, these factors are less understood and may be different among older adults. This gap in knowledge is crucial for HIV prevention efforts, particularly the development of targeted interventions for this age group. To address this gap, we examined individual and partner factors associated with HTC uptake among individuals ≥50 years old in a district of Northern Tanzania.
Methods
We analyzed data from a cross-sectional survey conducted with 600 older adults ≥50 years of age in the Rombo District of Northern Tanzania between April and June 2015. In order to increase randomness of the study sample, participants were identified by multistage sampling. First, individuals aged 50 years and older were randomly selected from village registers, and then visited at their home and invited to participate. If the participant was not at home, researchers made two additional attempts before declaring that a participant could not be reached. Additional details on the sampling methods for the study are described elsewhere. 21
After obtaining informed consent, paper-based, structured surveys were administered in person in Kiswahili, followed by HIV testing according to Tanzanian national guidelines. 22 Surveys were administered in a private place in/near the home or at the village/ward office, depending on the preference of the participant. HIV testing included pre-test counseling, initial testing of a finger-pricked blood sample, a confirmatory test for those who tested positive, and post-test counseling. Those who tested HIV-positive were informed of the result and referred to a nearby district hospital for ongoing HIV care. The study received ethical approval from the Institutional Review Board of Kilimanjaro Christian Medical University College and from the Rombo District Authority.
Instruments
Data collected included individuals’ socio-demographic information, knowledge of HIV prevention and transmission, risk perception and awareness, and past use of HTC services. We also collected demographic information for their most recent sexual partner.
Demographic information
Individual-level determinants included age, gender, education, and insurance status.
Past counseling and testing
HTC uptake, which was the dependent variable, was coded 1 if an individual had ever been counseled and tested for HIV and 0 if they had never been counseled and tested.
HIV risk behaviors
Alcohol use, self-assessed risk of acquiring HIV, condom use, and sexual activity in the past three months.
Partner characteristics
Relationship characteristics included relationships status, as well as any partners’ age and education.
Statistical analysis
Statistical analysis was performed using Stata Version 14 (StataCorp LP, Texas). Descriptive statistics were used to summarize the analytical sample. We fit bivariate logistic regression models to assess individual and partner-level determinants of HTC uptake. Variables with p values < 0.20 were included in the final multivariable models. For multivariable analyses, a logistic regression model was used to evaluate how individual and partner factors were associated with HTC uptake. All associations were presented as adjusted odds ratios (aORs) with 95% confidence intervals (CIs).
Results
Of the 600 individuals surveyed, 342 (57.0%) had previously tested for HIV and 10 (1.7%) tested HIV-positive, with a higher prevalence among women (2.1%) than men (1.3%). Of the ten participants who were confirmed to be HIV infected, eight reported that they were aware of their HIV status. Participant ages ranged from 50 to 90 years, with a mean age of 65 years (SD = 10.3 years). There were more males than females (n = 311, 51.8%) and most participants (n = 558, 93.0%) had not completed secondary school. Approximately two-thirds of participants (n = 415, 69.2%) were married, while the remainder (n = 185, 30.8%) were single, divorced, widowed, or separated. More than half of participants (n = 350, 58.3%) had health insurance. Most participants (n = 426, 71.0%) self-reported having ‘no risk’ of acquiring HIV despite the fact that more than a half (n = 310, 51.8%) reported having sex in the past three months and condom use was very rare (3.3% at last sexual encounter; see Table 1).
General individual and partner characteristics of older adults by HIV testing.

HIV: human immunodeficiency virus.
Individual determinants of HTC uptake
Compared to those who had no formal education, those who had primary and those who had secondary/higher education had increased odds of HTC uptake (aOR = 2.6; 95% CI 1.6–4.0) and (aOR = 2.0; 95% CI 1.0– 4.4), respectively. Having health insurance was also associated with increased odds of HTC uptake (aOR = 1.7; 95% CI 1.2–2.6). Compared to those who were between 50 and 59 years old, those who were ≥70 years had reduced odds of HTC uptake (aOR = 0.4; 95% CI 0.3–0.7). Compared to individuals who did not drink alcohol, those who reported that they drank 6–7 days per week had decreased odds of HTC uptake (aOR = 0.6; 95% CI 0.3–1.0). Finally, being male was associated with lower odds of HTC uptake (aOR = 0.5; 95% CI 0.3–0.7).
Relationship determinants of HTC uptake
Among those with partners, the partner’s age and education were associated with HTC uptake. Compared to participants whose partners were between 50 and 59 years old, those whose partners were ≥70 years had decreased odds of HTC uptake (aOR 0.4; 95% CI 0.3–0.7). Compared to those whose partners had no formal education, participants whose partners had primary school (aOR = 2.5; 95% CI 1.7–3.8) or secondary education (aOR = 2.0; 95% CI 1.4–5.9) had increased odds of HTC uptake (Table 2).
Multivariate correlates of HIV testing among older adults (≥50 years) in Northern Tanzania.
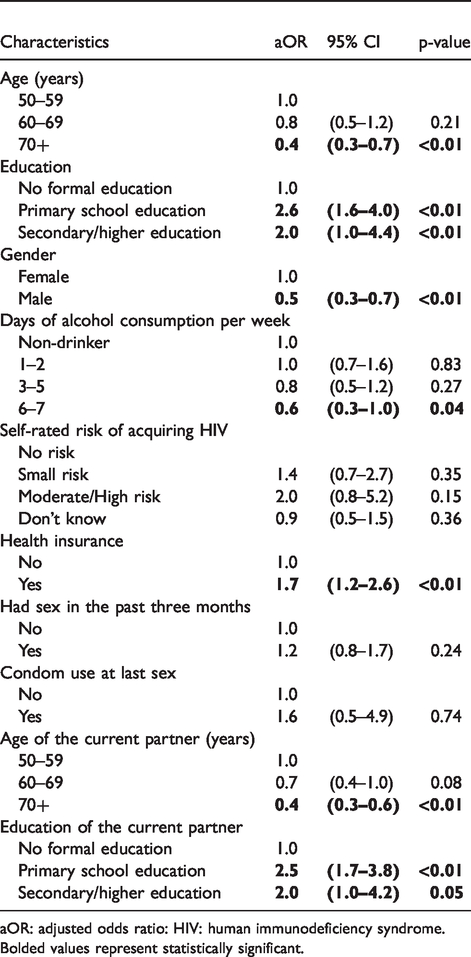
aOR: adjusted odds ratio: HIV: human immunodeficiency syndrome.
Bolded values represent statistically significant.
Discussion
In this study of individuals ≥50 years old, we found that several individual- and relationship-level factors were significantly associated with HTC uptake. Specifically, at the individual level, higher education level, having health insurance, lower age, female gender, and lower alcohol use were all associated with increased HTC uptake. Among those with partners, partner factors associated with HTC uptake were lower age and higher education of the partner. The positive associations between female gender 23 and higher educational attainment with increased HTC uptake have been observed in several other studies.24–26 However, these studies were not specific to older adults. At the relationship level, a more educated partner may exert more influence on the health behaviors of their counterpart. 27 This may be due to increased knowledge and awareness of HIV risk and the benefits of HTC. The reasons for lower uptake among those with older partners are less understood. We would speculate that this may be due to perceived lower risk of HIV.
In a systematic review of studies that primarily focused on testing among younger individuals, age was not significantly associated with HTC uptake. 23 However, our study found heterogeneous HTC uptake among age groups, with those 70 and older reporting lower levels of testing than those in the 50–59 age group. At the relationship level, participants with older partners were also less likely to test. These results may be explained by the perception of low risk of HIV acquisition among older individuals, which may continue to strengthen as people age. Other potential explanations are that members of the older generation may have less access to educational materials about HIV, may be less likely to engage in conversations with others about HIV, or may be less capable of accessing testing services. These are important areas for future study, as increased uptake of HTC among older adults may lead to earlier HIV diagnosis and several associated health benefits.
We also observed that alcohol consumption was associated with lower odds of HTC uptake. The Kilimanjaro region, where the Rombo District is situated, has been previously shown to have one of the highest levels of alcohol intake in Tanzania. 28 In studies of younger individuals at-risk for HIV, excessive drinking was associated with increased risk behavior and lower overall health, including lower uptake of preventative services like regular HIV testing.29,30 Our study findings suggest that this behavior has similar effects on HTC uptake across different age groups.
More than a half of the individuals in the study reported having sex in the past three months. Common misconceptions about reduced sexual activity among older individuals may be directly related to reduced attention to older adults in HIV prevention efforts and may have contributed to the low uptake of HTC in this population. Interestingly, we did not find association between the number of lifetime partners and HTC uptake. This may be because of the selected age range of the study population. At the age of 50 years and above, the lifetime number of partners may not have the same effect on personal perceptions of HIV risk, and therefore may not predict HTC uptake as it would for younger individuals.
Our study had several limitations. First, this was a cross-sectional study and therefore temporal association cannot be established. Given that we did not gather data on the timing of HTC, some of the explanatory variables (e.g. health insurance status, alcohol consumption, condom use at last sex encounter) could have occurred either before or after HTC, thereby introducing bias. However, we included the variables because they have been associated with HTC in previous studies.11,31 Second, the survey did not include items exploring several well-known factors that could potentially influence HTC uptake in this sample, such as having multiple sexual partners and experiences of HIV stigma. Third, study participants came from a single district in Northern Tanzania and therefore results may not be generalizable to the entire country. However, in our approach, we utilized multistage sampling to increase randomness. Recall bias is likely because some of the survey questions asked about partner characteristics and behaviors that may have occurred months or even years prior (e.g. last sexual activity). Moreover, self-reported past engagement in HTC and HIV risk may also limit our findings, since these were not corroborated by additional data sources.
Conclusion
Our findings suggest that both individual and partner factors were predictive of HTC uptake in individuals ≥50 years old, HIV risk was perceived as low among participants despite substantial risk behavior, and prior engagement with HTC was suboptimal. Therefore, targeted interventions are needed to improve HTC uptake among adults aged ≥50, and programs should encourage partner involvement. Future research should focus on the acceptability of HTC in this population, identifying and evaluating adaptations to standard HTC to meet the needs of older adults, and the gathering of longitudinal data to assess temporality and causality in factors associated with HTC uptake among older individuals.
Footnotes
Acknowledgments
We would like to thank the study participants for their time and willingness to provide this information. We also thank the District Executive Director and District Medical Officer of Rombo for permission to conduct the study. We are grateful to the Ward and Village leaders for introducing the research team in their respective areas.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received support from the U.S. Health Resources and Services Administration through the Medical Education Partnership Initiative (Grant # T84HA21123). CM was supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under Award # U01HL142099; Fogarty International Center Training Grant numbers D43TW010138 and D43-TW009595; and National Institute of Minority Health and Development Grant # R01 MD013493-01. The content is solely the responsibility of the authors and does not necessarily represent the views of the National Institutes of Health.