
Abstract
The characteristics and serological responses of primary syphilis are not completely understood. We aimed to describe the characteristics, the serological responses and presumptive treatment of primary syphilis in HIV-positive and -negative men who have sex with men (MSM). We conducted a retrospective review of microbiological and demographic information from MSM presenting with primary syphilis. There were 111 cases of primary syphilis in MSM, the median age was 46 (IQR = 37–53years) and 40 (36%) were living with HIV. Fifty percent of MSM presented with painful lesions and 14% with extra-genital lesions. Extra-genital lesions were significantly more likely to be painful than non-genital lesions (OR 4.72; 95%CI = 1.25–17.83, p = 0.02). Overall, a reactive serological response demonstrated a sensitivity of 80% (57/71) compared with Treponema pallidum PCR. Serology was more sensitive in MSM with no previous syphilis (OR = 3.38, 95%CI = 1.00–11.43, p < 0.05). MSM presenting with painless lesions were more likely to be treated presumptively (OR = 3.39, 95%CI = 1.38–8.33, p < 0.002). There were no differences in the characteristics, serological responses or management according to HIV status. Fifty percent of MSM with primary syphilis presented with painful lesions; extra-genital lesions are more likely to be painful than genital lesions, serology is positive in 80% and there were no differences between HIV-positive and -negative MSM. Understanding the characteristics of primary syphilis will underpin public health campaigns.
Introduction
Infectious syphilis has increased significantly in the past 20 years especially in men who have sex with men (MSM). 1 , 2 As the incidence of syphilis has increased, the clinical presentation of primary syphilis is increasingly variable: lesions can be painful in up to 74% with a corresponding increase in extra-genital lesions (including anal and oral).3–5 Clinicians are relying on molecular technology using Treponema pallidum polymerase chain reaction (TP-PCR) testing, and serology has been shown to be insensitive compared to TP-PCR in men with primary syphilis.4–6 Many patients attending sexual health clinics with lesions of primary syphilis are being treated presumptively on the day, due to the lack of point-of-care testing of genital lesions. 5 , 6 Understanding the clinical characteristics of primary syphilis could underpin future public health strategies to reduce the transmission and morbidity of syphilis. We aimed to describe the characteristics of primary syphilis lesions, the sensitivity of serology and presumptive same-day treatment of primary syphilis in our large cohort of MSM.
Methods
This is a cross sectional analysis of the electronic clinical records of MSM who were diagnosed with primary syphilis between January 2016-March 2020 in an open access sexual health clinic in Brighton, UK. The clinic sees an average of 6540 attendances by MSM per year. All MSM presenting with genital or extra-genital lesions had a clinical history and examination by a sexual health clinician, as well as serology for syphilis. In Brighton, (as in most of the United Kingdom), we use a reverse sequence syphilis screening algorithm: blood samples are screened using a treponemal specific enzyme immunoassay (EIA) [Abbott Architect© Abbott Park, IL, USA] and if positive, syphilis is confirmed using Venereal Disease Research Laboratory (VDRL) and the Treponema pallidum particle agglutination (TPPA) [Serodia, Fujirebio Inc., Tokyo, Japan]. A TP-PCR (Fast Track Diagnostics, Luxembourg [platform is a 47 Kda target gene provided by Launch Diagnostics Ltd, Longfield, UK]) taken from the genital or extra-genital lesion and herpes simplex virus (HSV)-PCR testing was performed from the same sample (Fast Track Diagnostics, Luxembourg). During the study period, TP-PCR testing from genital specimens was introduced, although not exclusively. Dark field microscopy was not used routinely during the study period and results of dark field microscopy were not collected as part of this study. MSM with suspected syphilis would either be offered same-day presumptive treatment at the discretion of the sexual health clinician or recalled to the clinic for treatment once results of the TP-PCR or serology were reported by the laboratory. We defined cases of primary syphilis as sexually-active MSM presenting with painful or painless genital or non-genital (oral or anal) ulcers or skin lesions which were either TP-PCR positive or the patient had a reactive serological response and no recent history of rash and a negative HSV-PCR. 7 , 8 We excluded cases where MSM presented with a rash as these most likely were presentations of secondary syphilis.
In MSM with no previous history of syphilis (no clinical history of previous syphilis or a previous recent (last 12 months) negative EIA); we defined a reactive serological response as a reactive EIA and reactive confirmatory TPPA. For MSM with a previous history of syphilis (from their clinical history, either from the patient if they were new to the clinic, or from their documented clinical records (including serology) if their previous syphilis was treated in our department) we defined a reactive serological response as a four-fold or more increase in VDRL titre. Data were analysed using Excel. Bivariate associations were examined using crude odds ratios or Mann-Whitney U tests using 95% confidence intervals (CI).
Results
Overall, there were 120 cases of primary syphilis, 9 of which had a positive HSV-PCR leaving 111 cases for analysis. The median age was 46 years (IQR = 37–53) and 40/111 (36%) were HIV positive. Confirmation of diagnosis of primary syphilis was made on TP-PCR test [14/111 (13%)], TP-PCR test and serology [57/111(51%)] and serology alone [40/111 (36%)]. Overall there were 83/111 (75%) MSM with no previous syphilis (diagnosis made on TP-PCR [7/83 (8%)], TP-PCR and serology [44/83 (53%)] and serology alone [32/83 (39%)]; and 28/111 (25%) with previous syphilis (diagnosis made on TP-PCR [7/28 (25%)], TP-PCR and serology [13/28 (46%)] and serology alone [8/28 (29%)] (Figure 1). Ninety-six (86%) presented with genital lesion(s), 15/111 (14%) presented with extra-genital lesion(s) (11 anal, 4 oral) and 56/111 (50%) presented with painful lesions. Extra-genital lesions were significantly more likely to be painful than genital lesions (OR 4.72; 95%CI = 1.25–17.83, p = 0.02), and MSM with extra-genital lesions had a significantly higher VDRL titre (p = 0.03). Overall, serology was reactive [no previous history of syphilis (n = 51); previous syphilis (n = 20)] in 57/71 (80%, CI = 71%–90%) of MSM with a positive TP-PCR test. Serology was reactive in 44/51 (86%) MSM who had no previous syphilis with a positive TP-PCR and 13/18 (72%) MSM who had previous syphilis with a positive TP-PCR. Serology was more sensitive in MSM with no previous syphilis (OR = 3.38; 95%CI = 1.00–11.43, p = 0.05). Eighty-one out of 111 (73%, 95%CI = 64.7–81.2) were treated presumptively on the day of presentation and in those not treated on the day, the median number of days until treatment was 7 days (range = 3–28 days). MSM presenting with painless lesions were more likely to be treated presumptively on the day of presentation than MSM with painful lesions (OR = 3.39, 95%CI = 1.38–8.33, p < 0.002). There were no differences in the characteristics and serological responses of primary syphilis between HIV-positive and HIV-negative MSM, nor whether they were treated presumptively or not (Table 1).
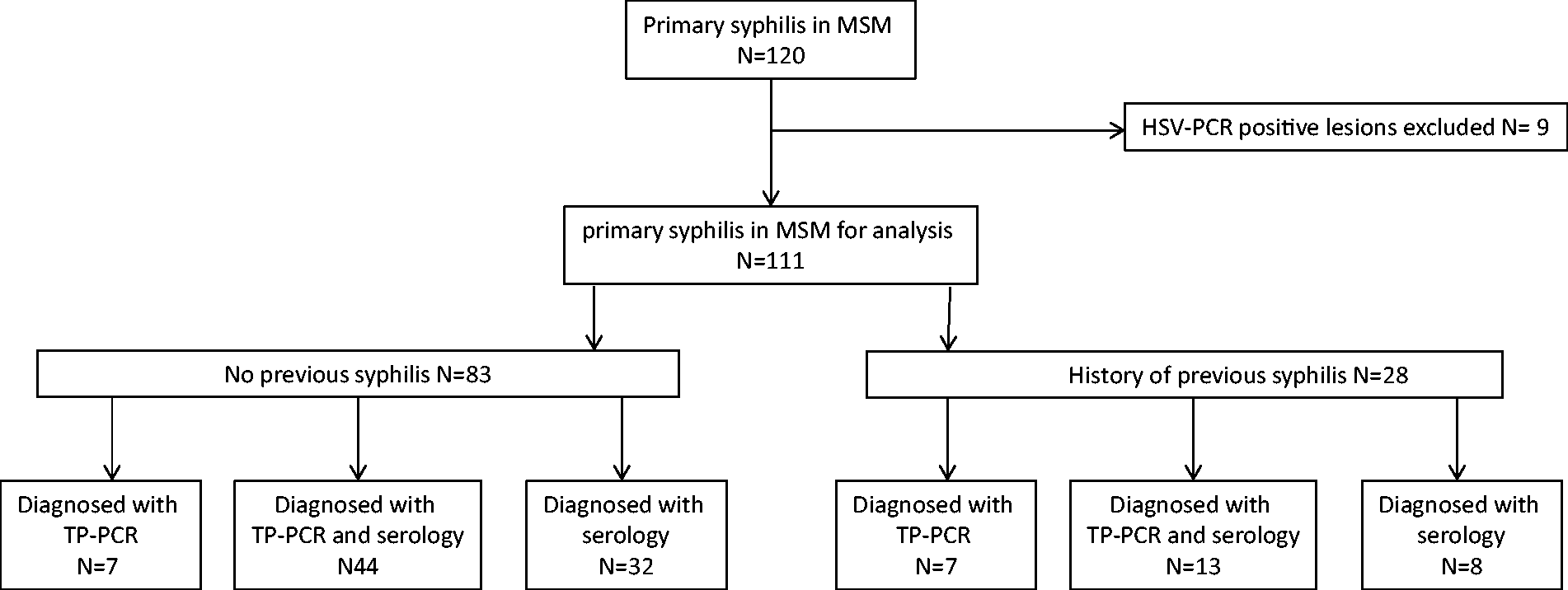
Primary syphilis in men who have sex with men; N = 120.
Clinical features and management of 111 cases of primary syphilis in men who have sex with men, Brighton Sexual Health Clinic, January 2016–March 2020.

aVDRL=venereal disease research laboratory.
Discussion
We have shown that painful lesions of primary syphilis in MSM are common, particularly in extra-genital lesions. Studies from Australia have shown that primary syphilis is painful in 49%-74% of cases although this is the first study to our knowledge showing that extra-genital lesions are significantly more painful than genital lesions. 4 , 5 It is likely that extra-genital syphilis, particularly ano-rectal primary syphilis, becomes secondarily infected causing increased inflammation and pain. Patients with painful ano-genital lesions are probably presenting to clinical services not as experienced in the management of genital ulcer disease and are not tested appropriately for syphilis, so it is important that we challenge the accepted dogma that primary syphilitic lesions are painless.7–9
Only 80% of MSM with primary syphilis in our study with a positive TP-PCR had a reactive serological response. We also showed that MSM presenting with extra-genital primary syphilis have a higher VDRL titre than MSM with genital lesions. Data from a single small study in South Africa suggest that the sensitivity of serology in primary syphilis is 71%. 6 To our knowledge, there are no other data comparing VDRL titres of primary syphilis in different anatomical sites and the relevance of this is not clear. It is plausible that secondarily-infected lesions allow more rapid invasion of TP into the blood and an enhanced serological response. This could also be explained by asymptomatic lesions being present longer before becoming secondarily infected and painful, and therefore the VDRL titre has had longer to evolve. MSM with primary syphilis in our study who have no previous history of syphilis are more likely to have a serological response than MSM who have had previous syphilis. Again the significance of this finding is not clear but given the increasing incidence of syphilis, particularly in MSM using HIV pre-exposure prophylaxis (PrEP), repeat testing to ensure that re-infection is not missed is important. 10 In an era of increasing rates of syphilis, some of which may be managed by non-specialists, it is important to understand the limitations of syphilis serology in MSM presenting with ano-genital lesions. A single negative serology test may miss a case of primary syphilis and this message is important when considering public health strategies to control syphilis.
MSM in our study who present with painless lesions of primary syphilis are more likely to receive presumptive treatment than MSM with painful lesions. In an Australian study of 31 MSM with primary syphilis, there were no differences in clinical presentation between MSM who were treated presumptively or waited for the results of diagnostic tests. 5 In a much larger study of 183 MSM with primary syphilis, MSM were more likely to be treated presumptively if the lesion(s) were painless, however, this difference was not significant. 4 It appears that clinicians are still making assumptions about painful genital and extra-genital lesions and attributing these on the day of presentation to non-syphilis causes of genital ulceration such as HSV or anal fissures. MSM who did not receive presumptive treatment waited an average of seven days before being treated. MSM with symptomatic STIs may continue to be sexually active, leading to further transmission of STIs. 11
There were no differences in the characteristics of primary syphilis nor the likelihood of MSM receiving same-day presumptive treatment between HIV-positive and -negative MSM. Previously studies have shown that MSM living with HIV are more likely to have painful and extra-genital lesions. 4 , 12
Public health interventions for syphilis control rely partly on training non-specialists and at-risk communities to recognise symptoms of syphilis. Awareness that primary syphilis can present with painful and extra-genital lesions is an important public health message. In the absence of rapid, point-of-care testing of lesions, clinicians need safe, accurate and validated clinical decision-making tools on when to offer presumptive treatment, preferably based on accurate, contemporary data on the clinical characteristics of primary syphilis.
There are several limitations to this study: this is a single-centre retrospective analysis of patient records and we could not guarantee the accuracy of the clinical data. We only included data on MSM who had reactive serology and or a positive TP-PCR; MSM with atypical lesions may not have been sampled and will have been excluded from this analysis. MSM who were co-infected with syphilis and HSV were excluded from the analysis in the study design, so the features we have described are not representative of populations of MSM with syphilis-HSV coinfection. This is a sample from a tertiary sexual health setting seen by experienced sexual health clinicians and so thesedata may not be generalisable to a non-specialist clinical setting, for example in general practice.
In conclusion, we have described the contemporary characteristics of primary syphilis in HIV-negative and HIV-positive MSM. Fifty percent presented with painful lesions, and extra-genital lesions are more likely to be painful than genital lesions. Serology is only sensitive in 80% of MSM with primary syphilis and is more sensitive in MSM with no previous history of syphilis. Clinicians in our study are more likely to treat MSM presumptively if their primary syphilis lesion is painless. We have also shown that there are no differences in the characteristics of primary syphilis between HIV-positive and -negative MSM. Understanding the characteristics of primary syphilis will support public health campaigns which focus on testing at-risk and symptomatic populations of MSM.
Footnotes
Acknowledgements
We would like to acknowledge Dr. Mohammed Osman Hassan Ibrahim FRCPath, consultant clinical microbiologist and the clinical team at Brighton & Sussex Sexual Health for their assistance with this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.