
Abstract
Intimate partner violence (IPV) and sexually transmitted infections (STIs) are significant public health problems worldwide. However, most research on this association and risk of STIs has been conducted in Western countries and may not be generalizable to women living in different contexts, such as Thailand. We aimed to examine prevalence of IPV and identify factors associated with STIs among Thai women. Participants were patients aged 15–49 years attending two gynecology clinics at a university hospital in Bangkok, Thailand. Data were collected through an anonymous structured questionnaire, including sociodemographic characteristics, IPV, childhood abuse (CA), sexual risk behaviors, alcohol use, depressive symptoms, and self-reported STI diagnosis. Multivariate logistic regression analyses were used to examine factors associated with STI diagnosis. Among 400 participants, 84 (21%) had ever experienced at least one type of IPV in the past year. IPV, CA, age at first sex, multiple sexual partners, and alcohol use were significantly associated with STI-positive. Women who reported IPV (OR = 2.65, 95% CI = 1.11–6.28), experienced CA (OR = 5.59, 95% CI = 1.08–28.99), and had multiple sexual partners (OR = 1.39, 95% CI = 1.08–1.79) were significantly more likely to have an STI. Incorporation of IPV screening into general STIs screening is needed for this population to prevent and decrease IPV and STI consequences. Further research is also needed to understand the pathways linking IPV and STI risk to optimize the design of effective prevention interventions.
Introduction
Intimate partner violence (IPV) is a serious global health problem that adversely affects the health of women. It is one of the most pervasive human right abuses, and it affects one in every three women worldwide. 1 Although IPV is often associated with overt physical violence, it may manifest as coercive control by an intimate partner or ex-partner that includes a range of abusive behaviors, such as physical aggression, sexual coercion, psychological abuse and controlling behaviors. 1 Prevalence rates of IPV vary by country. For example, Devries et al. 2 found the lowest rates of IPV in East Asia (16.3%) and the highest rates in Central Sub-Saharan Africa (65.6%). However, prevalence of IPV has been estimated to be higher in clinical settings than in the general population, 3 because many survivors have to seek services due to injury. Specifically, researchers studying sexually transmitted infection and family planning clinic populations have documented IPV rates up to and greater than 50%. 4 , 5
Sexually transmitted infections (STIs) are infections that commonly spread by sexual behaviors. In Thailand, the prevalence of STIs has been increasing. The prevalence rate of STIs in 2005, 2010, and 2015 were 24.78, 40.87, and 61.02 per 100,000 population with gonorrhea and syphilis being the most prevalent. 6 Given the high IPV prevalence and STIs in clinical settings, there is strong evidence to indicate that women who experienced IPV have increased odds of having a history of STI. 7 , 8 The association between IPV and STIs has been studied in a range of settings, with different samples, and using a variety of measurements. However, the majority of studies come from developed country settings; 4 , 7 , 8 there is a dearth of evidence from Thailand.
The association between IPV and STIs may be explained by the fact that individuals with increased rates of IPV are often the same individuals at risk for STIs. 4 , 7 , 8 Evidence has been suggested bio-psycho-social factors related to STIs may include IPV, a history of childhood abuse (CA), sexual risk behaviors, alcohol and drug use, and mental health problems that result in female disempowerment and marginalization. 1 , 2 For example, Reza et al. 9 found that girls and young women (aged 13 to 24 years) who reported childhood sexual abuse (CSA) had an increased odds of reporting an STI compared with those who did not report chilhood sexual abuse (aOR = 3.69, 95% CI = 1.78–7.66). In addition, women who experienced IPV were found to be three and a half times more likely to have an STI as compared to women without a history of violence (OR = 3.50, 95% CI = 1.94–6.32). 10
IPV has been linked with higher levels of sexual risk behaviors, including early onset sexual activity, forced unprotected sex, and increased substance use. 8 , 11 , 12 Studies have shown that abused women are more likely to have multiple sexual partners and less likely to use condoms, thus putting them at increased risk for STIs. 13 , 14 Furthermore, alcohol use before or during sex has been shown to be a potential risk factor of HIV/STI transmission and acquisition. Even at lower amounts, alcohol consumption has been shown to increase the likelihood of unprotected sex and other risk behaviors. 15 Despite this, research on sexual risk behaviors and alcohol use associated with of STIs has not been explored among Thai women.
Numerous papers in the literature investigated associations between STIs and depressive disorders. 7 , 11 , 16 While STIs is risk factors for depression, depression may increase susceptibility to STIs and risk behaviors. For example, a recent population-based cohort study has explored the effect of depressive disorder on STIs, and found that depression increased the risk of subsequent newly diagnosed STIs in Taiwan patients (HR = 1.54, 95% CI = 1.34–1.76). 17 Additionally, among HIV-positive women, those who used drugs or alcohol had significantly worse depressive symptoms compared to those who did not use drugs or alcohol. 7 , 18 Overall, it seems likely that these variables can act as mutual risk factors associated with STIs that need for further investigation. Therefore, this study aimed to (1) examine the prevalence of IPV and (2) identify factors associated with STI diagnosis among Thai women attending gynecology clinics. Research on these relationships may help to uncover existing gaps in our knowledge and offer direction for urgently needed STI prevention and interventions in Thailand.
Methods
Study design and population
Data for this analysis came from a larger study titled “The Patterns of Casual Relationship of STIs among Women Attending Gynecology Clinics”. A cross-sectional design was used to examine factors associated with STI diagnosis. In the larger study, the sample was classified by diagnosis types (e.g., benign tumors, STIs, and HIV). The diagnosis types were stratified to ensure an equal number of samples across each group (n = 133 from each). The participants were patients attending two gynecology clinics (the GYN and STI clinics), located at a university hospital in Bangkok, Thailand. Participants had to: (1) be aged 15–49 years old; (2) be informed about STI diagnosis by the physician (for new cases); and (3) to have received counseling by a staff nurse at first visit from each clinic, respectively. Women were excluded if they have not ever engaged in a sexual relationship, reported current mental ill health (e.g., schizophrenia, bipolar disorder, and depressive disorder) or were presently taking antipsychotic medication, and were in the presence of their partners or other family members.
The Institutional Review Boards at Faculty of Medicine Siriraj Hospital, Mahidol University approved this study. A staff nurse at each clinic reviewed participants’ medical records to identify eligible women for the study. Patients who were interested in participating were invited in person by investigators who were trained regarding IPV and mental health counseling. Verbal consent was obtained from each respondent (18 years and older) before administering the questionnaire. 19 In case younger than 18 years, the consent was obtained from both participants and their guardians. However, the participant herself had the opportunity to either withdraw from the study or not to answer the questionnaires. Serial code numbers instead of participants’ names were used on each questionnaire. Confidentiality of collected data was maintained throughout the study.
Study measures
Sociodemographic characteristics
Age, education, income, and career were reported separately by participants and partners. Marital status, length of marriage, and number of marriage were also obtained by questionnaires.
Intimate partner violence (IPV)
Experiences of IPV were measured by the Abuse Assessment Screen (AAS). 20 For the purpose of this study, participants answered the modified AAS questions which included: (1) “Within the last year, have you ever been hit, slapped, kicked, or otherwise physically hurt by your partner?”; (2) “Within the last year, has your partner forced you to have sexual intercourse even when you didn’t want to?”; and (3) “Within the last year, have you ever been emotionally hurt, threatened, humiliated, or controlled by your partner?”. A positive answer to any one of these behaviors was considered to have experienced IPV (coded 1 = yes; coded 0 = no).
Childhood abuse (CA)
Participants who reported physical or sexual abuse before age 15 were considered to have experienced CA (coded 1 = yes; coded 0 = no).
Sexual risk behaviors
Participants were asked about age at first sex and number of sexual partners in their lifetime. Multiple partners was defined as having 2 or more lifetime partners (coded 1; coded 0 = single sexual partner).
Alcohol use
Using two questions assessed drinking behavior in the past month for participants and their partners: (1) “Have you ever had a drink in the past month?” and (2) “Have your partner ever had a drink in the past month?”. Responses from either participant or partner were classified as having alcohol use (coded 1) or not having alcohol use (coded 0) in the past month.
Depressive symptoms
The Center for Epidemiologic Studies Depression Scale (CES-D) is a 20-item self-report scale intended to assess depressive symptoms in the general population. 21 Items were answered on a 4-point Likert-type scale ranging from 0 rarely/none of the time to 3 most/all of the time in the past week (Cronbach’s alpha 0.91 for the present sample). A higher score indicated more depressive symptoms. The total scores range from 0 to 60, and a cutoff score of 16 or above is considered depressed.
Self-reported STI diagnosis
History of STI diagnosis in the past 12 months was self-reported via a single item: “Have you had any sexually transmitted infection or other diagnoses as listed?”. A yes response of at least one infection of condyloma, syphilis, herpes, hepatitis B, or HIV (top five diseases in STD clinic) was categorized as STI-positive (coded 1), while an incident of myoma uteri, endometriosis, or dysfunctional uterine bleeding (DUB) (top 3 diseases in GYN clinic) was categorized as STI-negative (coded 0). Although participants were asked to complete a set of questionnaire in a counseling room at each clinic for privacy reasons, patients’ medical records were accessed by research team staff to confirm the diagnosis.
Statistical analyses
All analyses were conducted using SPSS version 18 (SPSS Inc, Chicago, Illinois). Descriptive statistics were used to characterize the sample. Bivariate analyses and Fisher’s exact tests were used to assess the relationship between variables of interest and STI diagnosis. Multivariate logistic regression analyses were utilized to assess the associations between risk factors and STI diagnosis, controlling for variables that were significantly associated with STIs in the bivariate analyses.
Results
A total of 429 participants were recruited. Of these, 29 participants were excluded from the study due to inconvenience (93.2% response rate). Women’ mean age was 36.42 years (SD = 9.46, range 17–49 years), whereas partners’ mean age was 39.42 years (SD = 11.14, range 15–72 years). About 35% of participants were between 36–45 years, while 17% of partners were between 15–25 years. 52.2% of participants were married with a mean length of marriage of 8.60 years (SD = 8.10). Almost 44% of participants and 34% of partners attended graduate education. Most participants and partners were employed. About one third of couples reported that their monthly incomes were less than 10,000 Thai baht ($323) which is below the national average income. About 21% of participants (n = 84) reported experiencing at least one type of IPV from their partners in the past year. The prevalence of childhood physical or sexual abuse was 9.5% (n = 38). The mean age at first sex and number of sexual partners were 20.34 years (SD = 4.55) and 3.24 (SD = 6.62), respectively. Partners’ alcohol use in the past month (60.8%; n = 243) was found to be higher than participants’ alcohol use (40.5%; n = 162). About 38.3% of participants (n = 153) met the cutoff for depressive symptoms.
Sociodemographic characteristics by STI diagnosis (n = 400).
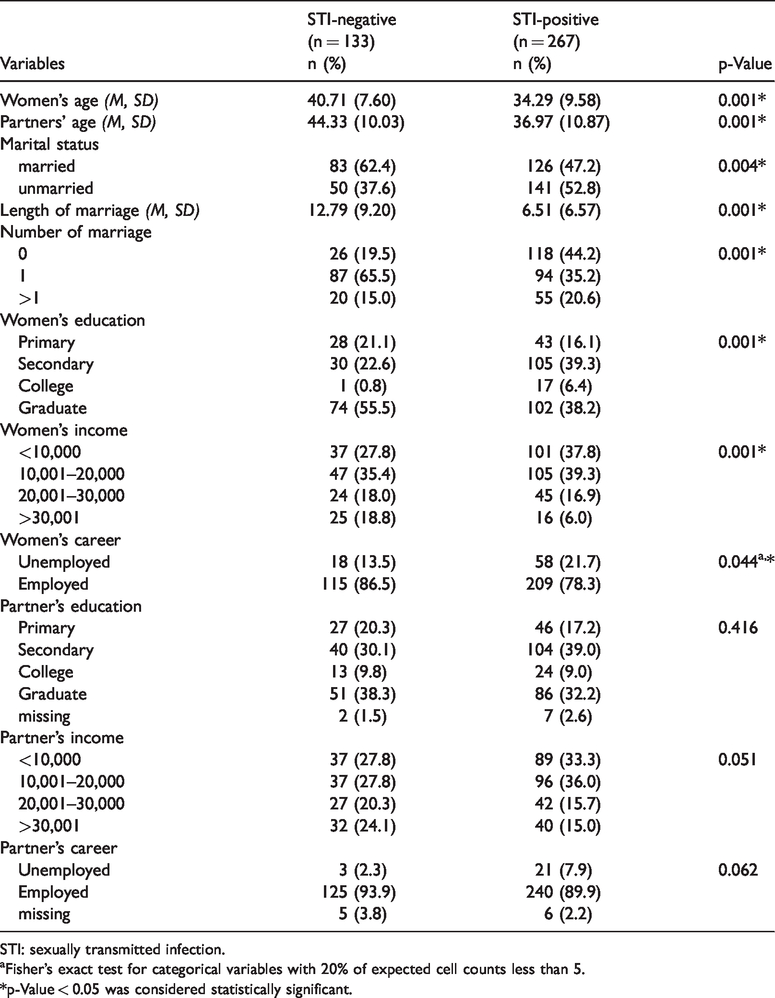
STI: sexually transmitted infection.
Fisher’s exact test for categorical variables with 20% of expected cell counts less than 5.
*p-Value < 0.05 was considered statistically significant.
Predictor variables by STI diagnosis (n = 400).

STI: sexually transmitted infection; IPV: intimate partner violence; CA: childhood abuse.
Fisher’s exact test for categorical variables with 20% of expected cell counts less than 5.
*p-Value < 0.05 was considered statistically significant.
Multivariable logistic regression of predictors of STI-positive status among Thai women attending gynecology clinics (n = 400).
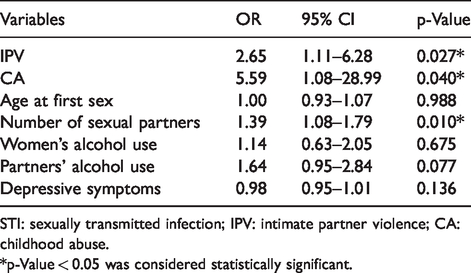
STI: sexually transmitted infection; IPV: intimate partner violence; CA: childhood abuse.
*p-Value < 0.05 was considered statistically significant.
Discussion
To our knowledge, this is the first study to investigate the prevalence of IPV and identify factors associated with STI diagnosis among a sample of Thai women attending gynecology clinics. Although the prevalence rate in this study (21%) was not as high as those found in the U.S. (38% 7 and 32% 12 ), our finding indicated that IPV commonly occurred among Thai female patients. This low prevalence rate may reflect that IPV is viewed as a private matter within the family. 22 Victims of IPV may keep silent and face a substantial amount of shame and stigma, making it difficult for them to seek help from outsiders until their health or overall situation becomes severe. 23 As a result, IPV might undermine a woman’s ability to access health care services and disclose the abuse to someone. In practice, though, few clinical settings in Thailand support routine screening or assessment for IPV, and most Thai providers do not screen for IPV. Additionally, STIs are often asymptomatic or present with mild symptoms, making them difficult to diagnose and treat. Thus, incorporation of IPV screening into general STI screening is needed for this vulnerable population to decrease or prevent IPV. Importantly, policies must be developed or strengthened that IPV screening in clinical settings should be implemented and should include the training of medical and nursing professionals to address patients’ experiences with IPV in their clinical encounters. Thai providers should offer empathetic support as required and be familiar with appropriate places for referring those revealing IPV. Domestic violence shelters, One Stop Crisis Center (OSCC), a social worker, or a psychiatrist may be appropriate options depending upon the patient’s needs.
Consistent to previous studies, 11 – 13 we found that IPV was associated with STIs. Notably, 28% of those who reported IPV tested positive for an STI, which equated to over 2.6 times increase in the odds. A possible explanation for this association could relate to the underlying balance of power. Evidence suggests that women are more vulnerable to STIs partly because of deep-rooted gender inequalities and violence. 24 The male-dominant culture may limit a woman’s ability to negotiate safe sex in an intimate partner relationship and an attempt to negotiate may even incite violence, thereby increasing women’s risk of STIs. 25 IPV has been identified as reducing the ability of women to protect and control their reproductive and sexual health. Given the connection of IPV with increased sexual risk behaviors, women with multiple sexual partners may be at increased risk of STIs, through their partners’ risky behaviors. Thus, interventions that encourage couple communication and shared decision making may be a promising strategy for changing views about equality in marriage and promoting negotiation.
Consistent with data from Reza et al., 9 exposure to abuse during childhood that occurred several years ago may be under-reported and increased the risk of STIs. It is possible that victims of CA may respond to IPV with learned helplessness, 26 resulting in a potential of victimization in adulthood. Learned helplessness may lead to low self-esteem and difficulties with problem solving. Consequently, women who experienced CA may engage in sexual risk behaviors as a coping mechanism. 27 In a busy clinical setting, our suggestion is to offer a prompt referral to an in-house social worker who can then discuss the problem in depth. The social worker may offer further support and can refer to local support services as required. Thus, efforts to prevent CA remain of paramount importance in Thailand because women may accept violence and develop maladaptive coping strategies during childhood and adolescent periods.
Unlike other studies, age at first sex was not a significant predictor of STIs. This may because the mean age of women in this study was higher than in the U.S. studies. 7 , 12 It is possible that young age at marriage has been correlated with IPV and other dimensions of limited relationship power, resulting in risk of IPV and STIs. 28 Several studies have reported an association between alcohol use and STIs; 7 , 11 , 29 however, our study did not find any significant trend. One reason for this is socio-cultural norms, such as the belief that female drinkers are not acceptable in Thai society. Although the percentage of women’s alcohol use in this study was lower than partners’ alcohol use, it is currently unknown whether the relationship between alcohol consumption and partner’s aggressive behaviors impacts on women’s sexual health outcomes. Further research is needed to identify the mechanisms by which alcohol contributes to both IPV and STIs. The more we know about how alcohol affects IPV and STIs, the better able we will be to develop effective prevention strategies.
Although the mean score of CES-D in the STI-positive group were higher than those in the STI-negative group, it was not statistically significant. It is possible that only 38.3% of women in this study exhibited depressive symptoms, which is lower prevalence rate as compared to Illangasekare et al. (73%). 30 A possible explanation may because staff nurses at gynecology clinics routinely provide counseling with patients on a variety of psychosocial and health problems. Therefore, higher level of mental health problems (e.g., fear, anxiety, or stress) may reduce at first visit and follow up. Although depressive symptoms did not predict an incidence of STI, it can impact women’s mental health. Screening for depressive symptoms at gynecological visits might help prevent at-risk women for experiencing more severe outcomes.
This study had several limitations. First, our findings were limited by the fact that we conducted a cross-sectional analysis and were unable to determine when the IPV started. Second, this study relied on the self-report approach, which may have introduced bias, likely from under-reporting. Third, the time frame for reported IPV was limited within the past year. However, the IPV might not have been happening concurrently with the acquisition of the STI. Fourth, the small sample size prohibited the examination of interaction effects and resulted in large confidence intervals. To increase precision, larger studies, preferably using multi-center sites, are recommended. Finally, the single-item measure of alcohol use may have reduced response severity of drinking; future studies should consider using the 10 question AUDIT (Alcohol Use Disorders Identification Test).
Conclusion
Given that women who were abused are at increased risk of STIs, screening of IPV should be assessed among female patients of gynecology clinics because these are unique opportunities to consistently contact women at risk. Training health care providers to ask appropriate IPV screening questions and give counseling to establish links between patients and support services may be an effective intervention to reduce the burden of IPV. Reproductive health care providers must be aware of factors associated with STIs among female patients, and address these associations as part of comprehensive treatment. Further research is needed to understand the pathways linking IPV and STI to optimize the design of effective interventions.
Footnotes
Authors’ contributions
All authors made substantial contributions to development, study design and data analysis plan. NT and PR recruited and collected the data. NT and NV analyzed and interpreted the data. NT has been involved in drafting and revising the manuscript. NT and NV critically reviewed the manuscript and finalized it prior to submission. All authors read and approved the final manuscript.
Acknowledgements
The authors would like to thank the nurses and staff members from gynecology clinics at Siriraj Hospital for their support and to the women who participated in the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was supported by China Medical Board of New York, Inc., Faculty of Nursing, Mahidol University.