
Abstract
Few studies investigate sexual health among Chinese international students in Australia. We recruited domestic (n = 623) and Chinese international (n = 500) students for separate online surveys on sexual behaviours and knowledge. Samples were compared using Chi square, Fisher’s exact and equality of medians tests. Domestic students were more likely than international students to have ever touched a partner’s genitals (81% vs. 53%, p < 0.01), had oral sex (76% vs. 44%, p < 0.01), vaginal intercourse (67% vs. 41%, p < 0.01) and anal intercourse (31% vs. 6%, p < 0.01). Domestic students were younger when they first touched a partner’s genitals (16 vs. 18 years, p < 0.01), had oral sex (17 vs. 18 years, p < 0.01) and vaginal intercourse (17 vs. 18 years, p < 0.01). Domestic students were less likely than Chinese international students to report only one lifetime partner for touching genitals (22% vs. 50%, p < 0.01), oral sex (25% vs. 55%, p < 0.01), vaginal intercourse (30% vs. 58%, p < 0.01) and anal intercourse (54% vs. 88%, p < 0.01). Domestic students were more likely than Chinese international students to use the oral contraceptive pill (48% vs. 16%, p < 0.01) and long-acting reversible contraceptives (19% vs. 1%, p < 0.01). Domestic students scored higher than international students on a contraception and chlamydia quiz (4/5 vs. 2/5, p < 0.01). Domestic and Chinese international students differed in sexual behaviours and knowledge highlighting the need for relevant sexual health promotion for both groups.
Introduction
Australian sexual health service providers have raised concerns around the rise of unintended pregnancy, sexual assault and sexually transmissible infections (STIs) among international students.1,2 This is consistent with Australia’s latest National human immunodeficiency virus (HIV) and STI strategies that identify mobile populations, young people and culturally and linguistically diverse groups as priority populations for reducing STI incidence.3,4 In 2018, there were over 690,000 international students in Australia, of which students from the People’s Republic of China were the largest group (30%). 5
Studying abroad allows some Chinese international students to explore non-marital intimate relationships and other forms of non-normative intimacy. 6 Past studies have highlighted the limited sexual and reproductive health knowledge among international students, particularly those from Asia.7,8 Barriers to accessing sexual health services include cultural sensitivities related to sexual behaviours, 9 language barriers and navigating unfamiliar health systems.2,8 There can also be financial barriers, with many international students having limited understanding of their Overseas Student Health Cover policies which they must purchase for basic medical costs.2,10
Although numerous studies explore sexual health outcomes of students in Australia,11–13 these are generally administered in English only. 14 Previous research suggests Chinese international students sometimes could not recognise sexual health terms in English (e.g. cervix, human papillomavirus [HPV]). 15 Capturing data on sexual health outcomes from Chinese international students in Chinese is essential to inform appropriate sexual health promotion. This study aims to describe key sexual health knowledge and behaviour indicators of Chinese international students and compare with those of domestic students.
Methods
Two comparable surveys were administered to their respective populations in the appropriate language at the same time using culturally-specific online recruitment strategies.
Sex, drugs and rock ‘n’ roll survey
Between March and April 2018, the Burnet Institute conducted the annual sex, drugs and rock ‘n’ roll (SDRR) survey of young people aged 15–29 years.16,17 Participants from the general population were recruited through emails to past participants, paid advertising and sharing on social media. Participants completed the anonymous survey in English which captured information on socio-demographic characteristics, sexual behaviours and knowledge, and alcohol and other drug use. Data were collected and managed using the secure web-based application REDCap and hosted at the Burnet Institute. 18 Participants viewed the participant information and consent form online and checked an electronic box to provide informed consent. Participants who pressed submit at the end of the survey were considered complete responses and included in the analysis. Participants could provide their email through a non-linked form and enter the draw to win a $250 voucher. The Alfred Hospital Human Research Ethics Committee approved the study (326/08).
Intimate attitudes, practices and knowledges survey
The intimate attitudes, practices and knowledges (IAPK) survey was developed based on items from the SDRR survey and modified to include culturally appropriate and additional questions relevant for Chinese students. The IAPK survey was developed in English and translated by bilingual author CQ into standard modern written Chinese. Four Chinese international students tested the survey for usability and provided feedback on layout, wording and cultural sensitivities. Between March and May 2018, authors FM, CQ and their contacts promoted the survey through Chinese student groups and WeChat, a social media platform popular among Chinese communities in Australia. 19 Participants were eligible if they were aged 16 years and older, an international student in Australia and able to complete the survey in Chinese. Participants indicated informed consent by checking an electronic box. Data were collected and managed using REDCap and hosted at the Burnet Institute. Participants who submitted their survey are included in analysis. Upon completion, participants could enter the draw to win one of four $100 vouchers. The University of Melbourne Human Research Ethics Committee approved the study (1749805).
Main measures
Socio-demographic characteristics: Both surveys recorded participants’ gender, age and current education.
SDRR: Participants reported their current gender identity (male, female, trans male, trans female, non-binary or a space to record any gender not listed), month and year of birth which were used to generate age and current education level (year 10 or lower, year 11, year 12, TAFE/college or diploma, university undergraduate, university postgraduate). Participants reported their country of birth; those who did not select Australia were asked their residency status (permanent resident/Australian citizen, working holiday, temporary resident, international student or I don’t wish to say). Domestic students were defined as participants who identified they were currently studying and were not international students, temporary residents or on a working holiday. IAPK: Participants reported their gender (male, female or other, with space to specify genders not listed), year of birth and current education level in Australia (high school, English college, Vocational Education and Training [VET], TAFE, university undergraduate, masters by coursework, masters by research, PhD or other). Responses were recoded to high school or post-high school for binary comparison. Chinese international students reported their country and territory of origin, length of time spent in Australia, whether they had ever received school-based sex education and whether this occurred within Australia, outside Australia or both.
Knowledge of chlamydia and contraception: Both surveys contained five statements to measure knowledge of chlamydia and contraception. Participants selected if statements were ‘true’, ‘false’, ‘I don’t know’ or ‘I don’t wish to say’. Responses ‘I don’t know’ and ‘I don’t wish to say’ were coded as incorrect to enable binary comparisons. Participants’ correct answers were added to generate a median score out of five. Items included:
Chlamydia can be diagnosed by a urine test (true) Left untreated chlamydia can last for years (true) People infected with STIs almost always have some symptoms (false) Chlamydia can make women infertile (true) Using contraception like the pill, intrauterine device or implant when you are young reduces your future fertility (chance of getting pregnant) (false).
Sexual behaviours: In both surveys, participants reported the age they first touched a partner’s genitals with their hands, gave or received oral sex, had vaginal intercourse and had anal intercourse. We created binary variables indicating whether participants ever engaged in each behaviour. Participants selected their number of lifetime partners (selecting from 1, 2–3, 4–5, 6–10, 21–50, over 50; recoded to 1, 2 to 5, 6 or more) and partners in the past year for each behaviour (none, 1, 2–3, 4–5, 6–10, 21–50, over 50; recoded to none, 1, 2 or more); these categories were selected because having multiple partners (i.e. more than one sexual partner) in a year is associated with higher rates of STIs.20,21 Participants who had ever had vaginal or anal intercourse reported how often they used condoms with regular and casual sex partners in the past year (always, usually, sometimes or never; recoded to always or not always). In SDRR, regular partner was defined as boyfriend/girlfriend/in a relationship and casual partner as one-night stand, friends with benefits, just seeing someone or fuck buddy. In IAPK, regular partner was defined as boyfriend or girlfriend and casual partner as ‘hook-up’. Participants also selected which forms(s) of contraception they used the last time they had vaginal intercourse (condoms, oral contraceptive pill, injection, implant, intrauterine device, morning after pill, withdrawal or none). For analysis, we grouped injections, implants and intrauterine devices as long-acting reversible contraceptives (LARCs).
STI testing among participants who reported vaginal or anal intercourse: In the SDRR survey, participants reported when they last had an STI test (never, 0–3 months, 4–6 months, 7–12 months, 1–2 years or more than two years ago). Responses were recoded to ‘ever had an STI test’ (yes/no). In the IAPK survey, participants indicated if they had ever been tested for any STI by a doctor or health worker in Australia (yes/no).
Sexual health information (Chinese international students only): Participants reported whether they believed it would be beneficial for them to receive targeted sexual health information for international students (yes/no/not sure). Participants stated what information should be available and how it should be provided (open text responses).
Data analysis
Data were analysed using Stata version 15 (StataCorp. 2017. Stata Statistical Software: Release 15, StataCorp LLC, College Station, TX). We used percentages to present categorical variables and medians for continuous variables. We used Chi square tests to compare categorical variables between domestic and Chinese international students and Fisher’s exact test where cell sizes were less than five. We compared continuous variables using an equality of medians test. We did not compare STI testing due to different items used between surveys. Gender comparisons only included males and females as other genders were not listed in the IAPK survey; however, participants of other genders were included in all other descriptive analyses. From SDRR, we excluded participants who were not currently studying, international students, temporary residents, those on a working holiday and 15-year-olds. From IAPK, we excluded graduates and participants from territories other than mainland China (e.g. Singapore, Taiwan and Honk Kong).
We used content analysis to code free-text responses related to sexual health information preferences. Responses were independently coded by authors CHD and CQ with discrepancies resolved through discussion.
Results
Survey responses
In the SDRR study, 1461 people provided consent and 1007 submitted the survey (69%). We excluded those who were not currently studying (n = 335), international students (n = 20), temporary residents (n = 3), those on a working holiday (n = 1) and 15-year-olds (n = 25). In the IAPK study, 1071 people provided consent and 543 submitted the survey (51%). We excluded IAPK participants who were aged 30 years and over (n = 18), graduated (n = 6) and from territories and countries other than mainland China (n = 19). The results describe survey responses from 623 domestic students and 500 Chinese international students.
Socio-demographic characteristics
Domestic students and Chinese international students had similar age and gender profiles (Table 1). However, domestic students were more likely than international students to be studying at high school (14% vs. 4%, p < 0.01). Of the Chinese international students, 51% had been in Australia for one year or more and 33% reported no sex education.
Socio-demographic characteristics among domestic and Chinese international students.
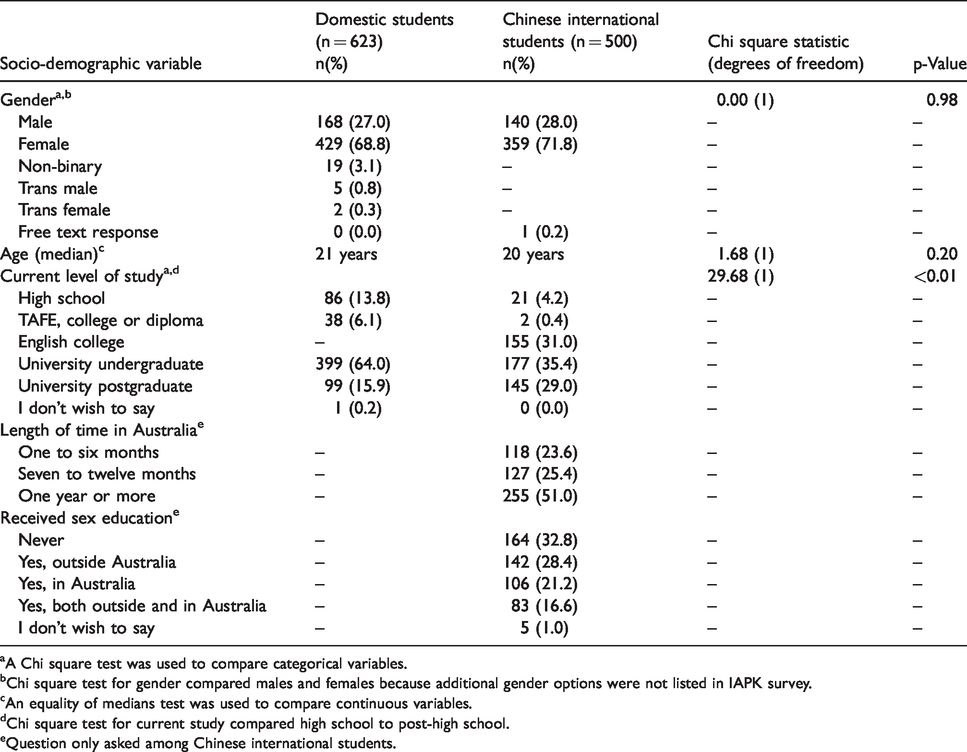
aA Chi square test was used to compare categorical variables.
bChi square test for gender compared males and females because additional gender options were not listed in IAPK survey.
cAn equality of medians test was used to compare continuous variables.
dChi square test for current study compared high school to post-high school.
eQuestion only asked among Chinese international students.
Knowledge of chlamydia and contraception
Domestic students scored significantly higher on the knowledge quiz compared to Chinese international students (4/5 vs. 2/5, p < 0.01). For each item, domestic students were more likely to select the correct answer than international students (Table 2). The largest difference was in response to ‘chlamydia can make women infertile’ where 63% of domestic students and 23% of Chinese international students selected the correct answer (p < 0.01).
Chlamydia and contraception knowledge among domestic and Chinese international students.
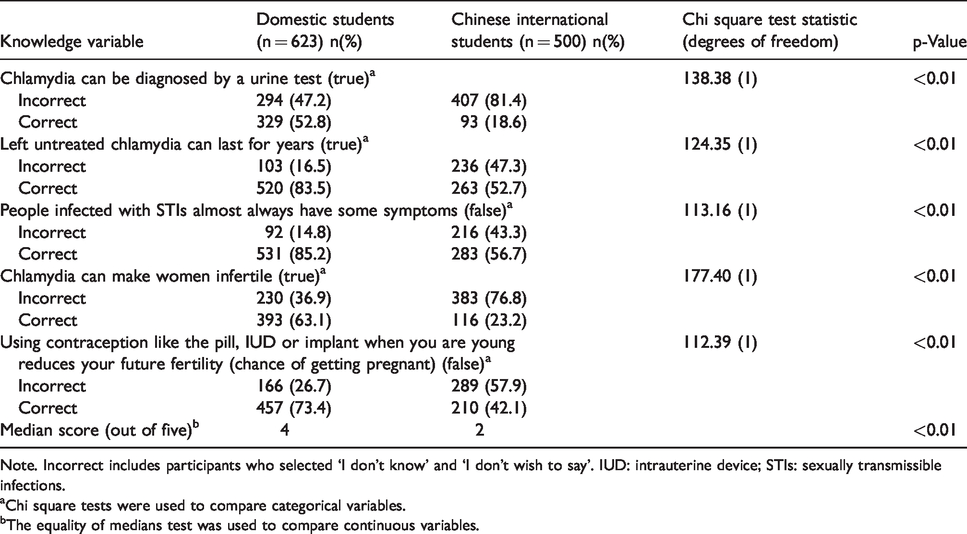
Note. Incorrect includes participants who selected ‘I don’t know’ and ‘I don’t wish to say’. IUD: intrauterine device; STIs: sexually transmissible infections.
aChi square tests were used to compare categorical variables.
bThe equality of medians test was used to compare continuous variables.
Sexual behaviours
Domestic students were more likely than Chinese international students to report ever touching a partner’s genitals with their hands (81% vs. 53%, p < 0.01), having oral sex (76% vs. 44%, p < 0.01), vaginal intercourse (67% vs. 41%, p < 0.01) and anal intercourse (31% vs. 6%, p < 0.01). Domestic students were significantly younger the first time they touched a partner’s genitals (16 years vs. 18 years, p < 0.01), gave or received oral sex (17 years vs. 18 years, p < 0.01) and had vaginal intercourse (17 years vs. 18 years, p < 0.01). There was no significant difference between domestic and international students for age reported at first anal intercourse (p = 0.31) (Table 3).
Sexual behaviours among domestic and Chinese international students.

Note: Percentages may not add up to 100% due to rounding. Participants who did not answer are not included in Chi square, Fisher’s exact or equality of medians tests.
aChi square tests were used to compare categorical variables.
bThe equality of medians test was used to compare continuous variables.
cAmong participants who reported they had ever done this behaviour.
dFisher’s exact tests were used to compare categorical variables with cell sizes less than five.
Domestic students were more likely than international students to report six or more lifetime partners and two or more partners in the past 12 months for touching genitals, oral sex and vaginal intercourse. For example, 37% of domestic students who had ever had vaginal intercourse reported having two or more vaginal partners in the past year compared to 19% of Chinese international students (p < 0.01). There was no significant difference between domestic and Chinese international students for the number of anal partners reported in the past 12 months (p = 0.60).
Condom and contraception use
Domestic students were less likely than Chinese international students to always use condoms with regular partners (22% vs. 61%, p < 0.01). More domestic students reported having a casual partner in the past 12 months than international students (41% vs. 21%, p < 0.01). Thirty-nine percent of domestic students and 64% of international students always used condoms with casual partners in the past 12 months (p < 0.01).
At last vaginal intercourse, domestic students were more likely than Chinese international students to report using the oral contraceptive pill (48% vs. 16%, p < 0.01) and LARCs (19% vs. 1%, p < 0.01). International students were more likely to use condoms (84% vs. 46%, p < 0.01) and emergency contraception (7% vs. 2%, p < 0.01) than domestic students at last vaginal intercourse. There were no significant differences observed between student type and reporting no contraception or withdrawal at last vaginal intercourse (Table 4).
Condom and contraception use among domestic and Chinese international students.
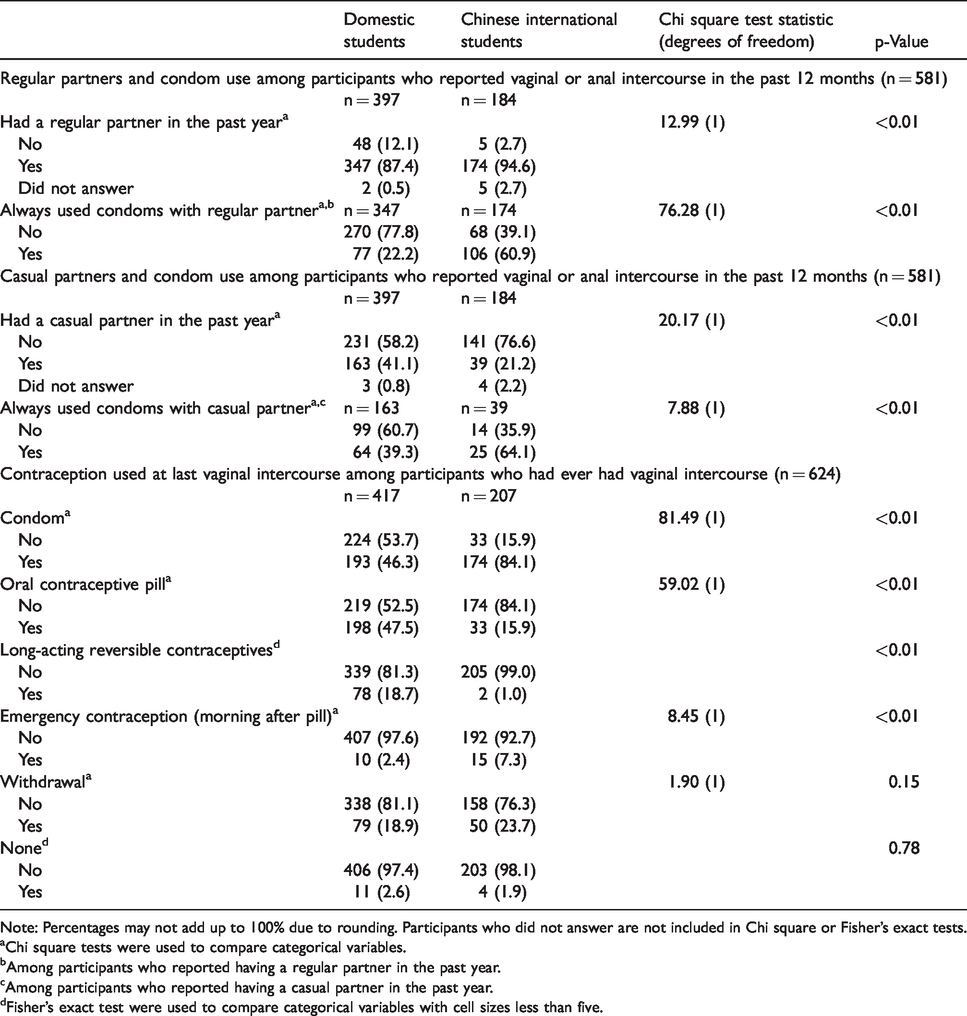
Note: Percentages may not add up to 100% due to rounding. Participants who did not answer are not included in Chi square or Fisher’s exact tests.
aChi square tests were used to compare categorical variables.
bAmong participants who reported having a regular partner in the past year.
cAmong participants who reported having a casual partner in the past year.
dFisher’s exact test were used to compare categorical variables with cell sizes less than five.
STI testing
Of domestic students who had ever had vaginal or anal intercourse (n = 431), 50% reported that they had ever had an STI test. Among international students who had ever had vaginal or anal intercourse (n = 211), 8% reported having an STI test in Australia.
Sexual health information: Chinese international students only
Among Chinese international students, 48% (n = 242) believed they would benefit from targeted sexual health information. Seventy-nine participants provided an open-text response for the information they thought should be provided. Common suggestions included information about: preventing STIs (n = 32), contraception (n = 17), general sexual health (n = 11), unplanned pregnancies (n = 8) and STI testing (n = 8). Some participants were interested in information about masturbation, sexual enjoyment and HPV vaccine. Eighty participants suggested how sexual health information should be provided including email (n = 25), internet (n = 18), WeChat (n = 15), online lectures/seminars (n = 13), printed material (n = 13) and university or health services (n = 10).
Discussion
Our results indicate that there were significant differences in sexual behaviours, knowledge, condom and contraception use between domestic and Chinese international students. Chinese international students were less likely to report risky sexual behaviours compared to domestic students. However, Chinese international students had significant gaps in sexual health knowledge and low rates of sexual education. Literature shows that mobility can facilitate opportunity for changes in sexual behaviours. 22 Possible sexual mixing 23 with Australian-born students who demonstrate riskier sexual behaviours could potentially lead to poor sexual health outcomes for Chinese international students if they do not have the knowledge and experience to reduce their risk.
Other studies have also found Chinese students were less likely than Australian students to participate in risky sexual behaviours7,24 and more likely to delay sexual activity. 25 This may partly be explained by cultural norms surrounding sexual activity. For example, qualitative studies have reported that many international students (particularly females) fear judgment for pre-marital sexual activity6,8 despite casual sexual relationships becoming increasingly normalised in urban China.26,27
In our study, Chinese international students were significantly less likely than domestic students to use the oral contraceptive pill and LARCs and more likely to use less effective contraception (e.g. condoms and emergency contraception). Cultural norms may play a role here as well; for example, in China, LARCs are viewed as a contraception method for older people who already have children rather than younger people. 28 Future work exploring culturally appropriate methods to improve longer term contraception use among Chinese international students in Australia would be beneficial.
The distinct differences in sexual behaviours and contraception use found between the two populations highlights the need to ensure sexual health programmes meet the needs of both domestic and international students. Past research with university students in Australia showed groups had different preferences for sexual health promotion based on their level of STI risk. 29 A common barrier of youth-focused sexual health promotion programmes and resources is that they lack cultural sensitivity. 30 Language can be a barrier because some sexual health terms do not translate easily from English into Chinese. 15 Some international students may have privacy concerns if they are seen attending a sexual health service8,31 or social events that promote sexual health. 29 It is essential to give all students the opportunity to access culturally relevant resources and services to enable them to make informed decisions about their sexual health.
In 2016, China announced that sex education would be a requirement in middle- and high schools to address increased HIV incidence among young people. 32 However, our findings suggest that a significant proportion of Chinese international students arrive in Australia without any sexual education. Participants of IAKP were interested in receiving information focused on contraception and preventing STIs and suggested email, WeChat and online lectures as preferred communication channels. Schools and universities are in excellent positions to deliver such information with access to international students through online learning systems, lectures and classrooms. 33 Technology-based interventions (including text messages and emails) have shown some success among young people in Australia 34 and similar interventions could be adapted for domestic and Chinese international students. Future campaigns should be designed and evaluated in close consultation with students to ensure content and dissemination methods are appropriate.
Limitations
This study has several limitations. Although both surveys had similar questions, there may be subtle differences in meaning or connotation due to translation. However, administering the IAPK survey in Chinese allowed students to participate in a language other than English. The SDRR survey had a higher completion rate than the IAPK survey. We were unable to calculate the response rate to each survey due to multiple online recruitment methods. Selection bias may have occurred where more conservative Chinese international students may not have participated due to the sensitive nature of sexual health. Those interested in sexual health were also more likely to participate. Both online surveys used convenience sampling through social media, thus participants are unlikely to be representative of the population and results should not be generalised to all domestic and Chinese international students in Australia. 35 Differences between domestic and international students may be confounded by other variables such as education; however, age and gender profiles were similar. Data were self-reported and potentially influenced by social desirability bias, despite the anonymity. We did not test reliability or validity; however, each survey contained measures from psychometrically-validated scales, novel researcher-derived questions and multiple questions consistently asked in the SDRR survey over the past 14 years. We only captured participants’ knowledge of chlamydia but not other STIs or HIV.
Conclusion
Our study showed that Chinese international students demonstrated fewer sexual risk behaviours than domestic students and therefore may not relate to interventions targeted at students who have multiple sexual partners who do not always use condoms. It is important to develop sexual health promotion that is relevant to the needs, beliefs and behaviours of the target population. Universities and sexual health promotion organisations should work closely with domestic and Chinese international students to ensure services, events and resources promoting sexual health are appropriate for different student groups.
Footnotes
Acknowledgements
The authors gratefully acknowledge the students who provided feedback on the survey and the participants for their time.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: FM is supported by an Australian Research Council Future Fellowship (FT140100222), CHD through an Australian Government Research Training Program Scholarship and YX through a Melbourne Research Scholarship.