
Abstract
We present the case of a 28-year-old man with recently-diagnosed human immunodeficiency virus and hepatitis C virus infection. He developed obstructive cholangiopathy secondary to cytomegalovirus and Kaposi sarcoma, both diagnosed by endoscopic retrograde cholangiopancreatography and biopsies. He received antiretroviral therapy, chemotherapy and valganciclovir with full recovery.
Introduction
Human immunodeficiency virus (HIV)/acquired immune deficiency syndrome (AIDS)-associated obstructive cholangiopathy is an obstructive syndrome secondary to inflammation and strictures of biliary ducts due to opportunistic infections; introduction of antiretroviral therapy has reduced its incidence. 1 We present a complex clinical case with advanced immunosuppression and coexistence of at least three conditions that affected his liver and biliary tree.
Case presentation
A 28-year-old man with recent HIV diagnosis was referred because of Kaposi sarcoma (KS); he had weight loss of 10 kg in three months, low-grade fever, diffuse abdominal pain and chronic diarrhea. His baseline studies were: HIV viral load (VL) 82,499 copies/mL, CD4+ T cell count 95 cells/mm3, positive serology for hepatitis C virus (HCV) with a HCV VL of 663,956 copies/mL. Liver function tests (LFTs) showed elevation of alkaline phosphatase (ALP) 215 U/L with a normal range (NR) of 38–126 U/L, gamma glutamyl transferase (GGT) 320 U/L (NR 12–58 U/L), alanine transaminase 69 U/L (NR 12–58 U/L) and aspartate transaminase 57 U/L (NR 15–46 U/L). Computed tomography scan showed reactive lymphadenopathy. Gastrointestinal endoscopy reported digestive tract KS. Bone marrow cultures were negative for opportunistic microorganisms.
In the next four weeks, ALP and GGT increased 1.5 times over NR and his diarrhea worsened. Stool stains showed Cryptosporidium parvum, liver ultrasound reported cholangiopathy. Nitazoxanide 500 mg BID and combination antiretroviral therapy (cART) with tenofovir/emtricitabine/raltegravir was given.
By week 6, diarrhea had improved; however, ALP and GGT increased 15 and 30 times upper the NR, respectively. Cholangioresonance reported nonspecific cholangitis, intra and extrahepatic biliary duct dilatation (Figure 1(a)). Transient elastography ruled out liver fibrosis. At week 7, an endoscopic retrograde cholangiopancreatography reported dilatation of intra and extrahepatic bile ducts; a biopsy was taken and histopathology showed KS and cytomegalovirus (CMV) infection (Figure 1(b) and (c)). The CMV VL was 1962 copies/mL and human herpes virus 8 (HHV-8) VL was 292 copies/mL. At week 8, nitazoxanide was stopped, valganciclovir 900 mg BID was initiated and a first cycle of vincristine/bleomycin chemotherapy was administrated.
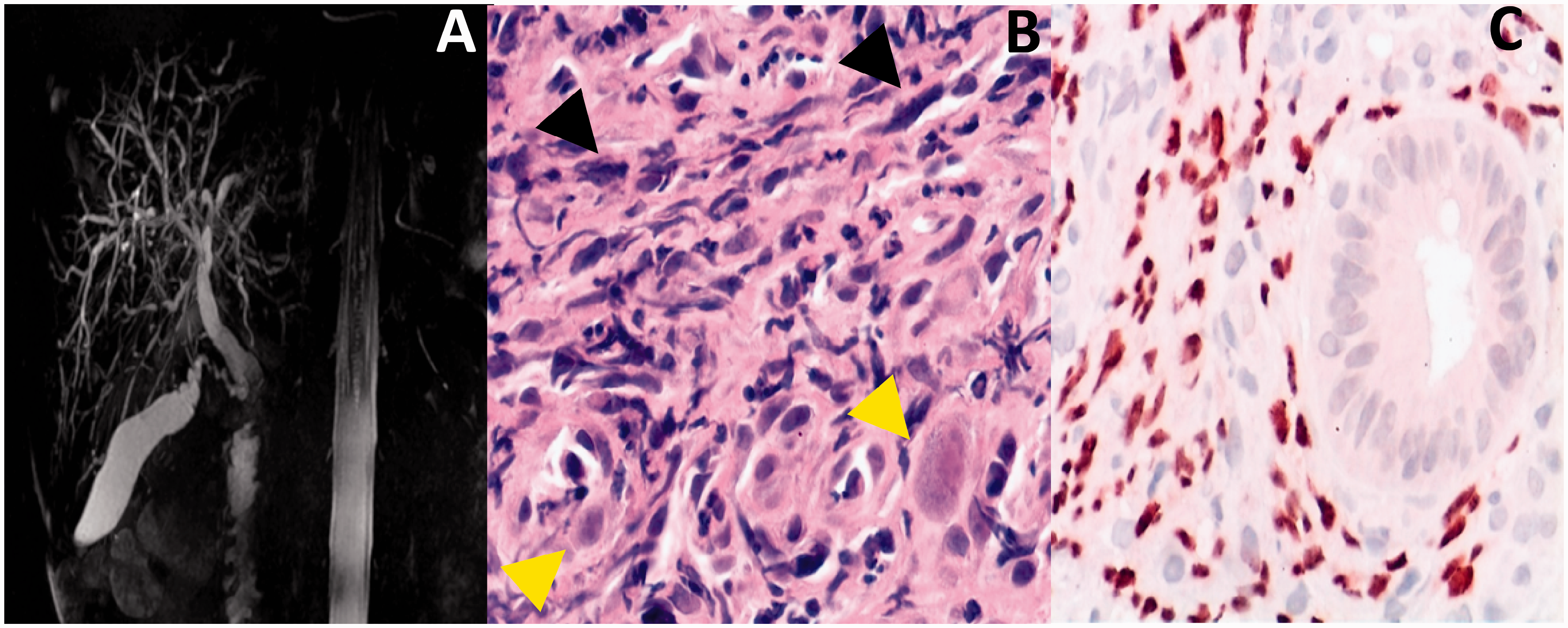
Radiological and histopathological changes compatible with obstructive cholangitis secondary to cytomegalovirus (CMV) and Kaposi sarcoma (KS). (a) Three-dimensional cholangioresonance with dilated intrahepatic and extrahepatic biliary ducts with multifocal strictures and segmental dilations; common bile duct: 12 mm is diagnostic of cholangitis. (b) Histopathology of common bile duct: yellow arrows show cytomegalic cells, caused by CMV; black arrows show fusiform malignant cells of Kaposi sarcoma, caused by human herpes virus 8 (HHV-8) (H&E 40×). (c) Immunohistochemistry positive for HHV-8 (40×).
Over the following weeks, his LFTs improved, abdominal pain and diarrhea remitted, he gained weight and his cutaneous KS lesions regressed with no need to give another cycle of chemotherapy. Valganciclovir was prescribed for 20 weeks until HHV-8 and CMV VLs were undetectable. A follow-up magnetic resonance imaging performed six months later reported a significant reduction of the bile duct dilation. He has been unable to obtain treatment for HCV but his last HIV VL was undetectable and CD4 + T cell count was 162 cell/mm3 at week 30. Figure 2 shows the clinical evolution of the case.
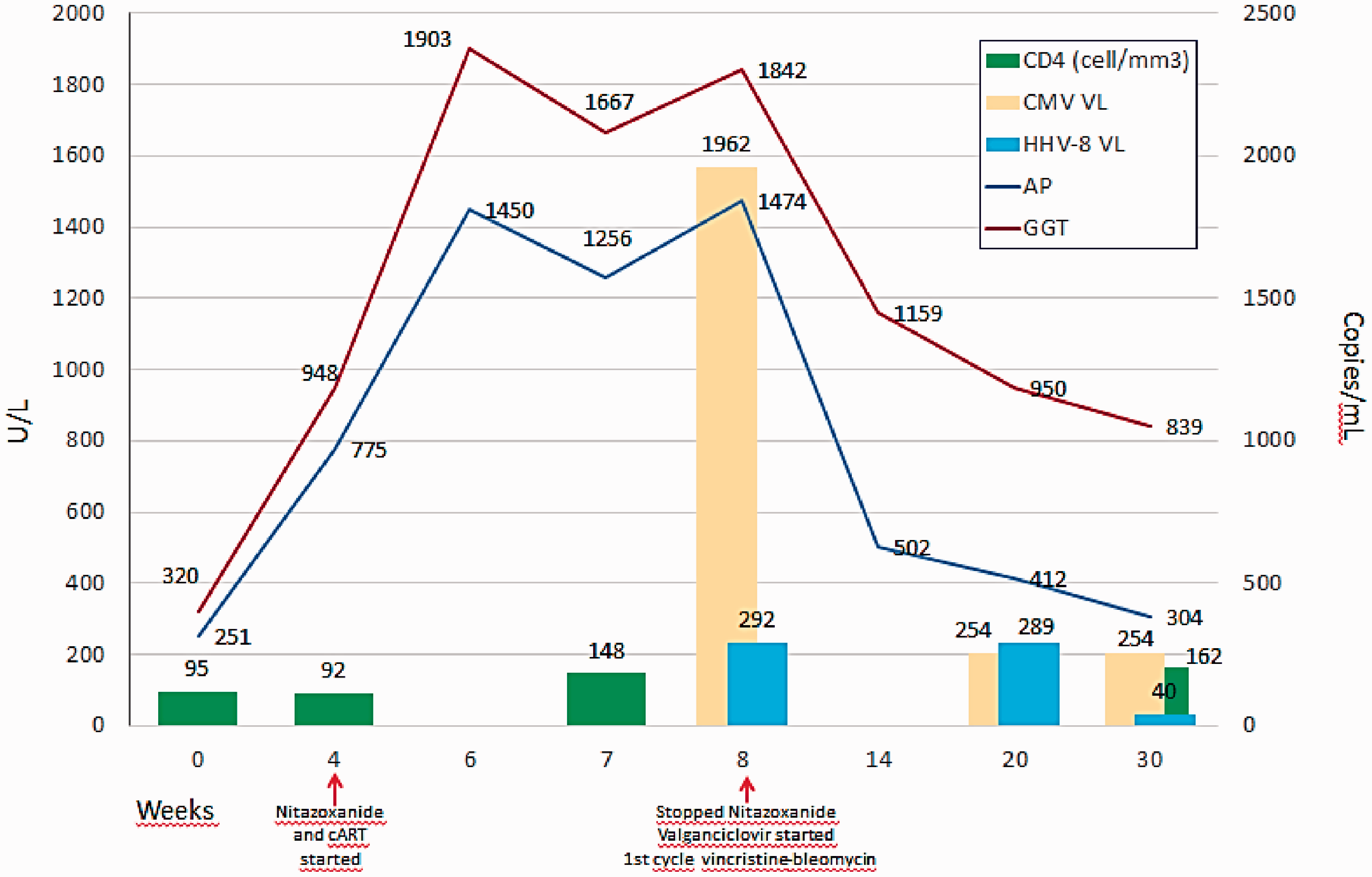
Clinical evolution of the case presented. CMV VL: Cytomegalovirus viral load; HHV-8 VL: human herpes virus 8 viral load; AP: alkaline phosphatase; GGT: gamma glutamyl transferase; cART: combination antiretroviral therapy. Baseline HIV viral load was 82,499 copies/mL and at week 30 was undetectable.
Discussion
The first reports of AIDS-associated cholangiopathy were reported in 1983; 2 , 3 it has been described mainly in immunocompromised patients, with an extremely low CD4+ T cell count and coexistence of opportunistic infections.4–6 To date, approximately 250 cases have been reported, mostly in the pre-cART period. 7 The predominant abnormality in LFTs of patients with cholangitis is raised ALP and GGT. The most common cholangiographic feature is papillary stenosis with dilatation of extra and intrahepatic bile ducts in. Median survival had been reported to be 34 months. 8
CMV infection with gastrointestinal involvement is present in 4.7% of AIDS-affected patients. 7 In the pre-cART era, 14% of patients with liver disease had CMV involvement and unlike other organs liver disease is usually asymptomatic.9–11
KS can affect the liver in 8.6%. 10 Up to 40% of patients with KS in the context of AIDS also have gastrointestinal involvement; nonetheless primary KS in the gallbladder or bile ducts is exceptional.12,13
Two case reports were published with coexistence of CMV and Cryptosporidium infection.14,15 Our case is unique for the coexistence of at least three conditions affecting the patient concomitantly (CMV, KS and HCV). It is possible that Cryptosporidium contributed to the disease but when the biopsy was performed, he had already received one month of antiparasitic treatment and it was not identified in bile ducts. It is also interesting given the low frequency of AIDS-associated cholangiopathy reported in recent years.
Treatment represented a challenge because he required multiple medications with close monitoring of adverse events and drug interactions. Duration of valganciclovir for CMV cholangitis is not well defined. Due to the extremely low CD4+ T cell count and the coexistence of other severe comorbidities, we decided to continue it until clinical recovery and undetectable CMV VL were achieved.
This case taught us that in the context of HIV infection even with mild or no abdominal pain and abnormal LFTs, biliary tract disease should be suspected and ruled out. A comprehensive diagnostic approach must be pursued since there may be more than one opportunistic disease that requires targeted treatment.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.