
Abstract
Anogenital warts (AGWs) rank among the most frequent sexually transmitted infections in young adults. They are benign lesions, but they pose a significant economic cost to health care systems and a substantial psychological burden on patients, who need evidence-based counselling. Human papillomavirus (HPV) vaccination has shown very high protection rates against AGWs in clinical trials and real-world settings but vaccination coverage remains low in many countries. The aim of this review is to summarize the current evidence on the risk factors for AGW development and to present the available real-life data on the impact of HPV vaccination on AGW incidence. An increased number of lifetime sexual partners, a new sexual partner in the last 12 months, smoking, and immunosuppression have been associated with increased risk for AGWs. HPV vaccination has led to a dramatic decline in AGW incidence in populations that have achieved high vaccination rates. These conclusions can contribute to primary prevention of AGWs and evidence-based counselling of AGW patients.
Keywords
Introduction
Human papillomavirus (HPV) infection is the most widespread sexually transmitted infection (STI) around the world. More than 100 HPV types have been identified, among which 40 infect the anogenital area. High-risk HPV types are carcinogenic and they are associated with anogenital precancers and cancers, whereas low-risk HPV types are associated mostly with anogenital warts (AGWs) and other benign diseases.1–3
AGWs, with an annual incidence rate between 100 and 200 new cases per 100,000 general adult population, rank among the most frequent STIs. 4 HPV low-risk types 6 and 11 account for approximately 90% of all cases of AGWs. However, high-risk HPV types are also occasionally detected in AGWs (usually as co-infections with HPV types 6 or 11). 5
Even though AGWs are benign lesions, several studies have reported an increased risk of cervical intraepithelial neoplasia (CIN) grade 2 or worse, 6 of penile intraepithelial neoplasia 7 and of anogenital cancers (especially HPV-related cancers) 8 in patients with AGWs. Furthermore, AGWs place a considerable economic cost on health care systems9–12 and a great psychological burden on patients, 12 , 13 who need evidence-based answers to their many questions about their condition. Several groups of patients need specific counseling, such as patients with a first diagnosis of AGWs, especially young women who worry about a possible HPV cervical infection, and patients who belong to high-risk groups for development of AGWs.
Fortunately, the majority of AGWs can be primarily prevented through vaccination. The quadrivalent 14 and, more recently, the nine-valent vaccine 15 against HPV infection include the HPV types 6 and 11 that cause 90% of AGWs. These vaccines have led to a significant decline in AGW incidence in countries that have managed to achieve high vaccination coverage rates.16–26 HPV vaccination has also been used off-label for the treatment of recalcitrant common warts. 27 , 28 However, HPV vaccination has created considerable controversy and the vaccination rates are low in many countries.29–32 Thus, identifying risk factors for the development of AGWs is still of paramount importance in our efforts for primary prevention of the disease.
In this review, we present available data on epidemiological risk factors for the development of AGWs and on the real-life impact of HPV vaccination in an effort to contribute to primary prevention of the disease and evidence-based counselling for our patients.
Methods
The PubMed database was searched for articles published from January 2000 until December 2019 using the following search terms: (genital warts or genital wart or anogenital warts or anogenital wart or condyloma acuminate or condylomata acuminate) AND (epidemiology or risk factor or contraceptives or smoking or immunosuppression or organ transplantation or condoms or HPV vaccination or HPV vaccine or papillomavirus vaccine or papillomavirus vaccination). The reference lists of retrieved articles were also searched for relevant publications.
Epidemiological risk factors associated with AGW development
AGWs is a disease of young adults. Incidence peaks before 24 years of age in females and between 25 and 29 years of age in males. 4 Most studies based on administrative databases or medical chart reviews reveal higher incidence and/or prevalence for males compared with females. In surveys that include both genders, however, more females than males report a diagnosis of AGWs. 4
Several characteristics of sexual behavior have been associated with increased rates of AGW. 33 Presence of multiple sexual partners has been well studied in both sexes, especially in young women, in several countries and it is consistently found to be an important parameter contributing to the increased burden of AGW development. In a population-based cross-sectional study of nearly 70,000 women from the 4 Nordic countries (Denmark, Iceland, Norway, Sweden), history of AGWs was strongly correlated with the lifetime number of sex partners. 34 In another cross-sectional study that included almost 8,000 men and women from the Baltic countries (Estonia, Latvia and Lithuania), five or more lifetime sexual partners were associated with ever receiving a diagnosis of AGWs in both men and women. 35 Data from a population-based cross-sectional study in the Czech Republic with 32,974 participants reported that a number of more than 14 lifetime sexual partners was the strongest risk factor for AGW occurrence. 36 A probability sample survey in the United Kingdom that interviewed almost 10,000 men and women who accessed care for a possible STI revealed a strong association of AGWs with increasing number of sexual partners. 37 A national probability sample survey conducted in Slovenia showed that women with at least 10 male partners were more likely to have a previous diagnosis of AGWs. 38 More than 2 sexual partners in the previous 24 months was also associated with a history of AGWs in an Italian cross-sectional study that included 9,259 university students. 39 The Australian Longitudinal Study on Women’s Health, a postal survey that included 9582 women, reported also that the odds of AGWs increased with the number of sexual partners. 40 Finally, in a prospective cohort study that included 1,020 Nigerian women, women with a higher number of sexual partners in the preceding year were more likely to develop AGWs. 41
Another aspect of sexual behavior that has been associated with the occurrence of AGWs is the acquisition of a new sexual partner. Data from the placebo arm of 2 randomized, phase III trials of a quadrivalent HPV (types 6, 11, 16, and 18) vaccine that included 8,800 women highlighted an increased risk for AGW development among women with a new sexual partner in a period of 12 months prior to AGW development. 5
Clinicians often advise the use of condoms in an effort to reduce the transmission of STIs. The protective role of condoms in AGW occurrence was initially reported by Wen et al. in a retrospective case-control study in men and women with and without newly diagnosed AGWs who had attended the Sydney Sexual Health Clinic. Overall, 977 patients and 977 controls were evaluated and the results showed that consistent condom use exerted a protective role against acquiring AGWs, equally in both sexes. 42 The same conclusion was reached by two recent studies that have already been mentioned above, one from Italy 39 and the other from the United Kingdom. 37 Both of these studies were cross-sectional and included approximately 10,000 participants from the general population.
Other studies, however, have not confirmed this protective role. Wiley et al. followed 3,000 men who have sex with men (MSM) for almost 5 years and reported no association between consistent condom use and development of external anal warts. 43 Similarly, a case-control study from Turkey that included 200 patients with AGWs and 200 controls reported no significant differences in condom use between patients and controls. 44 Furthermore, the population-based cross-sectional study of nearly 70,000 women from the 4 Nordic countries 34 and the prospective cohort study that included 1,020 Nigerian women 41 have both revealed an increased risk of AGWs in women that reported use of condoms.
The reason behind the contradictory results of the studies concerning the use of condoms is unclear. Possible explanations include recall bias, response bias or interviewer bias as well as the fact that most people may not be using condoms regularly or at the beginning of the sexual contact. Thus, a more detailed questionnaire is needed if we want to capture the subtle variations in the use of condoms by different people. Furthermore, the use of condoms may confer a false sense of “absolute protection” which, in turn, may lead people to riskier sexual behavior. Clinicians should continue to advise the use of condoms from the beginning of the sexual act but they should also make it clear that condoms may only reduce but not eliminate the transmission of AGWs.
In addition to the above mentioned risk factors for AGW development, history of being exposed to another STI has also been investigated. Data from the cross-sectional study conducted in the 4 Nordic countries among 70,000 women showed strong correlation between AGW occurrence and history of a previous STIs (genital chlamydial infection, gonorrhea, genital herpes, and trichomoniasis). 34 More recent data extracted from the cross-sectional survey in the Baltic countries 35 and the cross-sectional Italian study on university students 39 confirmed this association, in both men and women. The same is true for another cross-sectional study that included almost 23,000 Danish men. 45 Contrary to the above results, the retrospective case-control study from Sydney that included 977 patients with AGW and 977 controls showed that men and women with a history of previous chlamydial infection, as well as women with a history of genital herpes, were less likely to acquire AGWs. 42 This latter study, however, had a different study design (case-control study with data collection from medical records) compared with the above mentioned studies (cross-sectional studies with data collection from questionnaires) and examined each STI separately, not the presence of an STI generally.
MSM have been found to be disproportionately affected by STIs such as syphilis and gonococcal urethritis. 46 , 47 Whether sexual orientation comprises another risk factor potentially associated with AGW occurrence is not that clear. Cross-sectional analysis of data from 13,000 AGW patients that had visited STI clinics of the Sexually Transmitted Diseases Surveillance Network in the USA revealed the same prevalence of AGWs between MSM and men having sex with women (MSW). 48 However, in the cross-sectional Italian study on university students, 39 MSM were found to carry a significantly higher risk for ever developing AGWs, compared to MSW. The probability sample survey in the United Kingdom that interviewed almost 10,000 men and women who accessed care for a possible STI 37 reported also that the lifetime diagnosis of AGWs was more frequent in MSM, compared with MSW and, similarly, more frequent in women reporting sex with women (WSW), compared to women reporting sex exclusively with men (WSM). Both men and women that reported a same-sex partner in the past 5 years were more likely to report a history of AGWs but, interestingly, this association was no longer significant after adjusting for numbers of sexual partners. So, with the exception of the American study that assessed AGWs prevalence, 48 both the Italian 39 and the British 37 studies found an increased lifetime occurrence of AGWs in MSM and in both MSM and WSW, respectively, regardless of the reason for that association.
Even though sex between women is thought to carry a lowrisk for STI transmission, WSW have been reported to have significantly more male partners, engage more frequently in unsafe sex practices and receive more STI diagnoses, compared with women who report sex exclusively with men. 49 The results from the British study suggest an increased risk regarding the occurrence of AGWs in WSW and this risk should be further explored with more studies. Until then, WSW should not be ignored in health promotion campaigns about sexual health and HPV vaccination.
The use of oral contraceptives has also been investigated in several studies with contradictory results. Earlier studies that have been reported in the 2000s, such as the Australian Longitudinal Study on Women’s Health 40 and the study from the 4 Nordic countries 34 have reported a positive association between AGWs and oral contraceptives use. More recent studies, however, including the Italian study on university students 39 and the study from the Baltic countries, 35 have failed to report such an association. Differences in oral contraceptive regimens between the 2000s and more recent years may be a possible reason for the conflicting studies’ outcomes.
Apart from the above mentioned features of sexual behavior, other factors such as smoking have also been investigated in AGW studies. In most studies, an increased risk for AGW occurrence among smokers has been reported. This risk may be attributed to smoking-induced immunosuppression, 50 as well as to higher risk sexual behavior that smokers may have. In the retrospective case-control study from Sydney, 42 cigarette smoking was found to have a highly significant dose-response effect in males. Smokers of more than 10 cigarettes per day were twice as likely to have AGWs as were non-smokers, while smokers of less than 10 cigarettes per day showed a significant but lesser risk. In females, however, the association was significant only in the univariate analysis. In the population-based cross-sectional study of nearly 70,000 women from the 4 Nordic countries, smoking for >59 pack-years increased the probability of reporting AGWs. 34 A longitudinal analysis including 58,094 women from Denmark, Iceland, Norway and Sweden reported that smokers had an increased risk of being diagnosed with AGWs compared with non-smokers, while smokers experienced a 0.6% increased risk of being diagnosed with AGWs for each additional cigarette smoked daily. 51 A positive correlation between smoking and AGW burden was also detected in the Czech population, 36 in Italians, 39 and in Danish men. 45 A Turkish study has showed that smoking is furthermore associated with the duration of an AGW episode. 44 A very recent cross-sectional case control study from Greece that included 196 women with AGWs, 315 women with recent cervical HPV infection and 178 control women revealed significantly more smokers in the AGW group compared not only with the control but also with the “recent cervical infection” group. 52 Finally, a systematic literature review that was published a few years ago concluded that both incidence and recurrence rates of AGWs are significantly increased in smokers. 50
Immunosuppressed and people living with HIV (PLHIV) comprise a special risk group, which is vulnerable to HPV infection and AGWs. HIV infection has been associated with increased risk for the presence of any HPV, high-risk HPV and multiple HPV infections.53–55 Furthermore, prolonged persistence of HPV infection has been observed among adolescents living with HIV. 56 On the other hand, the presence of an HPV infection has also been associated with increased risk of HIV acquisition. 57 As far as AGWs are concerned, increased AGW prevalence in women living with HIV has been reported in two large prospective studies conducted in the USA that included almost 4,000 women. 58 In a prospective cohort study that included almost 1,000 Nigerian women, 41 both HIV-positive and HIV-negative, HIV infection was identified as a risk factor for prevalent AGWs. Finally, HIV positivity was reported to be a risk factor for AGWs among both men and women in a systematic review and meta-analysis of data from Sub Saharan Africa. 59
In addition to PLHIV, organ transplant recipients have also been shown to carry an increased risk of AGW occurrence. A recent study that included 120 organ transplant recipients showed an AGW prevalence of 24.2%. 60 Interestingly, 92.5% of included patients were not aware of the presence of their genital lesions during history taking. Non-white males carried the greatest risk. Another recent register-based prospective cohort study from Denmark 61 evaluated the risk for AGWs in 3,268 renal transplant recipients (RTRs) and compared it with a cohort of 162,910 non-RTRs. RTRs, and especially female RTRs, were found to have substantially higher risk of AGWs than non-RTRs. The risk increased <1 year after transplantation and remained increased for more than 10 years. A regular anogenital examination can, thus, be considered for organ transplant recipients to detect not only AGWs but also genital skin cancers, which have similarly been reported in this group. 60 Furthermore, given the less than desired levels of HPV vaccination in populations, consideration should be given for HPV vaccination electively prior to solid-organ transplantation.
All studies included in this review on the risk factors for the development of AGWs are summarized in Table 1.
Risk factors associated with increased risk for AGW development.
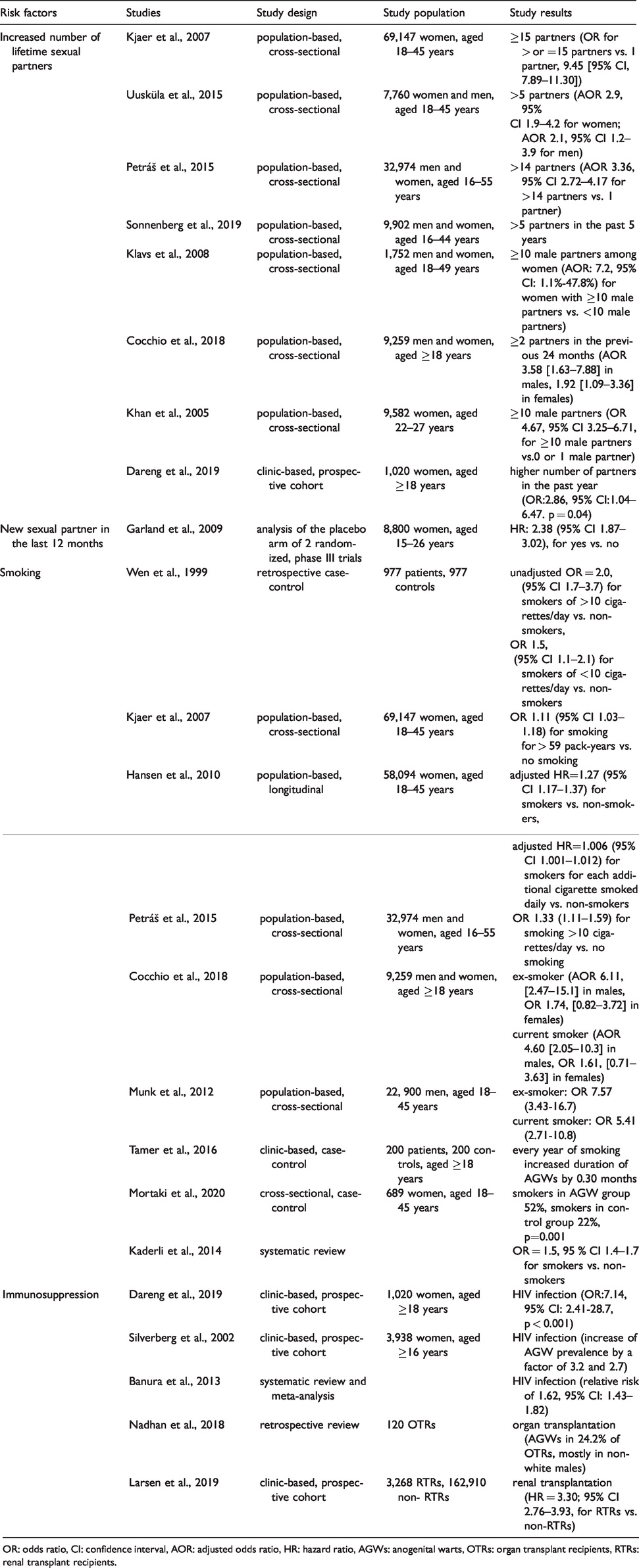
OR: odds ratio, CI: confidence interval, AOR: adjusted odds ratio, HR: hazard ratio, AGWs: anogenital warts, OTRs: organ transplant recipients, RTRs: renal transplant recipients.
The real-life impact of HPV vaccination on AGW development
The real-life impact of HPV vaccination on AGW incidence has been investigated in several studies conducted around the world in high-income countries. Data from low- and middle-income countries are lacking. A recent meta-analysis that included data from 14 high-income countries revealed that, after 5–8 years of vaccination, AGW diagnoses decreased significantly by 67%, 54% and 31% among girls and women aged 15–19 years, 20–24 years and 25–29 years, respectively. 62
Fairley et al. conducted a retrospective study from 2004–2008 in Australia, a country that has provided free quadrivalent HPV vaccination since 2007 to girls and women 12–26 years of age. The study reported that the proportion of women under 28 years with AGWs decreased by 25.1% per quarter in 2008, just 1 year after the implementation of the vaccination programme. 17 In the same country, the National HPV vaccination programme extended in 2013 to boys and the coverage rates for both males and females are among the highest observed worldwide. A recent review on the impact of 10 years of HPV vaccination in Australia 18 reported substantial declines in AGW incidence among vaccine-eligible women: relative to 2006–2007, national hospitalisation rates related to AGWs declined by 89.9%, 72.7% and 42.1% in females aged 12–17, 18–26 and 27–30 years, respectively, with no significant change for women aged 31–69 years. Reduction in the incidence of AGWs was also observed in heterosexual men even before the introduction of the male vaccination programme, suggesting a substantial herd effect in that population.
Towards the same direction, data from Denmark 5 years after the implementation of an HPV vaccination programme for girls and women showed a significant decrease in AGW incidence by 55% in women aged 12 to 35 years and by 36.6% in men aged 12 to 29 years, suggesting again a herd protection in the male population. 19 Similar data are reported from Belgium, where the HPV vaccination programme in girls 12 to 18 years old resulted in a 72% reduction in AGW incidence in women targeted by the programme and a herd protection of 51% in men aged 16 to 22 years. 20 A study from England also revealed a 82.3% decline in the rate of AGW diagnoses among females aged 15–17 and 67.7% among same-aged heterosexual males 5 years after the introduction of a quadrivalent vaccination programme in females. 21 Finally, a systematic review in the USA also reported consistent declines of AGWs in both females and males <25 years old, after the introduction of HPV vaccination. A lower risk of AGWs was demonstrated even for those receiving at least one dose of vaccine compared to those unvaccinated. 22 An exception to the rule of herd protection in males observed in the above countries is New Zealand, where the diagnosis of AGWs declined in women eligible for vaccination but not in men. 23
The effectiveness of HPV vaccination in reducing the incidence of AGWs has also been reported in studies from Israel 24 and Spain. 25 Furthermore, a population-based cross-sectional survey 26 of 19,199 women aged 16 to 40 years, chosen randomly from the general population in the Czech Republic, revealed a reduction of 90% in the acquisition of AGWs in immunized women from the first year of the completion of the quadrivalent vaccination. Notably, the vaccination also caused a reduction in the prevalence of recurrent AGWs by 89%.
However, despite the reported efficacy and effectiveness of HPV vaccination and despite the introduction of HPV vaccination programs worldwide, vaccine coverage has been suboptimal in several countries. In the USA, only 49.5% of females and 37.5% of males ages 13 through 17 have received all recommended vaccine doses, rates that are far below the Centers for Disease Control and Prevention’s Healthy People 2020 target of 80% coverage. 27 In most USA states, it is the only routinely recommended vaccine not required for school attendance. 63 In a large cross-sectional survey in Canada, among 5,720 girls, aged 12–14 years, 27.7% had not received any dose of the vaccine, despite the presence of school-based HPV vaccine delivery, while 14.4% of parents reported having refused to administer the vaccine to their daughters. 30 In Denmark, a rapid decline in vaccination uptake has been noticed after 2014, with coverage rate dropping from 90%, for girls born in the period of 1998 to 2000, to 54%, for girls born in 2003. 31 The decline followed negative public perception regarding the vaccine’s safety profile. The main reasons reported from parents for not vaccinating their daughters were concerns about vaccine safety, a desire to wait until their daughter was older, and lack of adequate information to give informed consent. 32 Interestingly, higher education has been reported to be associated with a higher risk of refusal of the HPV vaccine. 30 , 32
Conclusions
According to reported data, lifestyle and comorbidities of individuals can affect the risk for AGW development. An increased number of lifetime sexual partners, a new sexual partner in the last 12 months, smoking, and immunosuppression have been associated with increased risk for AGWs. The data for the association of condom and oral contraceptive use, as well as the presence of other STIs, with the appearance of AGWs are contradictory. Counseling about high risk sexual behavior and smoking, mainly among the younger age groups, is essential for reducing AGW occurrence. Regular anogenital skin examination should be offered to immunosuppressed patients, especially to PLHIV and to organ transplant recipients. In addition, routine implementation of prophylactic vaccination against HPV infection, for both females and males, especially prior to the initiation of sexual activity, is anticipated to maximize disease control and provide substantial benefits for public health.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.