
Abstract
Female and male condoms are the only methods that prevent both sexually transmitted infections (STIs), including HIV, and unintended pregnancy. Despite continuing high STI rates, few studies investigate factors predicting whether women initiating female condom (FC) use sustain use. Using data from a randomized trial, we examined predictors of sustained FC use at five-month follow-up (FU2) among female university students in South Africa who participated in either a one-session, information-only, group-delivered Minimal Intervention or a two-session, group-delivered Enhanced Intervention. In the final multiple logistic regression model, believing one’s partner holds positive attitudes toward the FC (aOR = 1.40; p = 0.028), and greater FC use for vaginal sex at previous assessment (aOR) = 1.19; p = 0.008) were associated with greater odds of FC use at FU2. Excluding number of FC-protected occasions at FU1 from the analysis, discussing FC use with partner (aOR = 2.89; p = 0.071) and believing one’s partner holds positive attitudes toward the FC (aOR = 1.63; p < 0.001) were associated with greater odds of use at FU2. The FC empowers women to protect themselves from both STIs and unintended pregnancy, but targeted interventions are needed to address men’s negative attitudes toward the device. Engaging men as FC champions to support and promote FC use, along with marketing campaigns targeted to men, may expand FC coverage and enhance uptake.
Introduction
Breakthroughs in “treatment as prevention” (TasP) 1 and pre-exposure prophylaxis (PrEP)2,3 have led the global public health community to embrace the goal of an AIDS-free generation. However, PrEP does not prevent sexually transmitted infections (STIs).4,5 Investment in other promising HIV biomedical prevention technologies in the development pipeline (including vaginal and rectal microbicides, preventive vaccines, multipurpose technologies for pregnancy and HIV prevention, and broadly neutralizing monoclonal antibodies 6 ) may surmount limitations of the male condom, especially those that minimize or eliminate the need for negotiated protection with partners. In the meantime, condoms (male and female) remain the only method to prevent STIs. The male condom is limited by being male-controlled, leaving the female condom (FC) as the only female-controlled method that protects against pregnancy, 7 HIV and other STIs.8,9 No one method will meet the needs of all women and men, especially young people; rather, offering multiple prevention options that fit the context of people’s lives and changing needs is essential. A South African national population-based survey found that only 58.4% of young women and men aged 15–24 years reported using a condom at last sex, 45.7% used a condom every time with their most recent sexual partner; condom use in this age group declined between 2008 and 2012. 10 In the Ring (IPM 027)11 and ASPIRE (MTN-020)12 clinical trials, little to no protection was provided among young women aged 18–21 years due to sub-optimal adherence.
The FC has been shown to be as effective as the male condom, 13 acceptable 14 and cost-effective.15–17 Several new FC brands have been approved by WHO/UNFPA and are now available. 18 Moreover, women may find it easier to inform their partners that they are using the FC as a contraceptive, thus circumventing discussion of disease prevention. 19 However, it remains an under-promoted and under-utilized method of triple protection against HIV/STIs and pregnancy. In South Africa, where the STI burden is very high, 20 including among adolescents and young people,21,22 FCs, unlike PrEP or TasP, can play a critical role in STI prevention.
A secondary analysis of STI data from the ECHO Trial, 23 a multi-country randomized trial which assessed HIV incidence among 7829 women from 12 sites in Eswatini, Kenya, South Africa, and Zambia who were randomized to intramuscular depot medroxyprogesterone acetate, a copper intrauterine device, or a levonorgestrel implant showed high rates of STIs among participants. At screening, Neisseria gonorrhoeae (NG) prevalence was 4.7% and Chlamydia trachomatis (CT) prevalence was 18.2%, with higher prevalence among women aged 24 years and younger versus those older than 24. Despite intensive counselling about HIV/STI prevention and the provision of STI treatment during follow-up visits, STI prevalence at the final visit was still high at 4.8% for NG and 15.4% for CT. Contraceptive continuation was high and pregnancy rates low across all contraceptive methods. 24 However, HIV incidence was high across all contraceptive methods, suggesting that ECHO participants who received intensive, comprehensive and integrated sexual and reproductive health counselling were able to successfully initiate and use the highly effective contraceptive methods, but were unable to protect themselves against STIs and HIV. This could be due to their inability to negotiate condom use with their partners.
Another study also showed high STI rates among 352 HIV-negative or unknown HIV status youth (16–24 years) in Durban and Soweto, South Africa; ≥1 laboratory-confirmed genital tract infections were identified in 70.2% of females. 21
South Africa has one of the largest government-funded public-sector FC programs in the world, 25 and one in which FC promotion is prioritized as a key component of a sexual and reproductive health services package. Data from the recent South Africa National FC Condom Evaluation indicated that the FC was perceived as a gateway to providing young people with sexual and reproductive health services; however, of 4442 anonymous surveys among women and men attending 114 primary health clinics, only 19.3% had ever used a FC, two-thirds of whom had used them for protection against both pregnancy and STI/HIV. 26 The proportion of users under 20 years was low, with only 7.7% of women and 6.1% of men aged 16–18 years reporting ever using the FC.
There are relatively few studies of FC use among university students in South Africa and elsewhere in sub-Saharan Africa (SSA).27–31 In the primary analyses for this study, which compared a two-session small-group intervention to a similar one-session intervention, we found that women in both groups reduced their number of unprotected vaginal intercourse occasions and increased the number of FCs used from baseline to both the 2.5-month (FU1) and 5-month (FU2) follow-ups, with no significant differences between the two groups. 28
In the present analysis, we aimed to identify predictors of FC use measured at FU1 associated with use of the FC at FU2 among university women who were exposed to either intervention.
Methods
Participants and procedures
Between March 2008 and October 2009, we recruited female university students in KwaZulu-Natal Province, South Africa, via outreach at campus sites where students congregated. Eligibility criteria for enrolment were: 18 years or older; full-time students; HIV-negative or unknown serostatus (self-reported); not pregnant or wanting to become pregnant in the next nine months; reported condom-unprotected vaginal intercourse in the past two months; had the capacity to complete informed consent and be interviewed; and willing to have assessments and interventions audio-recorded. Following screening, eligible students completed written informed consent and were scheduled for a baseline interview. Participants were then invited to attend an intervention randomization meeting within three weeks, where they were randomly assigned, in blocks of two, to either a one session, information-only, group-delivered Minimal Intervention (MI) or a two-session group-delivered Enhanced Intervention (EI), which included didactic information delivered in the MI, in addition to behavioral rehearsal of FC use, partner negotiation, and opportunity to practice these skills and problem-solve in the second session (detail described elsewhere). 28 Follow-up assessments were conducted at 2.5 and 5 months post-intervention, with assessment intervals linked to the academic calendar. Participants received the equivalent of $4 for baseline, $10 for FU1 assessment, and $15 for FU2 interview. All participants completed written informed consent. The Institutional Review Board of the New York State Psychiatric Institute and Research Ethics Committees at two South African universities approved study procedures.
Measures
Selection of variables that might be predictive of FC use at FU2 was guided by the Information-Motivation-Behavior Skills Model (IMB) 32 and the Theory of Gender and Power. 33 Table 1 presents the variables used linked to the two theories. We hypothesized that more gender-equitable norms, e.g., discussion of condom use before sex, and refusal of condomless sex, would be associated with FC uptake. We also expected that participants who reported a history of physical abuse or sexual coercion might be likely to use the FC because it is a method under their control. Finally, we expected that participants who had used the FC at FU1 would be more likely to report FC use at FU2.
Measures.

Primary outcome
The dependent variable, measured at FU2 interview, was a binary indicator of any FC use since the FU1 interview.
Predictor variables
With the exception of demographics, all variables used in this analysis were measured at FU1 (i.e., not measured at baseline), which occurred approximately ten weeks after participants completed the MI and EI. Since women had little experience with the FC at baseline, and all had undergone an intervention that affected their sexual behavior prior to FU1, 28 we used FU1 measures of other independent variables that were not assessed at baseline. Table 1 describes the predictor variables assessed in this study.
Statistical analysis
For these analyses, of the 233 participants who participated in either the EI or MI intervention and completed FU2 interviews, we included 199 people who had valid responses regarding FC use at FU2.
Descriptive statistics were generated for demographic variables and key potential FU1 predictors of participants’ use of the FC at FU2. We created several scales and report mean and range of the scaled variables. For categorical variables, we report the count of positive answers (“yes”) and proportion among the 199 participants in the analysis sample. Simple logistic regression analysis was employed to examine the association between each variable and FC use at FU2. For the test of each bivariate association, a p value ≤0.05 was considered as statistically significant.
We then used the stepwise model selection procedure to identify a prediction model for FC use at FU2. Only those predictors with corresponding p values ≤0.10 were considered at the beginning of this selection procedure. Two models were run: one that had all potential predictors including number of FCs used at FU1, and another that excluded this variable. The first model assessed whether any of the measures had an effect on FC use at five months over and above the effect of having used the FC two months after the intervention. The second model assessed the effect of the predictors apart from any influence they might have had on FC use at FU1. The stepwise method is a modification of the forward-selection technique and differs in that variables already in the model do not necessarily remain in the model. As in the forward selection method, variables are added one by one to the model, and the variable to be added must be significant. We considered a p value ≤0.10 as statistically significant in this model selection process. The data were analyzed using the PASW SPSS version 18.0. 39
Results
Sample characteristics
Participants were full-time students, Black, with average age of 20.4 years (SD = 1.9). The major home language was isiZulu (81.4%). Participants were primarily Charismatic/Evangelical (24.1%), Protestant (21.6%), and Roman Catholic (20.6%).
Partner characteristics
Most participants (95.9%) reported having a main partner and the mean partner age was 24.0 years (SD = 3.5) (Table 2). Nearly 17% reported that they were partially or totally financially dependent on their partners. Nearly four-fifths reported their partner had tested for HIV and nearly 10% that their partners had ever been diagnosed with an STI. Participants felt at risk for acquiring HIV (40%) and STIs (45%) from their partners.
Partner characteristics and perceived partner risk.

FC use at baseline and FU1
In our analysis sample, only 4.1% of participants reported having ever used the FC at baseline, prior to the intervention. In contrast, 98.5% of participants reported ever having used the male condom. At FU1, 62.6% reported having used the FC post-intervention.
Bivariate analyses
FC use at FU2
At FU2, 38.2% reported that they had used the FC since their FU1 interview. The associations of independent variables with FC use at FU2 in simple logistic regression analyses are shown in Table 3. The odds of FC use were 1.85 times greater among those who, at FU1, had any friend who had used a FC compared to those who did not (p = 0.049). The perception that partners had positive FC attitudes at FU1 was associated with higher odds of FC use at FU2 (OR = 1.61, p = 0.001). Participants who discussed using the FC with a partner at FU1 had 3.18 times the odds of using the FC at FU2 than those who did not (p = 0.043). There was a 25% increase in the odds of using the FC at FU2 for every additional FC-protected occasion at FU1 (OR = 1.25). Gender roles, relationship control, ever physical abuse and ever sexual coercion, perceptions of pregnancy and HIV risk, FC knowledge, and FC self-efficacy were not associated with FC use at FU2.
Simple logistic regressions associating any FC use at FU2 with FU1 hypothesized predictors (N = 199).
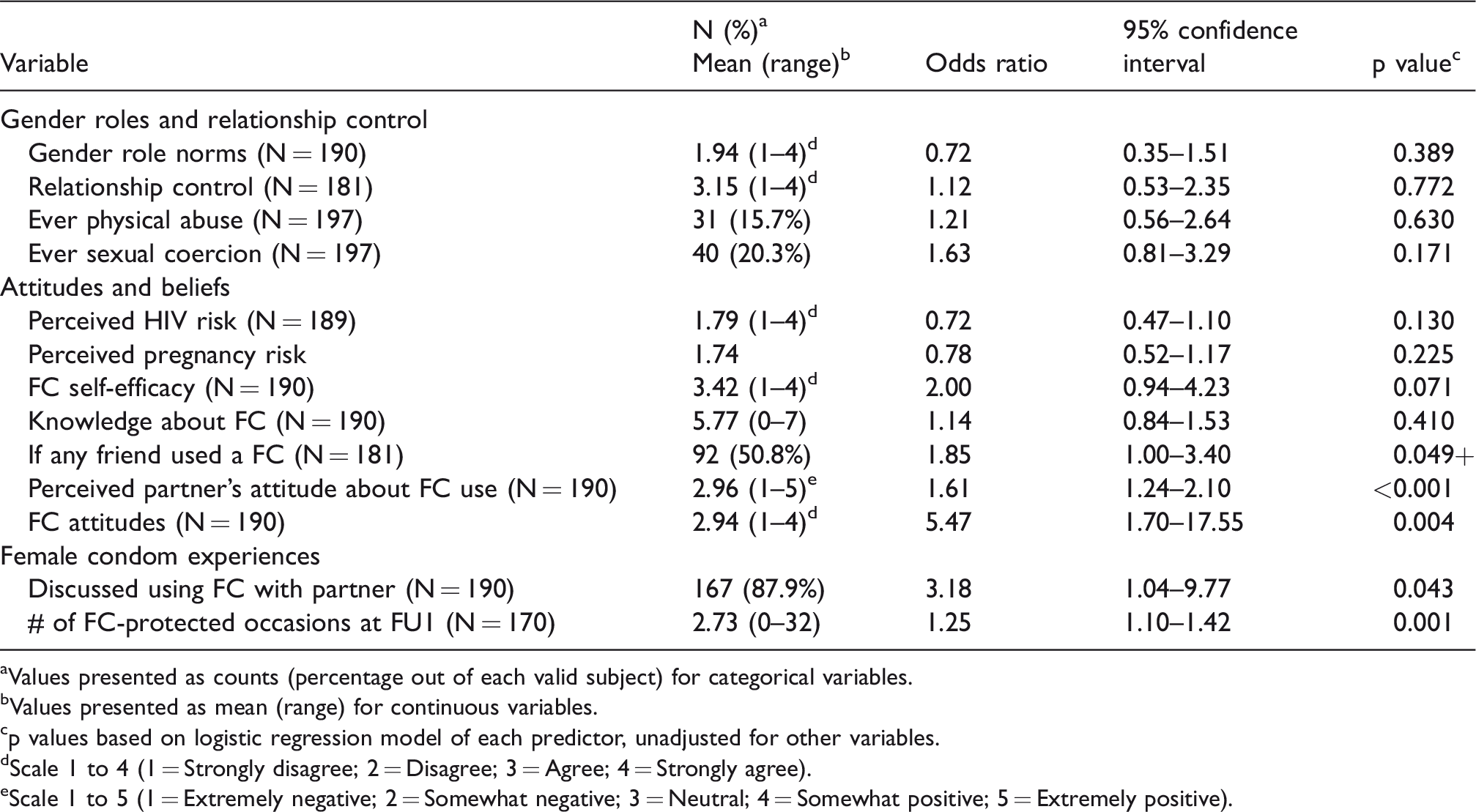
aValues presented as counts (percentage out of each valid subject) for categorical variables.
bValues presented as mean (range) for continuous variables.
cp values based on logistic regression model of each predictor, unadjusted for other variables.
dScale 1 to 4 (1 = Strongly disagree; 2 = Disagree; 3 = Agree; 4 = Strongly agree).
eScale 1 to 5 (1 = Extremely negative; 2 = Somewhat negative; 3 = Neutral; 4 = Somewhat positive; 5 = Extremely positive).
The final multiple logistic regression model in Table 4 was derived from a stepwise model selection procedure starting with all predictors in Table 1 included, with removal level at p > 0.10. In the final multiple logistic regression model for the total sample, believing one’s partner holds positive attitudes toward the FC (adjusted odds ratio [aOR] = 1.40; p = 0.028), and greater use of the FC for vaginal sex at FU1 (aOR = 1.19; p = 0.008), were associated with greater odds of using the FC at FU2.
Multiple logistic regression predicting FC use at FU2, including number of FC-protected occasions at FU1.
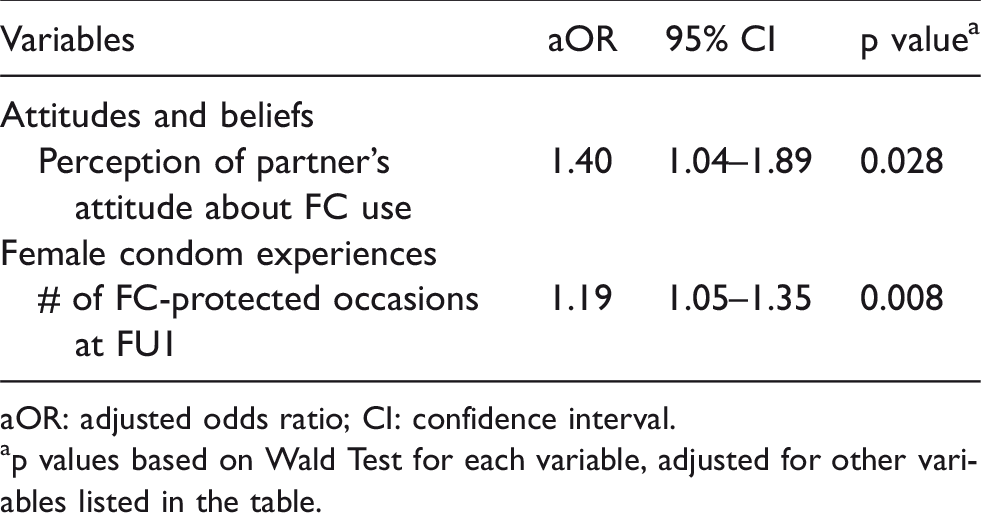
aOR: adjusted odds ratio; CI: confidence interval.
ap values based on Wald Test for each variable, adjusted for other variables listed in the table.
The final multiple logistic regression model in Table 5 was derived from a stepwise model selection procedure starting with the same predictors as those in Table 4 but excluding number of FC-protected occasions at FU1. In this model for the total sample, discussing use of FCs with partner (aOR = 2.89; p = 0.071) and believing one’s partner holds positive attitudes toward the FC (aOR = 1.63; p < 0.001) were associated with greater odds of using the FC at FU2.
Multiple logistic regression predicting FC use at FU2, excluding number of FC-protected occasions at FU1.
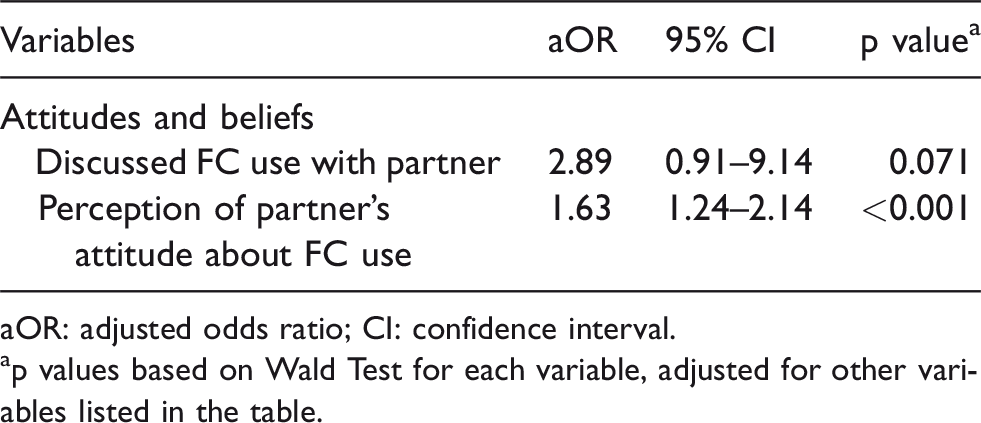
aOR: adjusted odds ratio; CI: confidence interval.
ap values based on Wald Test for each variable, adjusted for other variables listed in the table.
Discussion
In our study, participants reported significantly higher levels of sex acts protected by FCs five months post-intervention, and predictors of continued FC use were identified. We found that participants’ perception that their partners held positive attitudes about the FC and more FC-protected sex occasions at FU1 resulted in 1.40 the odds and 1.19 the odds, respectively, of having used the FC at five months FU. When we excluded prior number of FC-protected occasions in the regression, having discussed FC condom use with partner led to a nearly three-fold increase (aOR = 2.89) in continued FC use and the perception that partner had a positive attitude about FC use led to a 1.63 odds of continued FC use. A strength of this longitudinal design is that it allows us to conclude that positive perception of partner attitudes and discussion with partner are antecedent to subsequent FC use. In a study of US women and men, having positive attitudes about the FC significantly increased the odds of men using a FC (aOR = 7.61; CI = 3.09, 18.76; p < 0.001).40,41 Similarly, in a New York City FC intervention trial with family planning clinic clients, exploratory univariate analyses indicated that women who were satisfied with the FC or who believed their partner held positive attitudes about the FC were more likely to engage in repeated use of the FC. 42 In a cross-sectional study of 388 female undergraduate students from selected tertiary institutions in Oyo State, Nigeria, positive attitudes about the FC were associated with perceived confidence to use the FC, which potentially could result in increased condom use. 29
Contrary to expectations, variables selected based on the Theory of Gender and Power failed to associate with continued FC use at FU2. This may in part be a measurement issue. Our measure of Relationship Control used only four items from the Sexual Relationship Power scale. 35 Although our Gender Norms and Relationship Control measures were both reliable and evidenced face-validity, this was the first test of their construct validity, and it is unclear as to whether we adequately captured the constructs of interest. Neither physical abuse nor sexual coercion variables were associated with FC use at FU2. We had hypothesized that those who had a history of abuse or coercion may be more likely to initiate and maintain FC use because the FC may be less objectionable to men since it allows practice of safer sex without the restricted sensations that accompany male condom use. The relationship between abuse and coercion history may in fact be bi-directional, with some women more likely to initiate FC use, and others less likely due to preferences for skin-to-skin contact, anti-condom views, or belief that the visibility of the FC could result in partner’s objection. In addition, measurement error could have accounted for our non-significant findings as our measures of abuse and coercion were not specifically linked to FC use.
The lack of association between gender norms and FC use may also be due to shifting norms that allow greater sexual agency among young South African women; in particular, those at a higher education institution may be a more empowered population.
Male partner involvement and support are key to FC use, given that that sexual decision-making often is in the hands of men43–45 and that male partner resistance has been commonly cited as a significant barrier to its uptake. 44 Several studies in sub-Saharan Africa report male reluctance/refusal to use FCs, including 77.5% of 427 female Nigerian university students 46 and 17.8% of 242 women aged 18–49 recruited from a hospital in Zimbabwe. 47 In a qualitative study of 15 female university students who had ever used the FC in KwaZulu-Natal, South Africa, partners’ perception that the FC interferes with his sexual pleasure, was a deterrent to consistent FC use. 45
Other studies have found that male partners’ reaction to women asking their male partners to use the FC was a determinant of use.48,49 Beksinska et al. found that men were willing to assist their female partners with using the method and were influential in its use. 50 Findings from a couples-based intervention suggest that male partners can play an influential role in increasing FC use. 51 Several studies have found that men may enjoy using the FC52 and see advantages, including that women take responsibility for use and that it more comfortable than and less constrictive than the male condom.53–59 In a qualitative study (37 focus group discussions and 6 in-depth interviews) on the FC among men in urban and peri-urban areas in Cameroon, Nigeria and Zimbabwe, initiation of FC use by married men’s wives or stable girlfriends was not acceptable. 46 Although an accumulating number of studies highlight the importance of male partner involvement in FC use, few programs and interventions have targeted men. In a study of 38 men who were the current sexual partners of the female university students enrolled in our FC intervention, more than half reported that they had refused to use the FC when their partner first suggested it, 45 due in part to threatened masculinities.
FC use varies by type of sexual relationship and the level of sexual risk, as noted in a scoping review of FC in resource-constrained countries. 60 The majority of participants in our study had a main male partner and many felt at risk of acquiring HIV/STIs from their partner.
Empirical data predicting men’s influence on women’s FC use are limited. Much more needs to be understood about how to bring about greater FC knowledge, establish more favorable FC attitudes and norms among men, considering their documented influence on female partners, how to increase male partner involvement in FC promotion, and in what ways men’s support contribute to FC uptake and continued use.
Our findings suggest that men have a role in assisting and supporting their female partners’ use of the FC and point to the need for FC interventions with male partners and marketing campaigns targeted to men. However, of the more than 100 FC studies conducted to date, we identified 16 that included men, and only one included an intervention.27,31,40,43,45,46,51–56,58,59,61,62
Customizing FC demand-creation strategies and messages to persuade partners to support FC use is critical. Messaging that FC use can benefit men, e.g. increased sexual satisfaction and convenience of use, as well as shared responsibility for condom use in relationships and male introduction of the FC should be promoted. Rebranding and repackaging the FC to appeal to men may help to increase their FC use. Training men as FC champions to educate other men in social spaces where men congregate (workplace, sports events, men’s clubs) might be an approach to increase men’s interest in the FC and promoting its use with partners.
This is one of few studies that examine predictors of continued FC use among young women in SSA. South African university students are likely to be future leaders in society and may be better equipped to adopt to more equitable gender norms and be open to alternatives to the male condom. Given that the majority of study participants report having one main partner, relationship-based couples-level interventions focused on trust, communication and mutual decision-making might be useful. Also, student health services and HIV/AIDS educational programs in South Africa’s tertiary institutions provide a potential platform for reaching both women and men for disease and pregnancy prevention education, including advocacy of the FC as an additional option to male condoms.
The study has several limitations. First, FC use was self-reported and therefore may be subject to reporting bias, and the follow-up period was only five months. Second, data were collected at one tertiary institution and therefore may not be generalizable to students in other institutions of higher learning in South Africa. However, the numbers of tertiary students in South Africa are not insignificant; enrollment at public and private higher education institutions reached 1.1 million in 2016, and by 2030, is estimated to be 1.6 million. 63 Finally, we did not interview a sample of men. Despite these limitations, and although these data were collected some time ago, the study provides key information about factors influencing FC use which can inform the prevention messaging and targeting of promotional strategies.
Conclusions
At present, female and male condoms are the only methods that simultaneously prevent STI/HIV and pregnancy. While PrEP provides an effective option for HIV prevention, it does not protect against other STIs. Given persistently high STI rates, especially among youth, the triple protection afforded by FCs is a message to which young men may be receptive. Counseling on FC use should be built into standard clinical practice, and promotional programs and interventions should target male partners. Our study shows that young women’s use of the FC can be facilitated by positive attitudes and support from male partners. A decade ago Mantell, Stein and Susser made a strong plea for male partners to be “part of the bargain for barriers” 64 – it is high time this call is heeded, and concrete efforts are directed toward including men in FC programming.
Footnotes
Acknowledgements
We are grateful to the students who participated in this study and the valuable contributions of the study’s Community Advisory Board. We also acknowledge the contributions of the higher education institution who supported the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from NICHD (NICHD; R01-HD046351; Joanne E Mantell, MS, MSPH, PhD, Principal Investigator; Jennifer A Smit, PhD, South Africa Site Principal Investigator). The HIV Center for Clinical and Behavioral Studies at the New York State Psychiatric Institute and Columbia University is supported by a center grant from the National Institute of Mental Health (P30-MH43520; Principal Investigators: Anke A Ehrhardt (1987–2013)/Robert H Remien, PhD (2013–present)). The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Child Health and Human Development, the HIV Center for Clinical and Behavioral Studies at the New York State Psychiatric Institute and Columbia University and MatCH Research Unit (Maternal and Adolescent Child Health Research Unit), of the University of the Witwatersrand, Faculty of Health Sciences, Department of Obstetrics & Gynaecology.