
Abstract
A 20-year-old young woman with cauliflower-shaped lesions on her vulva was misdiagnosed as condyloma acuminatum. Further evaluation revealed positive serological tests for syphilis. On histological examination, and numerous plasma cells were seen to infiltrate the dermis heavily. The cauliflower-shaped lesions on vulva completely disappeared after benzathine penicillin treatment. Cauliflower-shaped lesions are a rare manifestation of secondary syphilis.
Keywords
Introduction
Syphilis is a sexually transmitted disease that results from infection with the spirochete, Treponema pallidum (TP); this condition is diagnosed frequently and is endemic in lower income regions of the world. 1 The medical literature includes descriptions of the numerous and complex cutaneous manifestations of secondary syphilis. 2 However, physicians who are unaware of its protean manifestations may easily misdiagnose secondary syphilis as another unrelated skin disorder. We report the case of a young woman with secondary syphilis in the absence of coinfection with human immunodeficiency virus (HIV) that presented with cauliflower-shaped vulvar lesions that were initially misdiagnosed as condyloma acuminatum.
Case report
A 20-year-old young woman presented to the gynecological department of our hospital with a six-month history of cauliflower-shaped lesions on her vulva that were increasing in size and number during this time. She denied any personal or family history of warts and reported no other skin lesions, dysuria, or systemic symptoms. She did report a positive sexual history with one man prior to the appearance of the cauliflower-shaped lesions. The gynecologist recommended a biopsy of the lesions that were on the left side of the vulva; this procedure did not result in a definitive diagnosis. The patient was referred to the dermatology department for further evaluation and treatment.
The patient presented to the dermatology department with large exophytic lesions involving both labia majora that extended anteriorly to the mons pubis and posteriorly to the perineum. The results of a 5% acetic acid test suggested an initial clinical diagnosis of condyloma acuminatum. The dermatologist recommended removal of the lesions using liquid nitrogen cryotherapy. The patient did not comply with treatment plans for reasons unknown and returned three days later for evaluation by a second dermatologist.
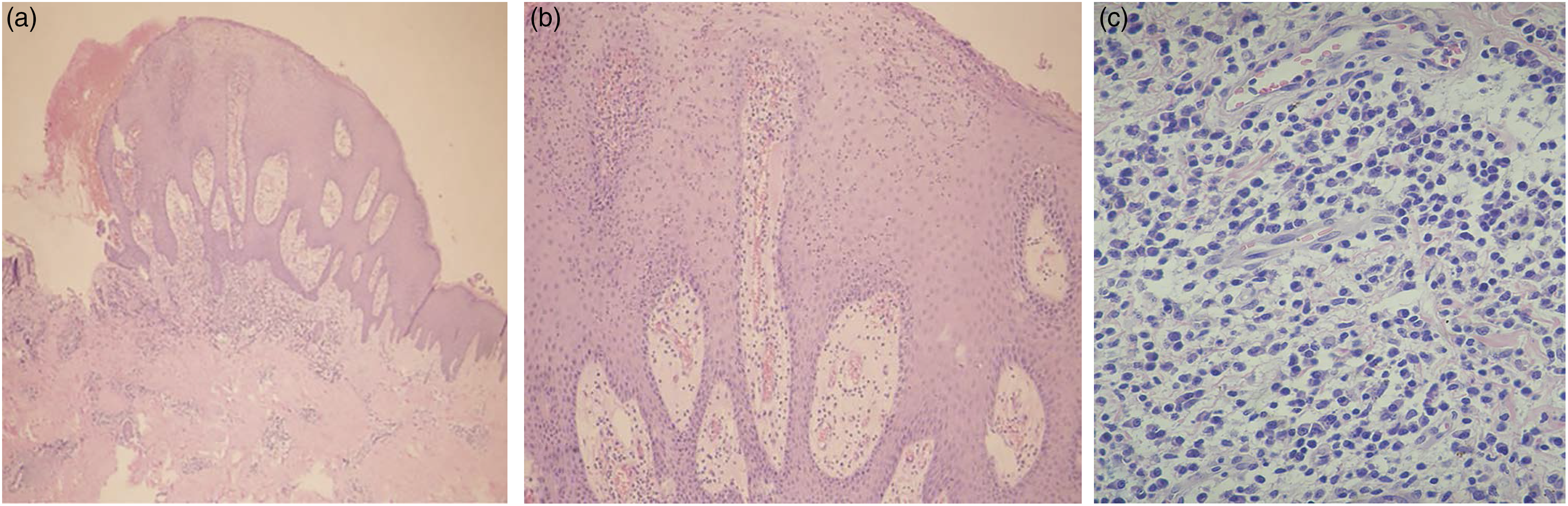
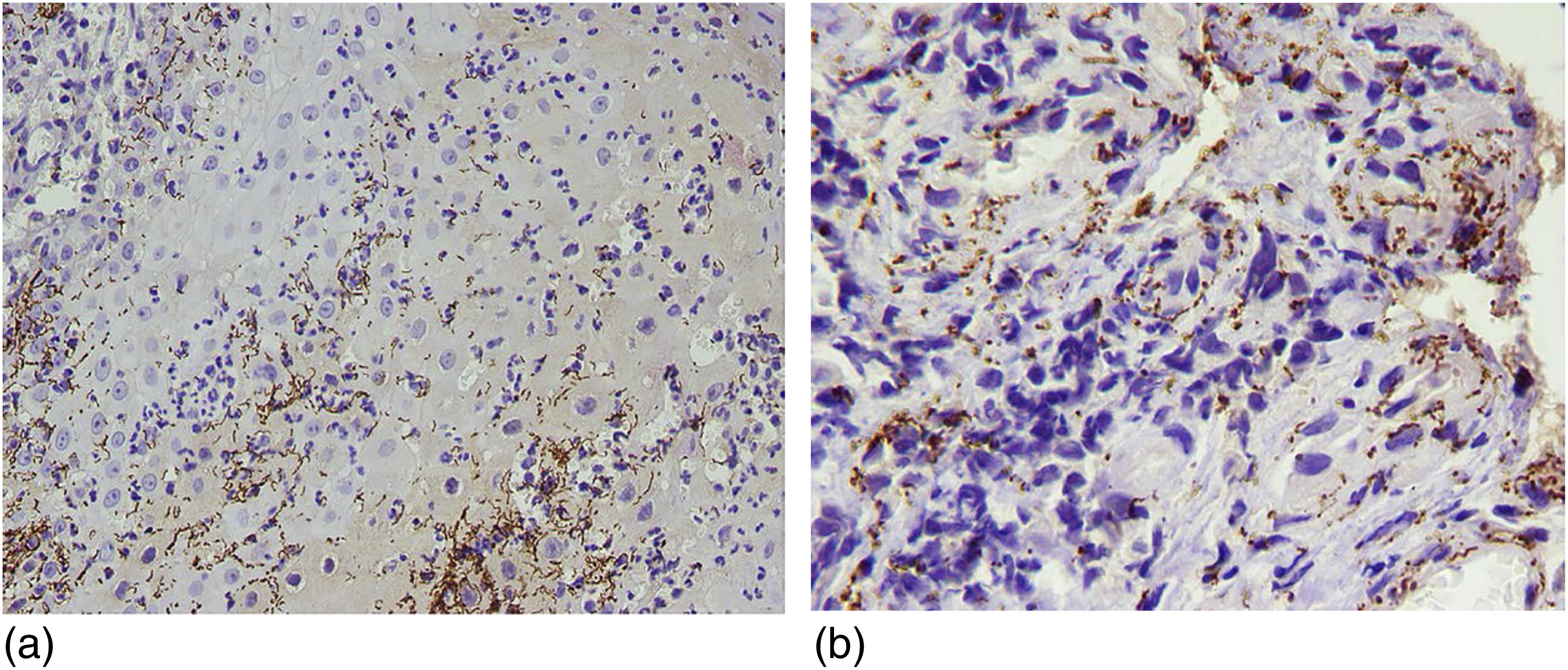
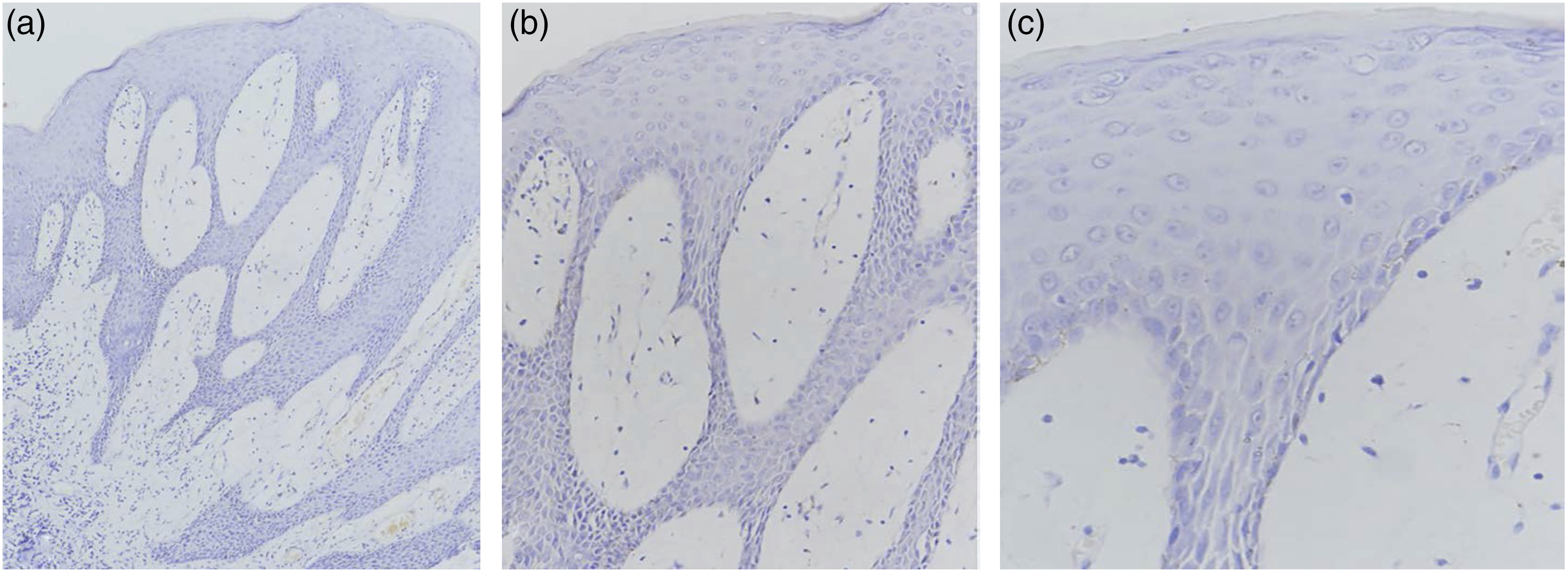
At the second consultation, the dermatologist carefully evaluated the vulva and identified many flat, granular papules (Figure 1(a) (blue circle)) of up to 1–2 mm in diameter among the cauliflower-shaped lesions. Although flat, granular papules or plaques are typically identified on the mucous membranes in association with condyloma acuminatum, they may spread to the rectal mucosa, the vagina, and/or the urethra. We reviewed the histopathological sections carefully and identified irregular epidermal hyperplasia with neutrophil infiltration; no koilocytes were detected (Figure 2(a)). These results suggested that the initial diagnosis of condyloma acuminatum might not be correct. We also identified telangiectasia and heavy infiltration of the dermis with plasma cells (Figure 2(b) and (c)). The immunohistochemistry (IHC) for the identification and localization of the TP in the specimen was performed using rabbit polyclonal anti-TP antibody (Abcam, the USA). The IHC result showed that the brown, linear TP were predominantly found in the epidermis and superficial of dermis (Figure 3(a) and (b)). However, we did not preserve the fresh vulvar tissue in −80°C and coinfection of HPV and TP could not be ruled out. Therefore, we conducted an IHC examination for the detection of HPV-6 and -11, which is significantly associated with higher risk of condylomata acuminata, to explore the HPV infection of vulvar lesions on 5-μm formalin-fixed paraffin-embedded tissue sections. An anti-HPV antibody, a mouse monoclonal antibody (BPV-1/1H8+CAMVIR, Abcam, the USA) that was described by the previous literature, was used to detect HPV types 1, 6, 11, 16, 18, and 31 in formalin-fixed paraffin-embedded tissue.
3
A negative staining result of HPV-1, -6, -11, -16, -18, and -33 was found (Figure 4(a) to (c)), and we completely ruled out the presence of HPV infection. Taken together, the results of our evaluation, which included the specific morphology of the vulvar lesions, the history of recent sexual intercourse, and results from the pathology specimens all suggested the diagnosis of atypical secondary syphilis. Further evaluation, including serology, revealed a reactive toluidine red unheated serum test (TRUST) with a titer of 1:256, positive Treponema pallidum particle agglutination (TPPA), and a negative test for HIV. We were unable to determine the results of TRUST, TPPA, and HIV tests from her sexual partner as they were no longer in contact with one another. She was treated with oral prednisone (10 mg, three times a day for three days) followed by intramuscular injection of benzathine penicillin G (2.4 MU once per week for three weeks) (25 March 2019; 1 April 2019; 8 April 2019). The cauliflower-shaped lesions were nearly gone when evaluated four days after the second dose of benzathine penicillin G (Figure 1(b). 5 April 2019) and disappeared completely at ten days after the final dose (Figure 1(c). 18 April 2019). There was no recurrence of the vulval lesions at 58 days after the final dose; the repeat serology revealed a decrease in TRUST titer from positive at 1:256 to positive at 1:8 (Figure 1(d). 6 June 2019). At the time of this case report, the patient was still undergoing follow-up and has remained symptom-free. (a) Many cauliflower-shaped lesions on the vulva and flat, granular papules of up to 1–2 mm in diameter among the lesions in the blue circle (21 March 2019). (b) Cauliflower-shaped lesions almost disappeared 4 days later since the second intramuscular injection of benzathine penicillin G (5 April 2019). (c) Cauliflower-shaped lesions disappeared completely 10 days after the last intramuscular injection of benzathine penicillin G (18 April 2019). (d) Cauliflower-shaped lesions disappeared completely 58 days after the last intramuscular injection of benzathine penicillin G (6 June 2019). (a) H&E demonstrated irregular epidermal hyperplasia with neutrophil cell infiltration and no koilocyte was observed (2*10). (b) Telangiectasia in the dermis and numerous plasma cells have been shown to infiltrate the dermis heavily (4*10). (c) Telangiectasia in dermis and numerous plasma cells have been shown to infiltrate the dermis heavily (40*10). (a) IHC examination of the lesion showing the brown, linear TP predominantly located at the epidermis and superficial of the dermis (SP, a: ×400). (b) IHC examination of the lesion showing the brown, linear TP predominantly located at the epidermis and superficial of the dermis (SP, b: ×1000). IHC: immunohistochemistry; TP: Treponema pallidum. (a) Negative staining result of HPV-1, -6, -11, -16, -18, and -33 were found in formalin-fixed paraffin-embedded tissue (SP, a: ×100). (b) Negative staining result of HPV-1, -6, -11, -16, -18, and -33 were found in formalin-fixed paraffin-embedded tissue (SP, b: ×200). (c) Negative staining result of HPV-1, -6, -11, -16, -18, and -33 were found in formalin-fixed paraffin-embedded tissue (SP, c: ×400).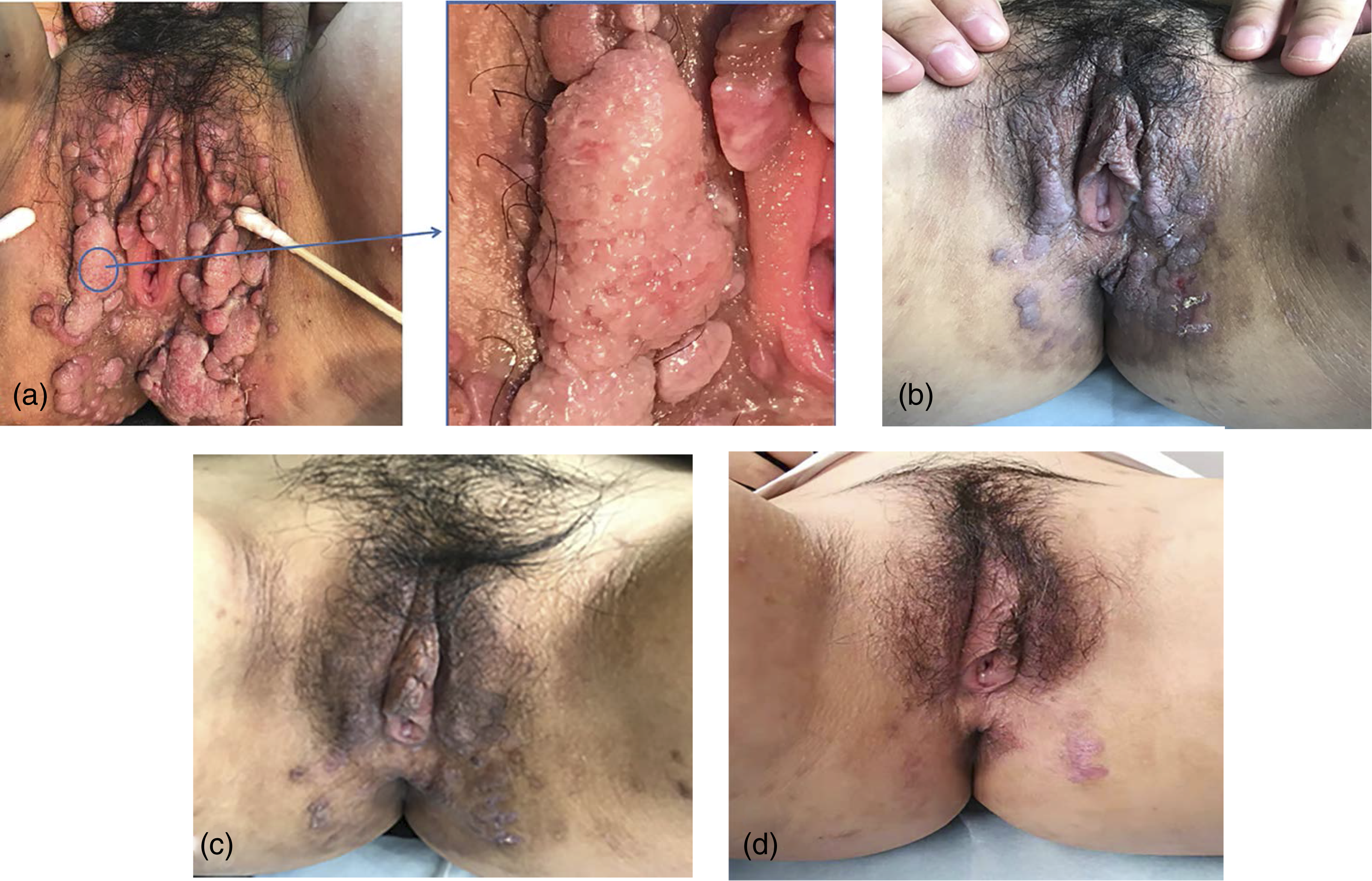
Discussion
Secondary syphilis has been called “the great imitator” as it can present with a diverse array of cutaneous manifestations. Maculopapular eruptions on the trunk or limbs are among the most common patterns of secondary syphilis. 4 Similarly, the condition known as condylomata lata has been associated with secondary syphilis and is typically identified as a smooth, flat rash located on the genitalia and the anus. 5 However, many atypical genital and anal lesions that are characteristic of secondary syphilis can mimic other skin diseases including scrotal eczema, 6 Behçet’s disease, 7 and genital filariasis. 8 Our patient reported a six-month history of cauliflower-shaped vulvar lesions; the differential diagnosis for lesions of this type includes condyloma acuminatum, condylomata lata, squamous cell carcinoma, basal cell carcinoma, and verrucous carcinoma. Condyloma acuminatum is a benign form of mucosal hyperplasia typically detected in the genital and perianal regions that results from infection with human papilloma virus. 9 The main clinical manifestations of these lesions are pink papules or cauliflower-shaped lesions typically 1 mm–1 cm in diameter that bleed easily in response to minor trauma. The large or flat lesions characteristic of condyloma acuminatum can also be identified with practice; the 5% acetic acid test is a helpful method that may provide an accurate diagnosis. However, the full specificity of this diagnostic maneuver has not been ascertained; some tumors will generate positive results with this test. 10 As such, dermatologists may misdiagnose other skin diseases as condyloma acuminatum if they are relying on clinical manifestations and results of the 5% acetic acid test alone.
The pathological characteristics of secondary syphilis are complex and multifaceted. However, plasma cell infiltrates in the dermis are an important pathological clue for the diagnosis of secondary syphilis in clinical practice. 11 It is also important to recognize that the histopathological examination of condyloma acuminatum typically reveals epidermal acanthosis; a high-power view will be notable for vacuolated keratinocytes and koilocytes in the upper layers of the epidermis. 12 The histopathological results in this case included numerous plasma cell infiltrates within the dermis; no koilocytes were detected. This provided a critical diagnostic clue and suggested to us that the vulvar lesions might be manifestations of atypical secondary syphilis; a serology test ultimately verified this diagnosis. Of note, the histopathological findings combined with the results of serology testing provided us with confirmation of the diagnosis of secondary syphilis; silver staining and immunofluorescent techniques to identify spirochetes were deemed unnecessary.
To the best of our knowledge, this is the first case report of secondary syphilis in a young woman with cauliflower-shaped vulvar lesions that were initially suggestive of condyloma acuminatum. The plasma cell infiltrates in the dermis detected in stained histopathological sections represented an important clue that suggested that these findings could be manifestations of atypical secondary syphilis. This case revealed the importance of histopathological examination when considering a diagnosis of atypical syphilis. To summarize, careful physical, histopathological, and serological examinations are required in order to diagnose secondary syphilis due to the atypical manifestations associated with this disease. Furthermore, this case warns us the STD-related serological screening should be performed in the management of STDs by the dermatologist.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.