
Abstract
In Malaysia, the HIV epidemic is concentrated in a highly stigmatized population, men who have sex with men (MSM). The relationship of multiple psychosocial health conditions and HIV risks have not been investigated. This study aims to assess the association of multiple psychosocial factors with risky sexual behaviour and HIV infection among MSM. Data on demographic characteristics, psychosocial health conditions, condomless anal intercourse (CAI), HIV testing and HIV status were collected via an anonymous online survey. Multivariable logistic regression model was used to determine whether psychosocial health conditions among MSM have a syndemic association with HIV status. Between July 2017 and February 2018, 622 MSM completed the online survey. Overall, 54.3% of participants reported engaging in CAI in the past three months and 46.0% were found to have two or more psychosocial health conditions. Increasing numbers of psychosocial health conditions (1, 2, 3, 4 or more) were significantly associated with HIV infection compared to those without psychosocial health condition (odds ratio [OR] 3.39, 95% confidence interval [CI]: 1.41–8.14; OR 3.51, 95% CI: 1.43–8.61; OR 4.22, 95% CI: 1.68–10.96, and OR 7.58, 95% CI: 2.44–23.55, respectively). Comprehensive HIV prevention programs addressing mental health and substance use are needed for MSM in Malaysia.
Introduction
Men who have sex with men (MSM) continue to bear the highest burden of the HIV epidemic worldwide including Asia because of biological factors as well as stigma, discrimination and barriers in accessing HIV testing and health care in general. The bio-behavioural surveillance survey conducted by the Ministry of Health found that the HIV prevalence among MSM in Malaysia had increased from 7.1% in 2012 to 8.8% in 2014, and to 21.6% in 2017. 1 The surge in the cases of HIV among MSM may be explained by high levels of risky sex behaviours and low uptake of HIV testing. 2 Low uptake of testing may drive HIV epidemics as HIV testing is the first step in entering the cascade of HIV. Knowledge of HIV status, initiation of and adherence to anti-retroviral therapy, and ultimately achieving viral suppression, are part of the broader treatment as prevention strategy. In Malaysia, criminalization of same-sex behaviours by sodomy law and Sharia law are structural barriers to HIV prevention as many MSM are afraid to disclose their sexual behaviour to their family, communities, and healthcare providers. 3 As a minority group that is discriminated against by Malaysian society, they may be vulnerable to psychosocial problems which have been shown to be associated with HIV infection.4,5
The sexual minority stress model postulates that the sources of mental health problems in lesbian, gay, bisexual and transgender (LGBT) populations are stigma, prejudice and discrimination. 6 The hostile environment against LGBT populations produces negative psychological outcomes such as expectations of rejection, hiding and concealing, internalised homophobia or homonegativity and problematic or maladaptive coping strategies. These negative psychological outcomes eventually lead to mental health conditions. Subsequently, Hatzenbuehler proposed psychological mediation framework, suggested that sexual minorities have difficulty in coping with stigma social or interpersonal problems, leading to mental health problems. 7 Hence, MSM are vulnerable to mental health conditions.
Past studies have also documented how these mental health conditions may overlap or synergistically drive each other. The term, syndemic, was first applied by Singer, in a study of HIV/AIDS among African Americans in the inner city of the United States, where HIV/AIDS was associated with underlying, interconnected problems such as mental health, substance use and violence. 8 Stall and colleagues then used the syndemic approach to explain the health disparities among MSM. They used this theory to examine the HIV risk in MSM in a syndemic approach focused on four specific psychosocial factors – poly-drug use, depression, childhood sexual abuse (CSA), and intimate partner violence (IPV) and concluded that the two or more psychosocial conditions interacting synergistically and contributing to an excess burden of HIV/AIDS in urban gay male populations in the United States.9,10 Since then, syndemics related to HIV risk and infection were reported among MSM from other Western countries5,11–14 and more recently, in China,4,15 Taiwan, 16 India,17,18 Vietnam, 19 and Thailand. 20
Previous research on MSM in Malaysia focused on social and behavioural factors related HIV infection among MSM. However, the relationship of psychosocial conditions and HIV infection among Malaysian MSM has never been examined. The primary objective of the study was to investigate the association and additive effects of multiple psychosocial factors (depressive symptoms, suicidal risk, “chemsex”, history of CSA and IPV) with HIV infection in this online sample of MSM.
Methods
Study setting
A cross-sectional analysis of an online study of HIV testing and sexual behaviours of MSM in Malaysia was conducted from July 2017 to February 2018. Advertisements about the survey were posted by non-government organization workers in social media such as Whatsapp as well as in popular gay dating application (Grindr). The survey was hosted by RedCap, a secure web-based electronic data capture system. 21 Interested participants were screened for eligibility by the following inclusion criteria: biologically male, at least 18 years old or older, having anal intercourse with another man in the past 12 months and being Malaysian citizen. On average, participants took 15–20 min to complete the survey.
In total, 2718 users accessed the survey, 1687 (62.1%) were screened and fulfilled the inclusion criteria, 1288 (47.4%) continued to the consent page and provided informed consent. Finally, in total, 622 (22.9%) completed the questionnaire.
Ethical consideration
The online survey was anonymous, with no personal identifiers such as name, address, or email addresses collected. Participant information sheet, informed consent page and questionnaire were available in both Bahasa Malaysia and English. The study was approved by the Medical Ethics Committee of the University Malaya Medical Centre (UMMC) (MREC ID no.: 201754-5196).
Demographic and background characteristics
Demographic characteristics such as age, race, educational level, employment status and self-reported sexual orientation were assessed. Sexual orientation was categorized as homosexual (“gay”, “people like us”, “MSM”, “bisexual”) and non-homosexual (“straight” or “heterosexual”).
HIV testing behaviour and self-reported HIV status
Participants were asked if they had ever tested for HIV and those who had tested for HIV were asked to recall the date of last HIV testing and result of the HIV test.
Syndemic of psychosocial factors and phenomenon
A syndemic count was created by summing the number of psychosocial health conditions which include presence of depressive symptoms, suicidal risk, “chemsex”, history of CSA and IPV.
Depression
Depressive symptomatology was assessed by the Center for Epidemiological Studies – Depression (CESD) questionnaire. 22 This consists of 20 questions to assess the depressive symptoms that participants experienced in the past one week. Each item is scored from 0 to 3 (0 = rarely or none of the time, 1 = some or little of the time, 2 = moderately or much of the time and 3 = most or almost all the time). Questions 4, 8, 12 and 16 are reversed in valence. Scores for each item are summed to provide a total score. The scores ranged from 0 to 60 (Cronbach’s alpha coefficient 0.866). Scores over 16 were used to define major depressive symptoms20,23 with higher scores indicate more severe depressive symptoms.
Suicide risk
Suicidal risk was measured by Suicide Behaviours Questionnaire-Revised (SBQ-R). A total score of 7 and higher in the general population indicate significant risk of suicidal behaviour. 24
“Chemsex”
Participants were asked if they had ever used psychoactive substances (crystal meth/“Batu”/ice, ketamine, ecstasy, poppers and gamma hydroxybutyrate/gamma butyrolactone [GHB/GBL]) before or during anal intercourse. 25
Childhood sexual abuse
CSA was assessed by asking the participants whether they had sexual intercourse with someone when they were under 18 years old. Those who answered “yes” were then asked whether they were pressured, forced or intimidated into doing something sexually that they did not want to do, including fondling, oral sex, and anal penetration. All participants who answered “yes” to this follow-up question were classified as having experienced CSA. 12
Intimate partner violence
Participants were asked whether they had ever been hurt, hit, or slapped, by a steady or casual partner, being forced by a steady or casual partner to have sex, being forced by a person who was not a steady or casual partner to have sex, or being fondled or forced into unwanted sexual touching.
Condomless anal intercourse
Condomless anal intercourse (CAI) was defined as responding “never” and “sometimes” to the questions regarding frequency of condom use during anal intercourse with a male partner in the last three months.
Statistical analysis
Firstly, descriptive statistics, such as means, standard deviations (SD), frequencies, and percentages were used to report the demographic characteristics and history of HIV testing. Prevalence of the psychosocial factors, syndemic phenomenon and count were examined along with bivariate analysis among all the psychosocial health conditions.
Potential correlates of CAI and self-reported HIV infection were examined separately using logistic regression. Significant variables associated with CAI and self-reported HIV infection in the bivariate analysis was further examined in the multivariable analysis. All the significance levels were set at 0.05. Multicollinearity was assessed using variance inflation factor (VIF), to measure the inflation in the variances of the parameter estimates due to multicollinearity potentially caused by the correlated predictors. The cut-off point of VIF was set at 5. 26
Results
Participants’ socio-demographic characteristics
A total of 622 sexually active, Malaysian MSM completed all questions in the online survey. Only two of the participants self-identified as “heterosexual/straight” while the remaining identified as “gay”, “PLU (people like us), “MSM”, “homosexual” and “bisexual”. The mean age of participants was 28.2 years old (range: 18–64, standard deviation: 6.9 years). Those aged 25 to 39 years old accounted for 58.4% of participants. Most of the participants were from Kuala Lumpur and Selangor (67.4%). In terms of ethnicity, Malay was the majority (n = 415, 66.7%), followed by Chinese (n = 120, 19.3%), and Indian with other ethnic groups (n = 87, 14.0%). More than half of participants (54.5%) attained their education level at undergraduate level or above (Table 1).
Socio-demographic characteristics of the MSM.

With regards to HIV testing, only 383 (61.6%) had ever undergone HIV testing prior to participating the survey (ever tester). Among the ever testers, 93 (24.3%) of them self-reported to be HIV-positive and 88 (94.6%) of them were seeing a doctor for HIV care.
Prevalence of psychosocial health conditions
Of all participants, 60.8% scored 16 or more (≥16) on the CES-D, indicating presence of major depression symptoms while among the HIV-positive participants, 71.0% of them scored ≥16. Significant suicidal risk was present in 30.7% of all the participants, scoring SBQ-R of 7 or more (≥7) while it was 39.8% among the HIV participants. As for “chemsex”, it was reported in 22.5% of all the participants before or during anal intercourse. Among the HIV-positive participants, prevalence of “chemsex” was 38.7%. History of CSA was present in 12.4% of all the participants while it was present in 19.4% of the HIV-positive participants. As for IPV, the prevalence was 24.6% among all the participants while it was 21.5% in HIV-positive group. Overall, 46.0% of the participants had two or more (≥2) psychosocial conditions, or syndemics. The proportion of CAI among all participants was 54.3%.
Table 2 presents the unadjusted odds ratios (OR) of bivariate relationship between psychosocial factors, CAI during the last three months and HIV-positive status. The psychosocial conditions were significantly associated with each other and with CAI during the last three months and HIV status. For example, MSM who experienced major depressive symptoms were more likely to report significant suicidal risk (odds ratio [OR] 4.02, 95% confidence interval [CI]: 2.67–6.01), IPV (OR 2.18, 95% CI: 1.45–3.16), engaged in risky sex behaviour (CAI during the last three months) (OR 1.57, 95% CI: 1.14–2.17) and self-reported HIV-positive (OR 1.16, 95% CI: 1.01–2.78). Additionally, significant suicidal risk was also positively associated with “chemsex” (OR 1.71, 95% CI: 1.16–2.54), history of CSA (OR 1.84, 95% CI: 1.13–2.99), IPV (OR 2.71, 95% CI: 1.86–3.97) and HIV status (OR 1.67, 95% CI: 1.03–2.73). Men who experienced IPV as victims were also more likely to experience major depressive symptoms (OR 2.18, 95% CI: 1.45–3.46) and significant suicidal risk (OR 2.71, 95% CI: 1.86–3.97).
Bivariate associations between psychosocial health conditions, condomless anal intercourse during last three months and self-reported HIV-positive status among MSM.
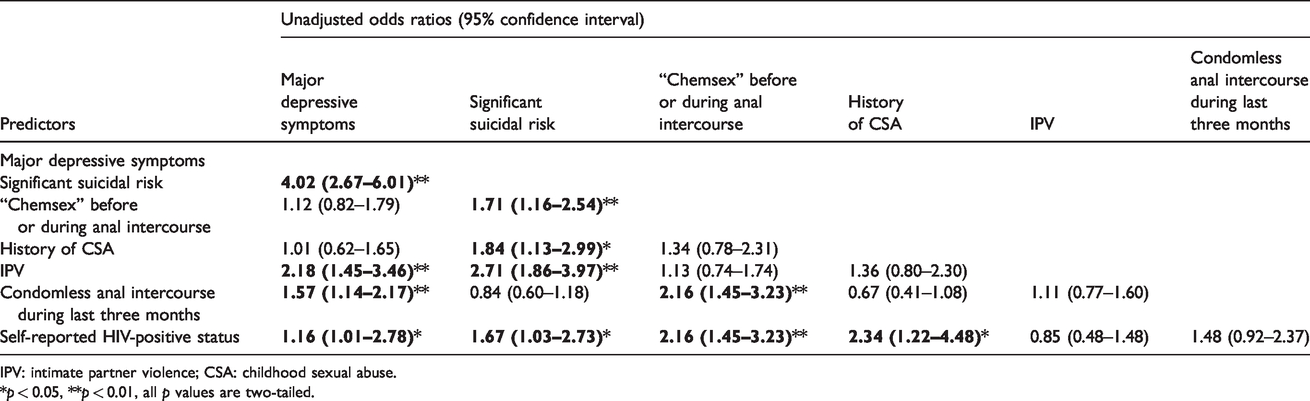
IPV: intimate partner violence; CSA: childhood sexual abuse.
*p < 0.05, **p < 0.01, all p values are two-tailed.
In terms of the analytic outcomes of the study, CAI during the last three month was associated with major depressive symptoms (OR 1.57, 95% CI: 1.14–2.17) and “chemsex” (OR 2.16, 95% CI: 1.45–3.23) while self-reported HIV status was associated with major depressive symptoms (OR 1.16, 95% CI 1.01–2.78), significant suicidal risk (OR 1.67, 95% CI: 1.03–2.73), “chemsex” (OR 2.16, 95% CI: 1.45–3.23) and history of CSA (OR 2.34, 95% CI: 1.22–4.48).
Multivariable analysis is presented below in Tables 3 and 4.
Correlates of CAI in the last three months.
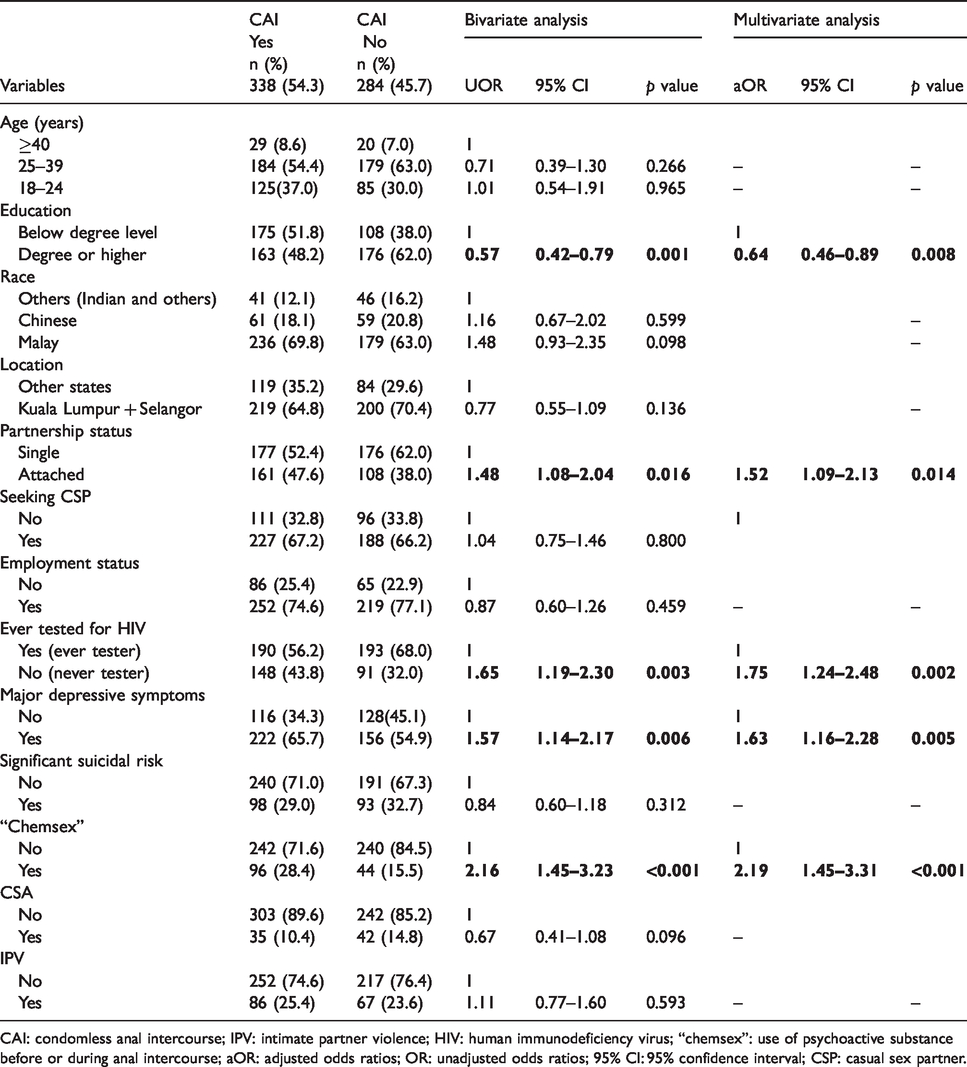
CAI: condomless anal intercourse; IPV: intimate partner violence; HIV: human immunodeficiency virus; “chemsex”: use of psychoactive substance before or during anal intercourse; aOR: adjusted odds ratios; OR: unadjusted odds ratios; 95% CI: 95% confidence interval; CSP: casual sex partner.
Correlates of self-reported HIV status among MSM.
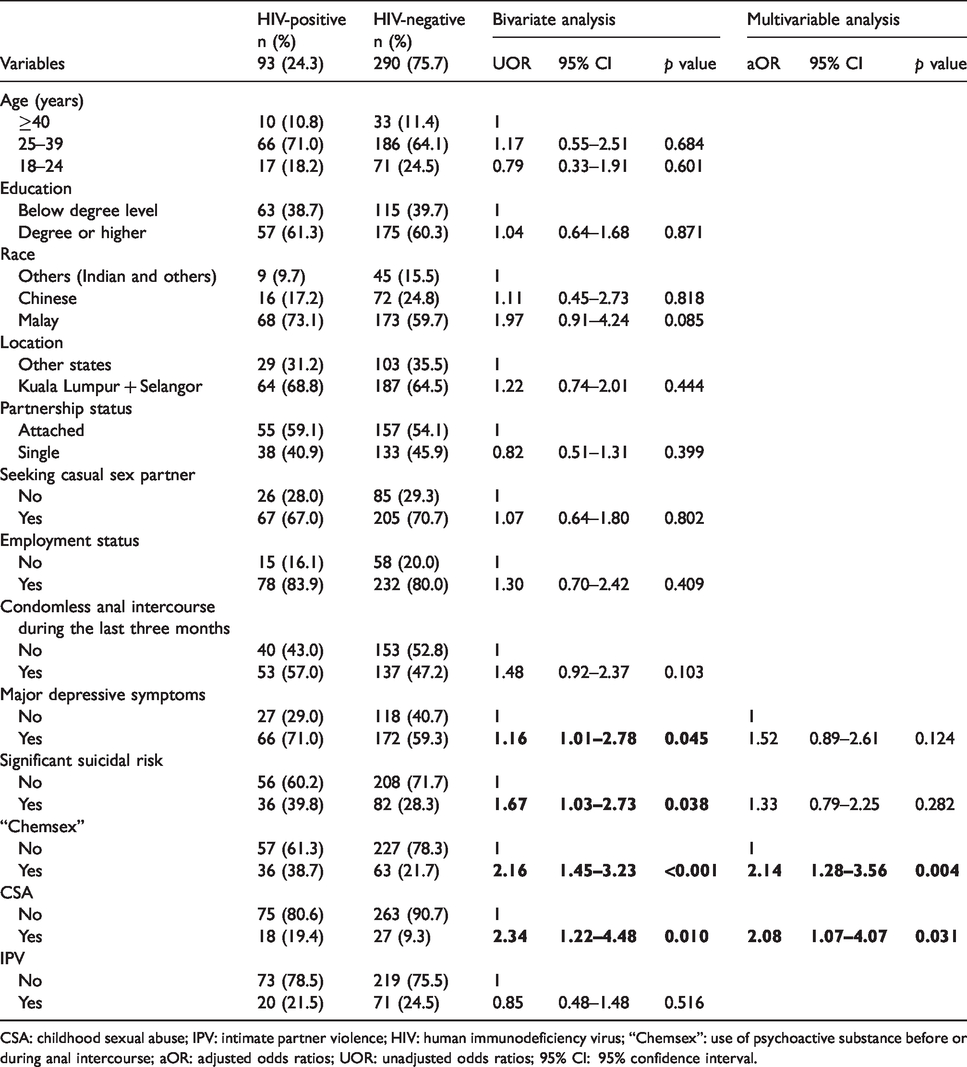
CSA: childhood sexual abuse; IPV: intimate partner violence; HIV: human immunodeficiency virus; “Chemsex”: use of psychoactive substance before or during anal intercourse; aOR: adjusted odds ratios; UOR: unadjusted odds ratios; 95% CI: 95% confidence interval.
Association between socio-demographic characteristics and psychosocial health conditions with CAI
Table 3 shows the correlates of CAI during the last three months among 54.3% of the MSM in this online survey.
From the bivariate analysis, those with higher educational background (above degree level) were less likely to be having condomless sex during anal intercourse (OR 0.57, 95% CI: 0.42–0.79). Meanwhile, those who were in partnership were more likely to engage in CAI (OR 1.48, 95% CI: 1.08–2.04). Besides, those who were never tested for HIV (“never testers”) was associated with CAI (OR 1.65, 95% CI: 1.19–2.30). As for the psychosocial health conditions, participants who reported major depressive symptoms (OR 1.57, 95% CI: 1.14–2.17) and “chemsex” (OR 2.16, 95% CI: 1.45–3.23) were significantly more likely to report CAI (see Table 3).
To determine the relative importance of socio-demographic factors and psycho-social factors, multivariate logistic regression analysis was conducted. Higher education was significantly associated with reduced odds of CAI (adjusted odds ratio [aOR] 0.64, 95% CI: 0.46–0.89) while being attached in a steady relationship (aOR 1.52, 95% CI 1.09–2.13), never testers (aOR 1.75, 95% CI: 1.24–2.48), presence of major depression symptoms (aOR 1.63, 95% CI: 1.16–2.28) and “chemsex” (aOR 2.19, 95% CI: 1.45–3.31) significantly increased the odds of CAI. Presence of major depressive symptoms and “chemsex” were significantly associated with CAI (see Table 3).
Association between socio-demographic characteristics and psychosocial health conditions with self-reported HIV status
Table 4 shows the correlates of self-reported HIV status among the MSM who had ever tested for HIV. HIV-positive status was reported among 93 participants (24.3%).
From the bivariate analysis, participants whom experienced major depressive symptoms (OR 1.16, 95% CI: 1.01–2.78), significant suicidal risk (OR 1.67, 95% CI: 1.03–2.73), “chemsex” (OR 2.16, 95% CI: 1.45–3.23) and history of CSA (OR 2.34, 95% CI 1.22–4.48) were significantly associated with HIV-positive status.
Multivariate logistic regression analysis was then conducted. Engaging in “chemsex” (aOR 2.14, 95% CI: 1.28–3.56) and history of CSA (aOR 2.08, 95% CI: 1.06–4.07) were significantly associated with increased odds of HIV-positive status.
Furthermore, increasing number of syndemic (psychosocial health conditions) was significantly associated with HIV-positive status (see Table 5). Participants with 1, 2, 3, 4 or more psychosocial health conditions were significantly more likely to be HIV infected than those without psychosocial health conditions (OR 3.39, 95% CI: 1.41–8.14; OR 3.51, 95% CI: 1.43–8.61; OR 4.22, 95% CI: 1.68–10.96 and OR 7.58, 95% CI: 2.44–23.55, respectively).
Correlates of syndemic counts, condomless anal intercourse (CAI) and self-reported HIV status among MSM.

*p < 0.01, **p < 0.001, all p values are two-tailed.
OR: odds ratio; 95% CI: 95% confidence interval; CAI: condomless anal intercourse.
Discussion
The present study identified the co-occurrence or clustering of psychosocial conditions among Malaysian MSM, suggesting a syndemic effect. These findings were consistent with previous studies among MSM in USA,10,12 China,4,15 Taiwan, 16 India,17,18 Vietnam 19 and Thailand. 20 Results of the present study revealed that overlapping psychosocial conditions compound and increase an individual’s risk for HIV acquisition. Therefore, it is the synergistic interplay of the health conditions that magnify the HIV transmission.11,15,20
Almost two-thirds of men in this study experienced major depressive symptoms. The prevalence of depression in the general population in Malaysia ranges between 3.9 to 46.0%.27–29 Currently, there is a lack of attention on depression among male populations in Malaysia, 28 and even less, within the MSM populations. Reasons for the high prevalence of significant major depressive symptoms among MSM could be due to society’s homophobia, stigmatization, gay-related and sexual orientation-based victimization plus internalized homophobia faced by MSM. 30 Having clinically depressive symptoms was also associated with CAI and HIV infection in this study. Apathy and negative self-valuation associated with depression might have led to reduced personal motivation to engage in safe sex. 19
We also found that significant suicidal risk was positively associated with having major depressive symptoms, history of CSA and IPV in the bivariate analysis (see Table 2). Depression leading to self-harm is well established. 31 Based on the National Suicide Registry of Malaysia in 2009, there were 328 cases of suicide deaths reported in 2009; suicide rate of 1.18/100,000 population. 32 The suicide risk for MSM was six times higher than heterosexual men 33 and was result of a combination of discrimination, victimization, experience of homophobia and violence. The findings in our study is comparable to a Thai study, with rate of 27.6% among their MSM cohort. 20 Suicidal risk has been associated with IPV as MSM generally experienced higher rates of violence than the heterosexual population. 34
In this study, ever having “chemsex” was associated with CAI in the past three months and being HIV-positive. The use of psychoactive drugs such as methamphetamines can have physiological effects, facilitating HIV transmission via prolongation of sex or trauma to the anus or rectum. 35 The heightened sexual arousal and sexual disinhibition during “chemsex” may impair decision-making ability to use condoms. Health care providers should be trained to recognise the symptoms of substance use disorders and refer MSM with problematic use to psychiatric services. More integrated services that tackle sexual health and mental health issues are needed.
History of CSA was present among 12.4% of study participants, while globally this prevalence among MSM ranges from 1% to 32%. 36 MSM who experienced CSA usually do not realize the features of abuse during childhood and the inequality of power dynamics between them and older adults or superiors. 17 Even when they reach adulthood, some victims may develop a sense of remorse, that they have to take responsibility for the abuse because they were sought out by the perpetrators for being gay. 17 Therefore, the survivors may internalise the stigma as they continue to explore their sexuality in the conservative society where homosexuality is not generally accepted. CSA survivors are often related to participation in sex work which in turn increases the risk of HIV. 37 Therefore, education on CSA to children and family is an essential part of HIV prevention. Health care providers need to be vigilant in screening CSA and provide mental health care to the survivors.
As for IPV, the prevalence was 24.6% among all the participants. The estimated prevalence for victims of any form of IPV among MSM ranges from 32% 38 to 78%. 39 There is significant intersection between IPV, major depressive symptoms and significant suicidal risk. 40 MSM may fear partner violence in negotiating for the use of condoms while having sex with casual or regular male partners and disclosure of HIV status. 40 They may experience difficulties in accessing health services especially when they attempt to hide their MSM or HIV status for fear of IPV from the partner.
In examining the syndemics of psychosocial conditions in the context of MSM within South East Asian countries, positive associations with the outcome of CAI and HIV infections have been documented. For example, Biello et al. examined this association among MSM sex workers in Vietnam and found that for every increasing unit of syndemic conditions (depressive symptoms, alcohol dependence, CSA, illicit drug use at any time and sexual violence), there was a 25–30% increase in odds of CAI, which subsequently increased their risks for HIV infection. 19 Similarly, Guadamuz et al. found that increasing number of psychosocial factors were associated with increasing HIV prevalence and HIV incidence in a cohort of Thai MSM. HIV prevalence was 33.2% among MSM with four to five conditions (suicidal ideation, social isolation, alcohol, club drugs, selling sex and forced sex) but the HIV prevalence was 23.7% in men with one to three conditions and 15.3% in men without any psychosocial conditions. 20 Therefore, findings from the present study were consistent with the findings from previous studies.
Several limitations of the study ought to be acknowledged. Firstly, the recruitment of the participants comprised a convenience sample of MSM who used gay social media or MSM seeking/receiving the services of those social media. Online surveys may over-sample those who are more socially connected online. Hence, generalizing the results to a more diverse MSM population in Malaysia should be interpreted with caution and the true prevalence of psychosocial health conditions and syndemic phenomena may be underestimated. In this online survey, biospecimens were not collected for serologic testing to confirm the self-reported HIV test results; thus, participants who were unaware of their status and HIV prevalence may be under-reported.
Additionally, the assessment period of self-reported CAI and psychosocial conditions varied and temporality of these variables cannot be established. For example, the presence of major depressive symptoms was assessed for the past one week while CAI was assessed in the past three months. Apart from that, some variables were measured as single items such as “chemsex”, history of CSA and IPV. Next, CAI was not controlled for type of sexual partners, namely primary and casual sex partners. Furthermore, the cross-sectional study design of the present study limits our ability to infer the directionality of studied variables and establish causality of syndemics and HIV infection.
As this was an online survey, the response rate was low compared to non-online surveys. 41 However, the non-response rate was comparable to those of other online surveys of MSM which typically range from 15% to 20%.42,43 Nevertheless, internet-based methods may reach high-risk, hard-to-reach populations like MSM. Within the context of criminalization and stigmatization of MSM in Malaysia, internet-based recruitment may be more feasible than venue-based recruitment. Additionally, the perceived privacy of the online space may also yield more accurate, honest responses compared to face-to-face interviews.42,44 Lastly, our study did not use more complex statistical analyses to empirically test the syndemic effect of psychosocial conditions on HIV infection as has recently been shown. 45 Nevertheless, our findings strongly suggest co-occurrence of psychosocial conditions.
Conclusion
In conclusion, multiple co-occurring psychosocial health conditions among MSM were associated with risky sexual behaviour and HIV infection among MSM in Malaysia. The prevalence of psychosocial health conditions was high in sample and there was a significant additive dose response between the number of syndemic factors and HIV infection. Comprehensive HIV prevention strategies should include mental health care to address the co-occurring psychosocial conditions in a holistic manner in order to end AIDS by 2030.
Medical health care providers should be more vigilant in screening psychosocial conditions in their clinical practice and assist patients in coping with appropriate psychotherapy services. These interventions should be targeted at individual, social network, community and structural levels. Anal sex between men is criminalized by civil law and Sharia law in Malaysia. Recently, five Malay-Muslim MSM were convicted by Shariah law and were fined, caned, and imprisoned for having sex at a private residence. 46 The Prime Minister and religious authorities have repeatedly denounced LGBT people.47,48 Therefore, homophobia at the structural level has produced a disabling environment for MSM to disclose their behaviours and seek health services. 49 Future research agendas should explore structural interventions, as well as psychosocial interventions such as development of positive coping skills and promoting social support to address the co-occurring psychosocial conditions in this vulnerable population.
Footnotes
Acknowledgements
The authors thank the staff members of the Center of Excellence for Research in AIDS (CERiA), Pink Triangle (PT) Foundation, Kuala Lumpur AIDS Support and Services (KLASS) for their support in data collection.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was funded by World Bank. However, the funder has no role in the study design, data collection and analysis and preparation of this research.