
Abstract
Condylomata acuminata (genital warts) have been identified in transgender women after gender affirmation surgery. We describe a case of a 57-year-old transgender woman with biopsy-proven neovaginal condylomata acuminata following gender-affirmation vaginoplasty using the penile skin inversion technique. The patient was successfully treated with trichloroacetic acid. To our knowledge, this is the first case report demonstrating successful treatment of neovaginal condyloma with trichloroacetic acid. We provide a review of the relevant literature and highlight the evidence for the clinical utility of trichloroacetic acid in transgender women with condyloma of the neovagina.
Keywords
Introduction
Condylomata acuminata caused by human papillomavirus (HPV) are the most commonly acquired sexually transmitted infection (STI). 1 Transgender women have higher rates of STIs than the general population. 2 Data also suggest that HPV burden among transgender women is high, with HPV DNA detection between 80 and 97% in recent studies.3–5 Anogenital warts have been reported in transgender women after gender affirmation surgery (GAS), specifically when penile skin is used for construction of female genitalia. The penile and scrotal tissues utilized in GAS are associated with the highest rates of HPV infection among cisgender men. 6 Whether neovaginal warts arise from grafting of previously infected skin or from contact of the neovagina with HPV through coitus is undetermined.
Treatment recommendations for neovaginal warts have not been well described. Here we report a case of a transgender woman diagnosed with warts of the neovagina, one year following GAS with penile inversion vaginoplasty, who had a complete response to treatment with trichloroacetic acid (TCA).
Case report
A 57-year-old transgender woman presented with biopsy-proven warts of the neovagina. She noted vaginal bleeding and initially presented to another provider, who performed biopsies of friable neovaginal lesions, and referred her to our practice. Histopathology revealed benign condylomata acuminata. Workup for other STIs and vaginal pathologies, including N. gonorrhoeae, C. trachomatis, T. vaginalis, C. albicans, and bacterial vaginosis, was negative. The patient’s medical history was only significant for gender dysphoria, which was managed with cross-sex hormone therapy, facial feminization surgery, and GAS with penile-skin inversion vaginoplasty. GAS was performed one year prior to the onset of symptoms. This procedure involved orchiectomy followed by creation of a neovagina by inverting penile skin into the dissected fascial space between the bladder and rectum with subsequent tissue rearrangement to create feminine external genitalia. 7 The patient was sexually active prior to GAS but did not report any high-risk behaviors such as survival sex work or drug use. At presentation, she reported a monogamous sexual relationship with her cisgender female partner. Details of their sexual relationship, including methods of intercourse, were not obtained.
Speculum examination revealed copious, nearly confluent verrucous lesions along the apex and the right wall of the neovagina (Figure 1). The apical location of the warts within the neovaginal vault precluded the use of patient-administered imiquimod or podophyllotoxin treatment. Cryotherapy, another minimally invasive option, was not readily available in our clinic. Given her extensive surgical history throughout her gender transition, the patient declined surgical resection.
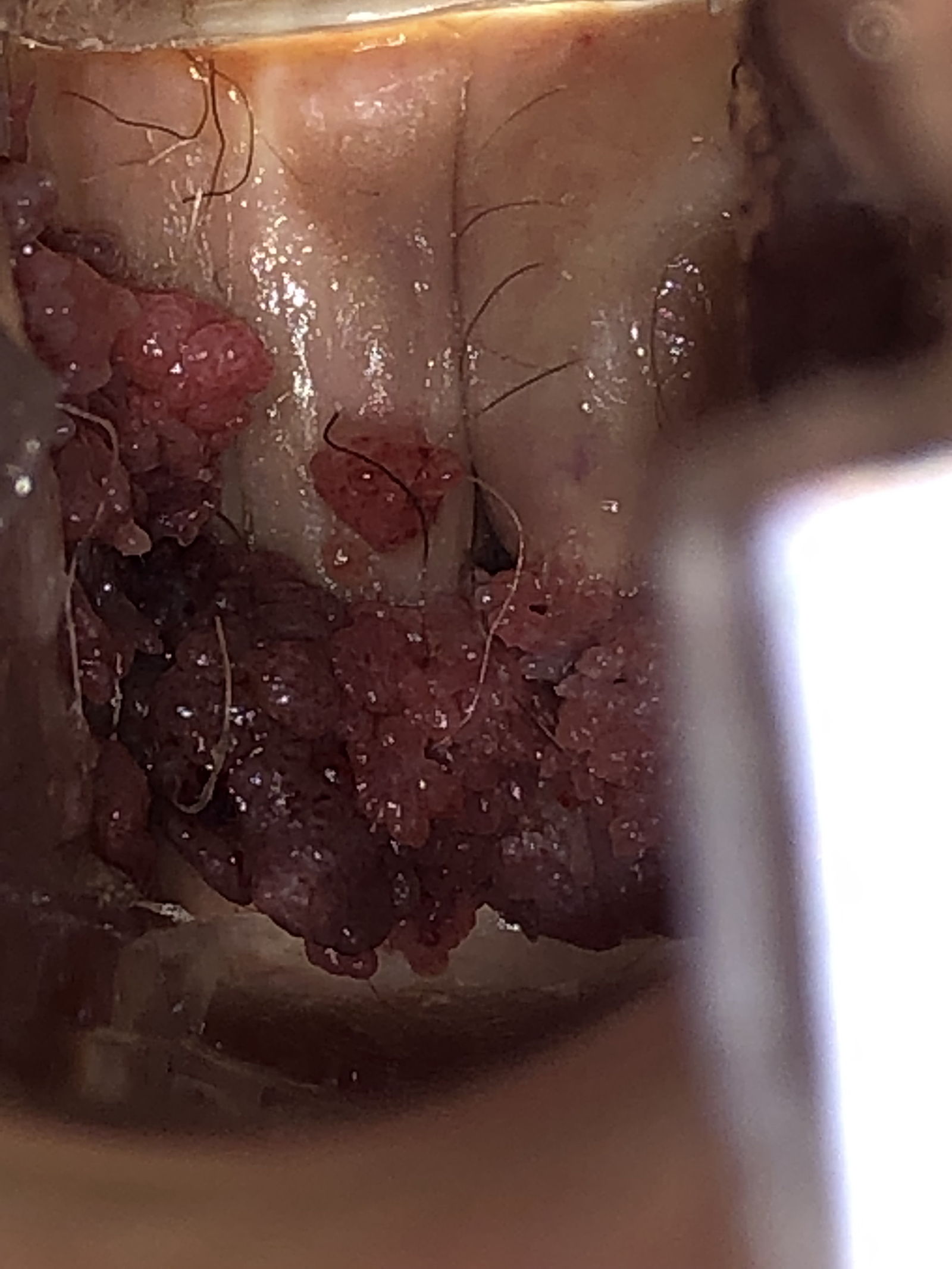
Condylomata acuminata of the neovagina pretreatment.
We therefore initiated treatment with TCA, applied in the office every one-to-two weeks for a total of six treatments until a complete clinical response was noted. TCA application was performed in the following fashion: (1) speculum was inserted into the neovagina, (2) petroleum jelly was applied to the vaginal vault, (3) TCA was applied with a cotton swab to the warts, and (4) vaginal packing was prepared with petroleum jelly and left in place for several hours. The packing was incorporated to reduce the risk of caustic damage to surrounding neovaginal structures. Overall, the treatment was well tolerated, and she did not develop significant pain, ulceration, or localized skin reaction. We did perform electrocautery on one occasion when the lesions were significantly small enough to safely and comfortably perform this procedure in an outpatient setting.
The patient is now 12 weeks post-treatment. Since completion, the patient has not had any disease recurrence or residual tissue damage from TCA treatments. She reported high satisfaction with the treatment and was grateful to avoid additional surgery.
Discussion
It is widely acknowledged that GAS mitigates gender dysphoria and improves sexual function and subjective wellbeing in transgender individuals. 8 Given the rates of STIs among transgender women, it is likely that healthcare practitioners will encounter these in patients who have undergone GAS. The majority of GAS is performed with the penile skin inversion technique, but other tissues may also be used, including intestinal, urethral, peritoneal, and split-thickness skin grafts. It is important to consider the STI risk profile based on tissue type. Whereas HPV has been associated with penile and scrotal skin, other STIs such as chlamydia or gonorrhoea have a predilection for columnar and transitional epithelium and have been identified in transgender women following GAS with colonic mucosa and integrated urethral or peritoneal grafts. 9 , 10
Our case report focuses on a transgender woman who underwent vaginoplasty with the penile skin inversion technique and was subsequently diagnosed with neovaginal warts. This case provides evidence for the clinical utility of TCA in a transgender woman with neovaginal warts, and particularly speaks to its functionality when patient-applied treatments are not feasible, or when an operative procedure is not desired or is contraindicated.
Our literature search identified 11 cases of transgender women with neovaginal condylomata acuminata. Reported treatments ranged from patient-administered methods podophyllotoxin or imiquimod, to physician-operated methods, including CO2 laser ablation, electrovaporization, surgical excision, and total colpectomy.11–18 To our knowledge, this is the first case report of neovaginal warts successfully treated with TCA.
TCA causes the chemical coagulation of tissue proteins and is commonly used to treat genital warts in an office-based procedure.19–22 Treatment with TCA carries the risk of ulceration at its application site. To mitigate this risk, the surrounding tissue should be protected by a gel, as was achieved in our patient with petroleum jelly. TCA is not considered ideal for keratinized tissue, such as the penile skin used to fashion the neovaginal canal in our patient, because it is typically recommend for mucosal lesions. However, the neovaginal lining can lose some keratinization, which may portend increased success on neovaginal warts compared to other lesions for treatment of keratinized tissue. 23 TCA may also be suitable if the neovagina is fashioned from other tissue, such as colonic mucosa or peritoneum.
Though no consensus exists to guide clinical management of neovaginal warts, having a variety of proven treatment modalities is important to optimize and individualize treatment. TCA can be safely and simply applied, and it produces rapid results and high clearance rates at a low cost. 24 This case also considers the utilization of combination therapy when appropriate. We were able to incorporate a single treatment of electrocautery in the clinic when the lesions were small enough for the procedure to be tolerable to the patient. We urge clinicians to adapt their treatment decisions to the individual needs of each patient, based on the overall clinical picture, patient preference, and availability of resources.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.