
Abstract
Patient demand on sexual health services in the United Kingdom is so high that many services have introduced online screening to accommodate more patients. There are concerns that these services may not be accessible to all. This service evaluation was undertaken to determine whether online screening is accessible by those patients most at need by comparing the demographics and number of asymptomatic chlamydial infections detected online and in clinic. No difference was found in the age nor level of deprivation, demonstrating that online services are an accessible way to screen for sexually transmitted infections without overburdening established services.
Introduction
Sexual health services (SHS) in the United Kingdom are confidential and free at the point of access. 1 They are essential in preventing onward transmission of sexually transmitted infections (STIs) and in maintaining good reproductive health; 2 however, the demand for SHS continues to increase putting greater demands on service capacity. Both the British Association for Sexual Health and HIV (BASHH) and the National Institute for Health and Care Excellence guidelines recommend that patients should be able to access an appointment at SHS within two working days of contact.3,4 Recent studies have shown that access to SHS in the United Kingdom has worsened and fall short of this recommendation with only a reported 91% of patients being offered an appointment within two working days.4,5
In 2015, Hampshire became one of the first counties in the United Kingdom to offer a comprehensive county-wide online sexual health screening for asymptomatic patients. This involves clinics directing individuals to ordering an online test from the SHS’s web site to a residential postal address in the county and sending the self-taken sample to an affiliated laboratory. Users receive results via a text or telephone call. The users are required to have internet access; the facility to confidentially receive the testing kit and to be able to self-sample correctly and return their samples.
Those at higher risk of STIs include people below the age of 25 years, Black and Asian ethnic minority patients (BAME), sexual and gender minority groups and those living in deprived areas.6,7 These groups are also more likely to face barriers to access due to stigma, discrimination and low awareness of STIs and SHS. 2 Additionally, they are less likely to be health literate and proactive in self-care.8,9 Although self-taken samples are as effective as clinician taken samples, 10 previous studies have shown that younger people and BAME individuals are less likely to return their self-taken STI samples. 11 Additionally, some younger people remain concerned about the ability to receive online kits and digital communication from SHS, confidentially.12,13 Due to these requirements, it has been suggested that online testing may not be accessible to these higher risk groups. However, countered against this, there are also specific barriers related to clinic attendance such as embarrassment, fear of discrimination, intimate examinations by clinicians or the inability to physically access SHS at a given time and location, so it might be that online testing offers a more convenient way to be screened for these individuals.17,18
Studies outside the United Kingdom have demonstrated the benefits of widened access to services through online screening, particularly in men having sex with men and in rural communities.14,15 Online STI screening has become increasingly available in regions of the United Kingdom,16–18 although limited data are available on what impact this has had on access to services. 19 There has been a substantial acceleration of remote STI screening due to COVID-19 with BASHH recommending the provision of online SHS to reduce face-to-face clinic visits. 20 This retrospective service evaluation aimed to identify the differences in demographic characteristics in patients diagnosed with chlamydia infection via online testing in comparison to those diagnosed in clinics. The objective of the analysis was to determine whether online screening is accessible and utilised by those patients most at need of SHS.
Methods
This service evaluation compared the number of asymptomatic chlamydial infections within two significant periods: Time 1 – before the introduction online self-sampling STI screening (September 2014–March 2015) and Time 2 – after the introduction of self-sampling services (September 2017–March 2018). The period for Time 2 was chosen to allow for the system to be up and running in order to allow for a valid comparison so that data would not be affected by problems associated with initial logistical difficulties. Chlamydial infection was a marker due to its being the most common bacterial STI, and particularly predominant in younger people 6 in line with National Chlamydia Screening Programme. The comparison between online and in-clinic SHS was based on online STI self-sampling offered to the residents of Hampshire, UK, through Solent NHS Trust ‘www.letstalkaboutit.nhs.uk’ portal since March 2015.
The sexual health electronic patient records of service users from Solent NHS Trust were used for data collection. Differences in patient demographics (i.e. age, gender, sexual orientation, ethnicity and postcodes (as a measure of deprivation using the UK Index of Multiple Deprivation) and case management between in-clinic and online service users were investigated. These variables were dichotomised to perform chi-square test on all variables.
A further in-depth analysis of the case management of a randomised selection of 100 patients in two comparison groups in Time 2, clinic diagnosed patients and online diagnosed patients, was completed. The records were individually analysed with their case management in detail in order to establish time between testing and treatment and the number of episodes of treatment. Where data were not recorded or incorrectly coded, individual data were excluded and subsequently substituted for the next randomised case. The University of Southampton Ethics and Research Committee approved this service evaluation (ERGO Number: 45657).
Results
Demographics of patients diagnosed with chlamydial infection, comparing before and after online testing was introduced.

BAME: Black and Asian minority ethnic; OR: odds ratio; CI: confidence interval; ref: reference category. *Significant at p < 0.05. The first OR (95% CI) column represents the comparison between clinic diagnoses when comparing before and after online testing introduction. The second OR (95% CI) column represents the comparison between clinic and online diagnoses since online testing introduction.
Case management of patients diagnosed with chlamydial infection after online testing was introduced (September 2017–March 2018), comparing clinic and online.
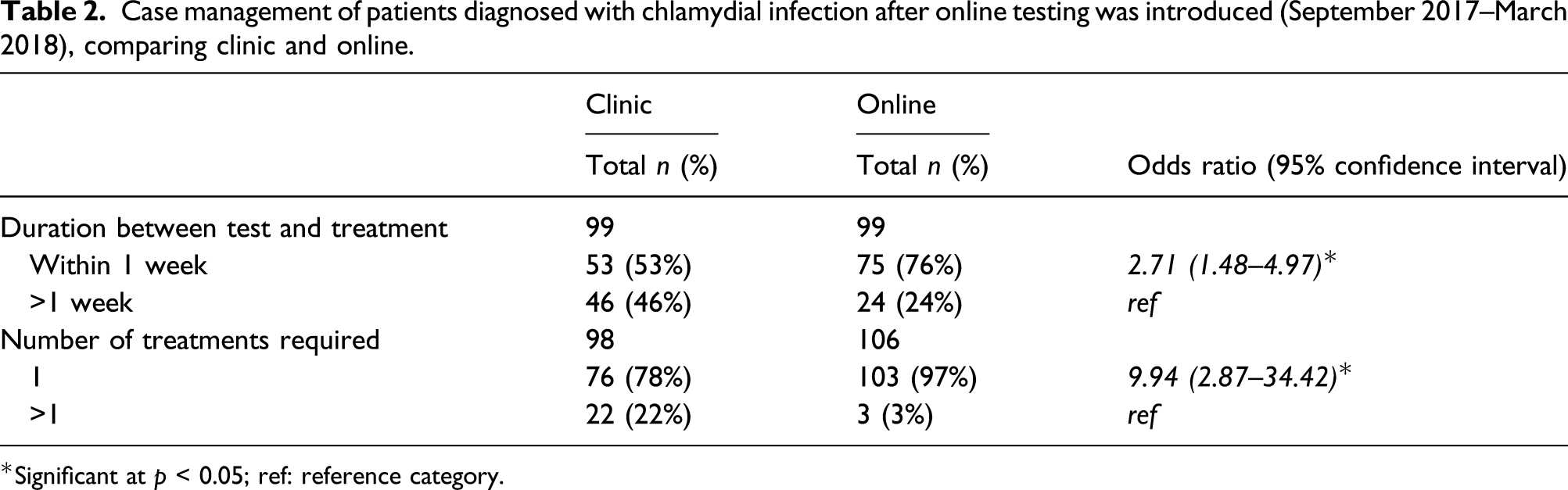
*Significant at p < 0.05; ref: reference category.
The analysis demonstrated no difference in the number of individuals living in an area of deprivation nor of gender between those diagnosed with before and after online testing was introduced within the two time periods. However, there was a significantly greater number of patients who were non-heterosexual (i.e. self-identifying as gay, bisexual or men who have sex with men) and of BAME ethnicity.
The patients diagnosed with chlamydial infection online were significantly more likely to be women, non-heterosexual and of white ethnic identity than those individuals who were diagnosed in clinic. There was no significant difference in the age or level of deprivation between those diagnosed in clinic service compared to those diagnosed via the online service. Additionally, patients diagnosed in clinic were significantly more likely to wait more than a week for treatment than those diagnosed through online services (76% vs. 53%, respectively, OR 9.94 CI 2.87–34.42) and were more likely to need retreatment (22% vs. 3%, respectively, OR 2.71 CI 1.48–4.97).
Discussion
This service evaluation compared the characteristics of individuals diagnosed with chlamydial infection before and after online STI screening was introduced and secondly the characteristics of those having online testing versus those who opted for in-person testing. This study found that women and non-heterosexuals were more likely to be diagnosed by online screening and that those individuals who were tested online received treatment faster and were less likely to require retreatment. There was no difference in the age or level of deprivation between those diagnosed in clinic service compared to those diagnosed via the online service. The concerns that online testing is not accessible to younger people or those from deprived areas are not supported by this study.
It is of notable significance that this study found that those diagnosed with chlamydial infection online received treatment sooner and were less likely to require retreatment than those diagnosed in clinic. The reason for this is unknown; it could be that the patients diagnosed online were more motivated to attend quickly and comply with treatment.
This study also found that women and non-heterosexuals were more likely to be diagnosed online than in clinic. This indicated that in these groups, online tests may be perceived as a more acceptable and accessible method of testing for STIs than in clinic. Overall, 13% of people in the United Kingdom are from BAME backgrounds, although in Hampshire where the study was conducted, this figure is only 8%. 21 The proportion of chlamydial infection diagnosed individuals of BAME ethnicity increased over the 2 years from 9% to 13%; however, they were less likely to be diagnosed via the online service. Previous research showing lower return rates of online testing kits among BAME patients could be a contributing factor. 11
The limitations of this study are firstly that there may be a proportion of undiagnosed chlamydial infection in patients who did not return their sample kits, additionally there is missing data for those patients who elected to have treatment from elsewhere. These may be the most hard to reach a group, and therefore, this study does not determine if access to these patients has been affected by the introduction of online testing. Secondly, within Hampshire, there are a large number of transient university student population who are not from deprived backgrounds but are temporarily residing in deprived city areas which may skew the analysis of deprivation.22,23 Thirdly, Hampshire has a lower proportion of minority individuals; both in sexual orientation and ethnicity than the rest of the United Kingdom, so the findings may not be transferrable to other areas or countries. Additionally, this study is limited by a small sample size regarding case management, even though a significant difference was detected.
This study demonstrates that online services are an effective and accessible alternative to screen patients for STIs without overburdening established services even in some high-risk populations such as younger individuals. However, we suggest that qualitative research is undertaken in specific demographic groups to identify any specific barriers to using online screening.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.