
Abstract
HIV self-testing (HIVST) offers an alternative to facility-based voluntary counseling and testing (VCT) services, particularly for vulnerable populations such as adolescents. This study aimed to determine the sociodemographic factors associated with adolescents preferring home-based HIVST over facility-based VCT in Kisangani, Democratic Republic of the Congo. A representative cross-sectional study using random sampling in clusters at three levels was conducted among adolescents (aged 15–19 years) to assess their hypothetical preference in home-based HIVST over facility-based VCT by a face-to-face, paper-based, semi-structured questionnaire, and logistic regression for statistical analysis. In 353 households, 754 adolescents were assessed for eligibility, of whom 628 were eligible. A total of 597 adolescents completed the study questionnaire. A majority of participants were aged 18–19 and of female gender. More than two-thirds of participants had never been tested for HIV and had no knowledge about HIVST before this survey. Among 597 adolescents who had completed the study questionnaire, a slight majority of participants (323/597; 54.1% [95% CI: 50.0–58.0]) preferred home-based HIVST over facility-based VCT. In a multivariate analysis, male gender (adjusted OR: 1.5, 95% CI: 1.1–2.1), marriage or partnered civil status (adjusted OR: 1.8, 95% CI: 1.1–3.1), and previous knowledge about HIVST (adjusted OR: 4.2, 95% CI: 2.6–6.8) were associated with preference for home-based HIVST over facility-based VCT. This study demonstrates that more adolescents preferred home-based HIVST over facility-based VCT in Kisangani. These observations suggest the existence of a specific sociodemographic profile associated with the acceptance of HIVST in adolescents living in sub-Saharan Africa.
Introduction
HIV testing, being the gateway to care, remains deficient among adolescents, e.g. aged between 10 and 19 years, 1 in sub-Saharan Africa where AIDS has become the leading cause of death among adolescents.2–4 Less than 20% of African adolescents know their HIV status, 3 while nearly 90% of HIV-positive adolescents in the world live in sub-Saharan Africa, and approximately 80% of all adolescent girls aged 15–19 years newly infected with HIV live in Africa.3,5 Uptake of HIV testing services is often low among adolescents due to multiple factors such as stigma and discrimination, fear over loss of privacy and confidentiality, the age of consent barrier, etc.6–8
HIV self-testing (HIVST) offers an alternative to facility-based voluntary counseling and testing (VCT) services, particularly for key populations (men who have sex with men [MSM], female sex workers, transgender people),9,10 as well as vulnerable populations such as adolescents.10,11 Currently, many African countries have policies supporting HIVST based on demonstrated evidence reported in the literature, 12 including HIVST data among adolescents.13–16 The highest rate of uptake of directly-assisted community-based HIVST, including door-to-door distribution of HIV self-tests, was reported among adolescents. 11 Furthermore, a recent rigorous evaluation of a door-to-door HIVST program demonstrated that knowledge of HIV status increased mainly among young adults aged 16–29 years, particularly among men, but unexpectedly not among women. 17
In the Democratic Republic of the Congo (DRC), where less than 10% of adolescents know their HIV status, 5 a recent field survey conducted among adolescents living in Kisangani demonstrated that door-to-door HIVST using a blood-based self-test and peer-based approach can be used with a high degree of acceptability and feasibility. 16 In order to extend these previous findings, the present study was designed to address the issue of the sociodemographic factors associated with the preference of home-based HIVST over facility-based VCT in adolescents living in Kisangani, DRC.
Study design and methods
This cross-sectional study was nested in a previously reported study in a population-based sample of adolescents in Kisangani, DRC, 16 consisting of a door-to-door survey using a capillary blood-based HIV self-test (Exacto Test HIV Self-test, Biosynex, Strasbourg, France), 18 and a peer-based supervised HIVST approach.
Kisangani is the capital city of Tshopo province and the third largest urbanized city in the DRC, comprising 1.6 million inhabitants, where 20% are adolescents, and the HIV seroprevalence rate is 2.3% in individuals aged 15–49 years.19,20 According to the law in DRC, the age required for a child to be employed is 16 years, and the legal age for marriage is 18 years for boys and 14 years for girls. Finally, the age adopted by law for participation in national and civil life is 18 years. 21
In brief, random sampling in clusters at three levels was used to select adolescents to survey during the vacation period (July–August 2018). All participants were volunteers recruited based on the following criteria: ignorance of own HIV status; being between 15 and 19 years of age; ability to speak and read French, Lingala, or Swahili languages; and signed informed consent. 16 Individuals not willing to be tested for HIV infection or not at home during the study team’s visit were excluded from the study.
The study protocol for this research has been previously described. 16 For this assessment, a face-to-face, paper-based, semi-structured questionnaire (in the participants’ chosen language: French, Lingala, or Swahili) to measure participant sociodemographic characteristics, HIV testing history, previous knowledge about the availability of HIVST outside this survey, self-reported sexual behavior, HIV risk perceptions, and preference for home-based HIVST over facility-based VCT was completed by all adolescents after performing the HIV self-test as an exit questionnaire, as previously described. 16 Note that all participants who were found to be HIV-positive with HIVST were provided with confirmatory testing and linkage to treatment and care.
The study was conducted after obtaining ethical approval from the Ethics Committee of the School of Public Health of the University of Kinshasa, constituting the National Ethics Committee of the DRC, and from the Ethics Committee of the University of Kisangani. Further permission was obtained from the Tshopo Provincial Health Division. Written informed consent was obtained from all participants or from their parents or guardians if the participants were minors according to the national recommendations (15–17 years). 22
Data were entered into an Excel database and analyzed using SPSS 20.0 (Chicago, IL). First, descriptive statistics were computed using mean (standard deviation) or median (interquartile range) for normal or skewed distribution, respectively, then, the 95% confidence intervals (CI) using the Wilson score bounds were calculated. Next, categorical data were compared using Pearson’s Chi square test, while Fisher’s exact test was used when the validity conditions of the latter test were not verified. Variables with a P-value < 0.2 in bivariate analysis and variables identified from the literature were entered into a full multivariate logistic regression model using stepwise model selection approach. A final multivariate regression model was carried out by integrating the variables with a P-value < 0.05 from full multivariate logistic regression. Missing values were replaced by the single imputation using regression technique because missing values were generally <0.5%.
Results
In 353 households enrolled by the study teams, 754 adolescents were assessed for eligibility, of whom 628 were eligible to participate. A total of 597 adolescents completed the study questionnaire (Figure 1). Baseline characteristics of the study participants are shown in Table 1. In brief, a majority of participants were aged 18–19 years and of female gender. More than two-thirds of participants had never been tested for HIV and had no knowledge about HIVST before this survey (Table 1).

Flow-chart showing the recruitment of study participants and their preference regarding home-based HIVST or facility-based VCT services. HIVST: HIV self-testing; VCT: voluntary counseling and testing.
Characteristics of 597 enrolled adolescents, living in Kisangani, Democratic Republic of the Congo.

aOverall missing values were <0.5% and were replaced by the single imputation using regression technique.
bOverall, 323/597 (54.1% [95% CI: 50.0–58.0]) adolescents preferred home-based HIV self-testing over facility-based voluntary counseling and testing.
cSelf-employed adolescents were engaged in for-profit activities such as trading, motorcycle taxi, or masonry.
Overall, a slight majority of participants (323/597; 54.1% [95% CI: 50.0–58.0]) preferred home-based HIVST over facility-based VCT (Figure 1 and Table 1). As shown in Table 1, both adolescents aged 18–19 (191/350 [54.6%]) and male teenagers (149/246 [60.6%]) preferred home-based HIVST. In addition, the majority of married or partnered (47/73; 64.4%) and self-employed adolescents (15/22; 68.2%) preferred home-based HIVST over facility-based VCT. Furthermore, 100/157 (63.7%) adolescents who were enrolled in a university program and 95/119 (79.8%) teenagers who had previous knowledge about HIVST preferred home-based HIVST over facility-based VCT.
In a bivariate analysis regarding the factors associated with adolescents preferring home-based HIVST over facility-based VCT (Table 2), male adolescents (P = 0.008) and those currently attending college, a technical school, or university program (P = 0.013 and P = 0.005, respectively), and those having previous knowledge about HIVST (P < 0.001) were more likely to prefer home-based HIVST over facility-based VCT.
Bivariate and multivariate analysis of factors associated with adolescents who prefer home-based HIV self-testing over facility-based voluntary counseling and testing.
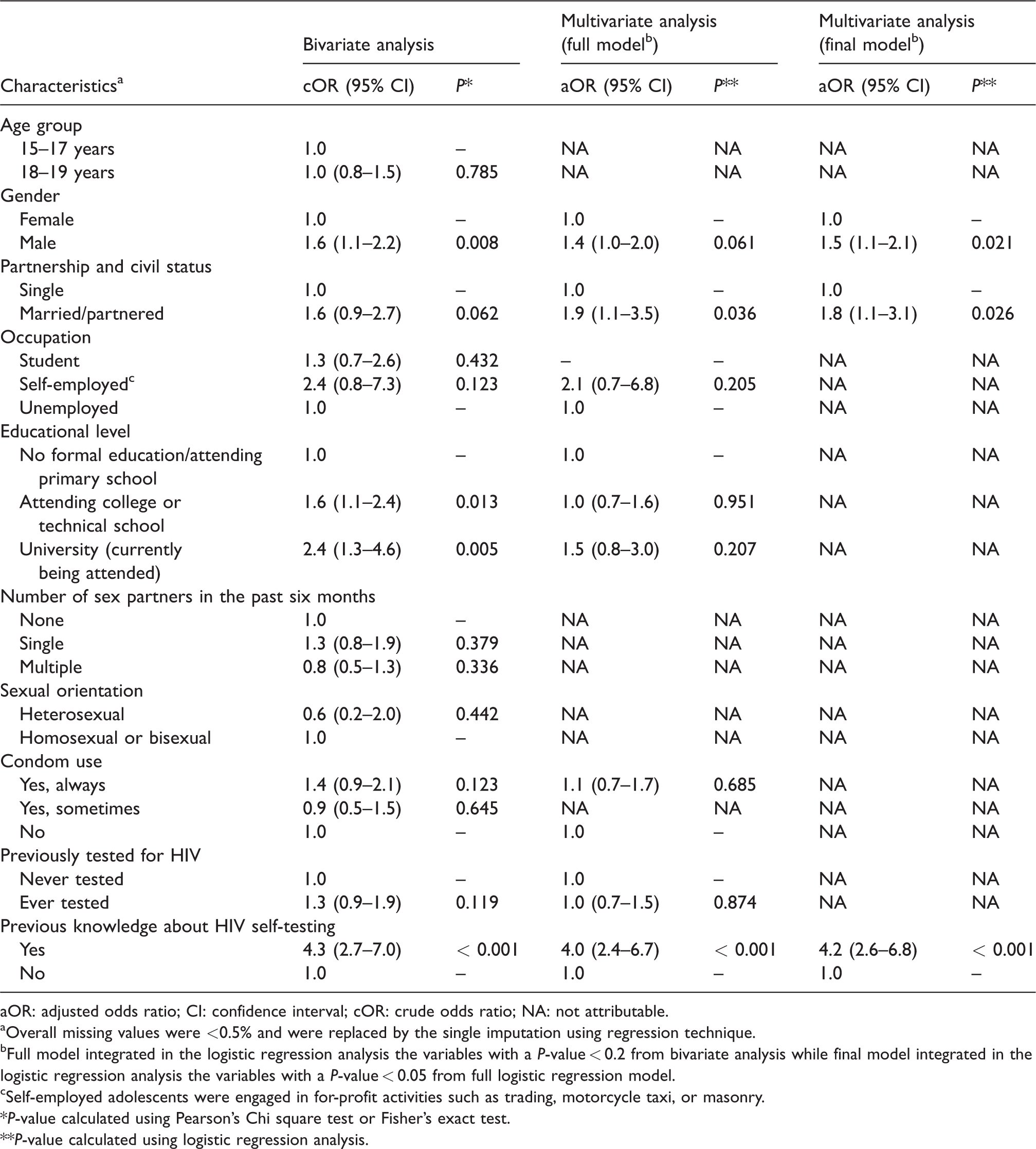
aOR: adjusted odds ratio; CI: confidence interval; cOR: crude odds ratio; NA: not attributable.
aOverall missing values were <0.5% and were replaced by the single imputation using regression technique.
bFull model integrated in the logistic regression analysis the variables with a P-value < 0.2 from bivariate analysis while final model integrated in the logistic regression analysis the variables with a P-value < 0.05 from full logistic regression model.
cSelf-employed adolescents were engaged in for-profit activities such as trading, motorcycle taxi, or masonry.
*P-value calculated using Pearson’s Chi square test or Fisher’s exact test.
**P-value calculated using logistic regression analysis.
Age, partnership, occupation, number of sex partners in the past six months, sexual orientation, condom use, and past history of HIV testing were not associated with a preference for home-based HIVST.
In multivariate analysis, male gender (adjusted OR: 1.5, 95% CI: 1.1–2.1), married or partnered civil status (adjusted OR: 1.8, 95% CI: 1.1–3.1), and previous knowledge about HIVST (OR: 4.2, 95% CI: 2.6–6.8) were associated with a preference for home-based HIVST over facility-based VCT.
Discussion
This study addresses sociodemographic factors associated with the preference for home-based HIVST compared with facility-based VCT among adolescents in Kisangani, DRC, a vulnerable and high-risk population for HIV. Data were collected using a survey administered during door-to-door capillary blood-based HIVST.
This study demonstrated that male gender, married or partnered civil status, and previous knowledge about HIVST constituted the sociodemographic factors significantly associated with adolescents preferring home-based HIVST over facility-based VCT. Taken together, these observations suggest that HIV testing programs focusing on adolescents living in the DRC could likely implement home-based HIVST to increase HIV testing among adolescents. Furthermore, HIVST among adolescents could be more effective in a subgroup of adolescents, mainly male adolescents with high education levels. 18
Effect of gender norms on HIVST among young adults was recently reported in Zambia. 17 Mulubwa et al. 17 demonstrated that knowledge of HIV status increased among young adults aged 16–29 years after a three-month intervention of door-to-door distribution of HIVST. These findings support our results showing that male gender is a relevant factor increasing the preference of HIVST. 17 However, previous studies assessing the acceptability of facility-based VCT versus home-based VCT did not find any association between sociodemographic characteristics of participants and their acceptance of home-based VCT. 23 However, home-based VCT was demonstrated to be the least costly strategy per client tested and was also cost effective in identifying HIV seropositive clients. 24 Since HIV testing is low among young men in sub-Saharan Africa due to fears over loss of privacy and confidentiality, stigma, and discrimination, HIVST offers a good opportunity to reach men who are not yet tested for HIV.7,8 By contrast, HIV incidence in sub-Saharan Africa is high among adolescent girls and young females aged 15–24 who are both at highest risk of HIV and particularly vulnerable. 5 Very often, the consideration of gender issues is limited to focusing on women as the main target of the programs (prevention of mother-to-child transmission, income-generating activities, etc.) without taking into account the impact of these intervention modalities on gender relations. Conversely, men are still far removed from testing and care centers, and constitute less than 20% of the active lines of HIV associations in sub-Saharan Africa, 10 suggesting differential effectiveness of the intervention by gender.
Previous studies have shown that high educational level was a factor that increases understanding of the instructions for use, the successful performance of the self-test, and the correct interpretation of the results.18,25 The present study shows that high educational level constitutes an independent factor that increased the preference of home-based HIVST among adolescents in Kisangani, DRC. Moreover, previous knowledge about HIVST increased the preference of home-based HIVST. However, despite multivariate logistic regression analysis, one of the two previous factors could constitute a confounding factor, simply because HIV education is mandatory during college and university courses according to the recommendations of the National Program for Adolescent Health in DRC. 19 Thus, the most educated adolescents are more likely to be informed about HIV and HIVST through college and university courses.
Strengths and limitations
The study has several strengths. First, it focused on the vulnerable adolescent population, that is at high-risk for HIV infection and for whom HIVST could constitute a complementary solution for HIV testing access 10 in the poorly documented cultural context of the DRC. Second, our study provided clarification on the profile of adolescents to guide targeted HIVST implementation strategies such as HIVST in the home. The study has, however, some limitations. Selection bias may have occurred, as the study population comprised mostly women. Furthermore, selection bias due to exclusion of participants who refused HIV testing may have occurred; however, the impact is likely negligible given that this group represented less than 5% of the larger study population, including adolescents. Finally providing only blood-based HIVST and supervised HIVST limited the study observations to this type of self-test and distribution approach. However, previous studies have shown that oral fluid-based HIVST and unsupervised HIVST were more accepted by key populations, such as MSM and female sex workers. 26
Conclusion
This study demonstrated that more adolescents preferred home-based HIVST over facility-based VCT in Kisangani, DRC. Male gender, married or partnered civil status, and previous knowledge about HIVST were found to be factors associated with adolescents preferring home-based HIVST over facility-based VCT. These observations suggest the existence of a specific sociodemographic profile associated with acceptance of HIVST in adolescents living in sub-Saharan Africa.
Footnotes
Authors’ contributions
ST-W, SB-A, CKT, and LB conceived and designed the research; ST-W performed volunteer recruitment, follow-up, and performed the experiments; ST-W, R-SMB, and ATT performed statistical analyses; ST-W and LB analyzed the results and drafted the manuscript.
Acknowledgments
The authors are grateful to the adolescents for their willingness to participate in the study. We thank the National AIDS & STI Control Program, Kinshasa, Democratic Republic of the Congo. We would also like to thank Dr Désiré Djoza and Dr Eric Adjaye for excellent technical assistance during the study. Finally, we thank Mr Geoffrey M. Graham for editing the language of our manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.