
Abstract
Objectives: Elvitegravir/cobicistat/emtricitabine/tenofovir alafenamide (E/C/F/TAF) is a recommended and widely used regimen for HIV infection. In this study, we aimed to determine the efficacy and safety of E/C/F/TAF in people living with HIV (PLWH), who are either treatment-naïve or switched from any tenofovir disoproxil fumarate-containing regimen. For switched patients, we aimed to determine the impact of switching from tenofovir disoproxil fumarate (TDF) to TAF on lipid profile and kidney functions. Methods: ACTHIV-IST Study Group produced a database, and five dedicated HIV centres in Istanbul entered data of PLWH who switched from any TDF-containing regimen to E/C/F/TAF and treatment-naïve patients who were initiated with the E/C/F/TAF regimen between January 2017 and December 2019. Clinical findings, viral parameters, lipid studies, renal function tests, adverse events and adherence to the treatment were recorded in this prospective observational study. Results: The study included a total of 614 switched and treatment-naïve patients. Of 430 treatment-experienced patients, 89% (382) were men, and the mean age was 42 ± 12 years. Among them, 47% (181/382) self-identified as men who have sex with men (MSM). The median duration of HIV diagnosis was 54 ± 29 months. The median duration of E/C/F/TAF use was 20 ± 36 months and that of previous treatment was 23 ± 18 months. HIV-RNA was undetectable at baseline and month 12 in 84.1% (360/428) and 86.1% (328/381) of patients, respectively (p > 0.05). Mean CD4 counts were 708 ± 287 cells/µL and 802 ± 305 cells/µL at baseline and month 12, respectively (p < 0.001). Serum creatinine levels remained stable during the treatment period. Mean total cholesterol levels at baseline and month 12 were 172 and 211 mg/dL (p < 0.01), LDL-cholesterol 104 and 138 mg/dL (p < 0.01), HDL-cholesterol 39 and 49 mg/dL (p < 0.01) and triglycerides 134 and 174 mg/dL (p < 0.01), respectively. The treatment was generally well tolerated. Eight patients discontinued the therapy (drug interaction: 3; lost to follow-up: 1; pregnancy: 1; pulmonary tuberculosis: 1; side effect: 1; patient’s decision: 1). Of 184 treatment-naïve patients, 88% (162) were men, and the mean age was 36.5± 12 years. Among them, 50% (81/162) self-identified as MSM. The mean duration of HIV infection was 21.6 ± 17.1 months. The mean duration of E/C/F/TAF use was 16 ± 4 months. HIV-RNA was undetectable at baseline and month 12 in 1% and 89.1% of patients, respectively. Mean CD4 counts at baseline and month 12 were 469 ± 223 cells/µL and 740 ± 298 cells/µL, respectively. During the treatment period, creatinine levels remained stable. Total cholesterol, LDL-cholesterol, triglyceride and also HDL-cholesterol levels increased. Mean total cholesterol levels at baseline and month 12 were 167 and 211 mg/dL (p < 0.01), LDL-cholesterol 108 and 143 mg/dL (p < 0.01), HDL-cholesterol 41 and 47 mg/dL (p < 0.01) and triglycerides 136 and 172 mg/dL, respectively (p < 0.01). The treatment was generally well tolerated. Three patients discontinued the therapy (drug interaction: 1; non-responder: 1; patient’s decision: 1). Conclusion: Starting with or switching to E/C/F/TAF in PLWH effectively suppresses HIV infection, is associated with an increase in CD4 cell count and is well tolerated in a real-life setting. Renal functions remained stable during the treatment. E/C/F/TAF use was associated with an increase in LDL-cholesterol and triglyceride levels along with an increase in HDL-cholesterol levels.
Introduction
Elvitegravir/cobicistat/emtricitabine/tenofovir alafenamide (E/C/F/TAF) combination is a recommended regimen in the current human immunodeficiency virus (HIV) treatment guidelines and is widely used in clinical practice. 1–3
Elvitegravir is an integrase strand transfer inhibitor (INSTI). INSTIs are anchor drugs for treatment-naïve patients with their high efficacy and favourable safety profiles, compared to non-nucleoside reverse transcriptase inhibitors (NNRTIs)4–6 and protease inhibitors (PIs).7–9 INSTIs show a high genetic barrier to resistance and high potency.
INSTIs are generally safe and well tolerated. In randomised clinical trials, 1–4% of the patients discontinued the therapy due to adverse effects. 10 Observational studies showed that discontinuations due to any reason tended to be less common with elvitegravir, but discontinuations due to toxicity did not differ among integrase inhibitors. Yet, neuropsychiatric toxicity leading to drug discontinuation was more frequent with dolutegravir, especially amongst women and older patients.11–16
Co-formulated E/C/F/TAF contains tenofovir alafenamide (TAF), a tenofovir prodrug with a 90% reduction in plasma tenofovir concentrations compared to the use of tenofovir disoproxil fumarate (TDF). Relatively higher rates of renal and bone toxicity are associated with high plasma tenofovir concentrations. TAF-containing regimens were shown to have advantages in renal function, bone parameters and lipid profile for treatment-naïve people living with HIV (PLWH). 17 Nevertheless, owing to the TAF component, a reduction in estimated glomerular filtration rate (eGFR) during the first 4 weeks of treatment, both in naïve and experienced patients, has been reported.8,17–21
Real-life studies are observational studies providing data about the treatment in a wider population. They determine whether the expected outcomes are obtained in routine clinical practice. They have more relaxed inclusion criteria, and exclusion criteria are not strict. 22 It is possible to see almost all scenarios in clinical practice with exposure to a large number of patients. On the other hand, real-life observational studies are often biased if they are used as an alternative to randomised trials since the balance between the groups is not ensured. 23
In this observational study, we aimed to determine the efficacy and safety of E/C/F/TAF on PLWH, who are either treatment-naïve or switched from any tenofovir disoproxil fumarate-containing regimen. For switched patients, we also aimed to determine the impact of switching from tenofovir disoproxil fumarate (TDF) to TAF on lipid profile and kidney functions.
We evaluated the clinical (patient history, physical examination, complete blood count and biochemistry), immunological (CD4 count) and virological (HIV-RNA levels) parameters of the patients.
Methods
Between January 2017 and December 2019, 614 PLWH older than 18 years of age were enrolled in this observational, prospective, multi-centre study by ACTHIV-IST (Action Against HIV in Istanbul) Study Group, which includes five centres following up PLWH in Istanbul. The first 6 months were the recruitment period.
The centres entered the data of PLHW who switched from any TDF-containing regimen to E/C/F/TAF and treatment-naïve patients who were initiated with the E/C/F/TAF regimen (Figure 1). All the patients in every centre received standard of care. Inclusion and Exclusion Criteria of the Study (PLWH: People Living with HIV; E/C/F/TAF: Elvitegravir/Cobicistat/Emtricitabine/Tenofovir Alafenamide).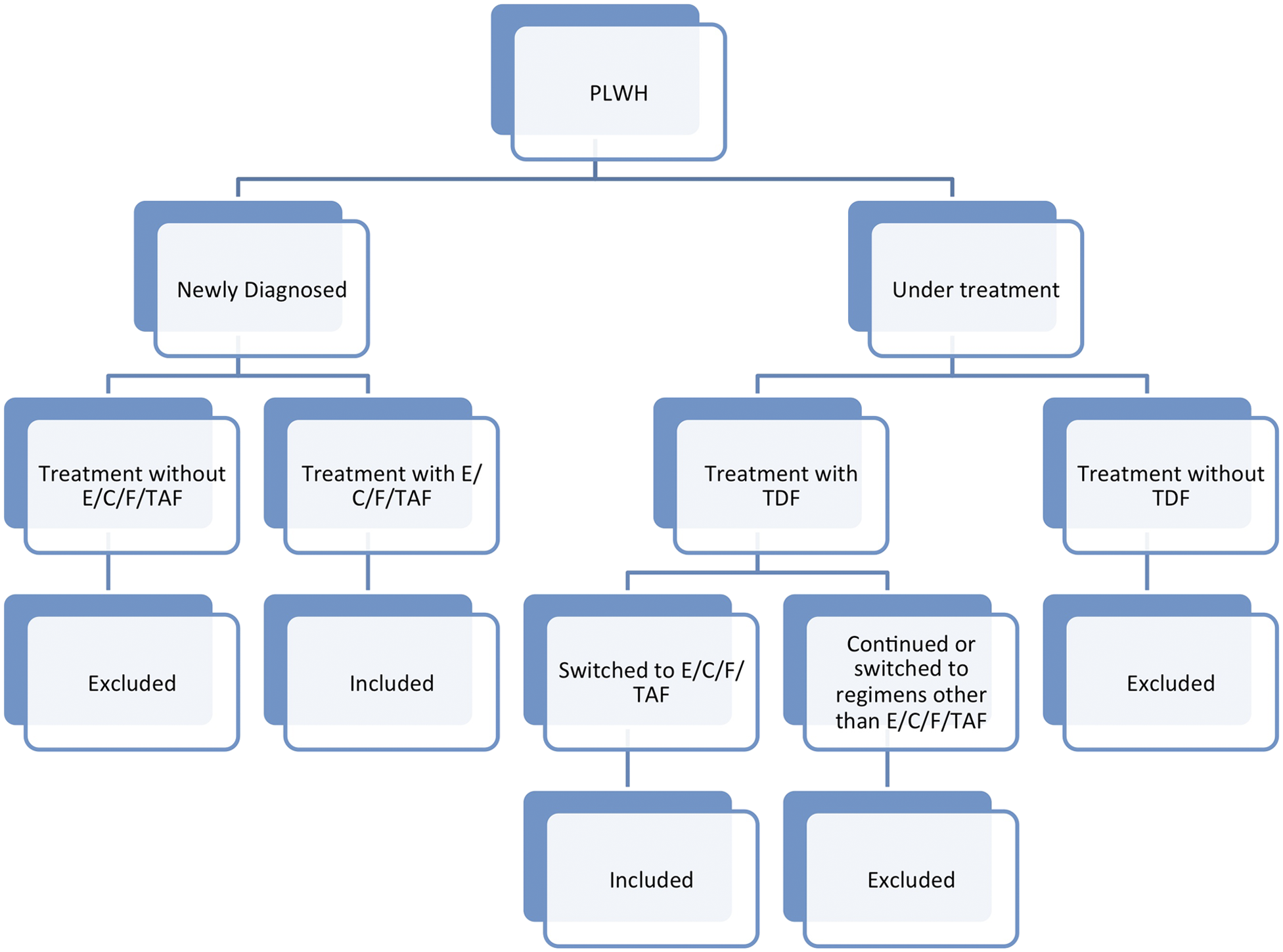
All newly diagnosed HIV/AIDS patients were confirmed by the Western Blot verification test (HIV BLOT 2.2, MP Biomedicals Asia Pacific, Singapore). The CD4+ cell counts were studied by flow cytometry (FACSCalibur, Becton Dickinson, New Jersey, USA), and HIV viral load was measured by PCR (COBAS AmpliPrep/COBAS TaqMan HIV-1 Test, Roche Molecular Systems, USA). Data on age, sex, CD4+ counts and HIV-RNA, complete blood count, renal function tests (creatinine levels and estimated glomerular filtration rate (eGFR)), lipid parameters (total cholesterol, LDL-cholesterol, HDL-cholesterol and triglycerides), adverse events and treatment adherence were collected from medical records and were transferred to an HIV database system. For those switching to the E/C/F/TAF regimen, the following parameters were recorded before the switch, and tests were repeated every 3–6 months.
Patients with high creatinine and low eGFR were also compared. For this comparison, the US National Kidney Foundation Classification for chronic kidney disease was used 24 : high creatinine was defined as >1.1 mg/dL in women and >1.3 mg/dL in men; low eGFR was defined as 90 mL/min/1.73 m2 for both genders. Rates of patients with low HDL and high triglyceride were compared using the National Cholesterol Education Program criteria 25 : low HDL (<55 mg/dL in women and <45 mg/dL in men) and high triglyceride (>200 mg/dL) were compared. Hepatitis B and C co-infections were screened by anti-HCV and HBsAg. The results at baseline and 3, 6 and 12 months were used for the analysis.
Adherence was assessed by the self-reporting of the patients. Reported side effects included those that were patient-reported (symptoms and complaints), based on laboratory data and clinically reported (signs and physical examination findings).
Statistical Analysis
For descriptive statistics, continuous variables were given as mean ± standard deviation, and categorical variables were given as rate and percent. Continuous variables at baseline, month 3, month 6 and month 12 were compared by repeated-samples ANOVA, and categorical variables were compared by Cochran’s Q test. p < 0.05 was accepted as statistically significant.
Ethics
The study was approved by the Ethics Committee of Istanbul University, Cerrahpasa Medical School.
Results
The study included 430 treatment-experienced and 184 treatment-naïve patients.
Treatment-experienced patients
Baseline characteristics and treatment durations of study population.
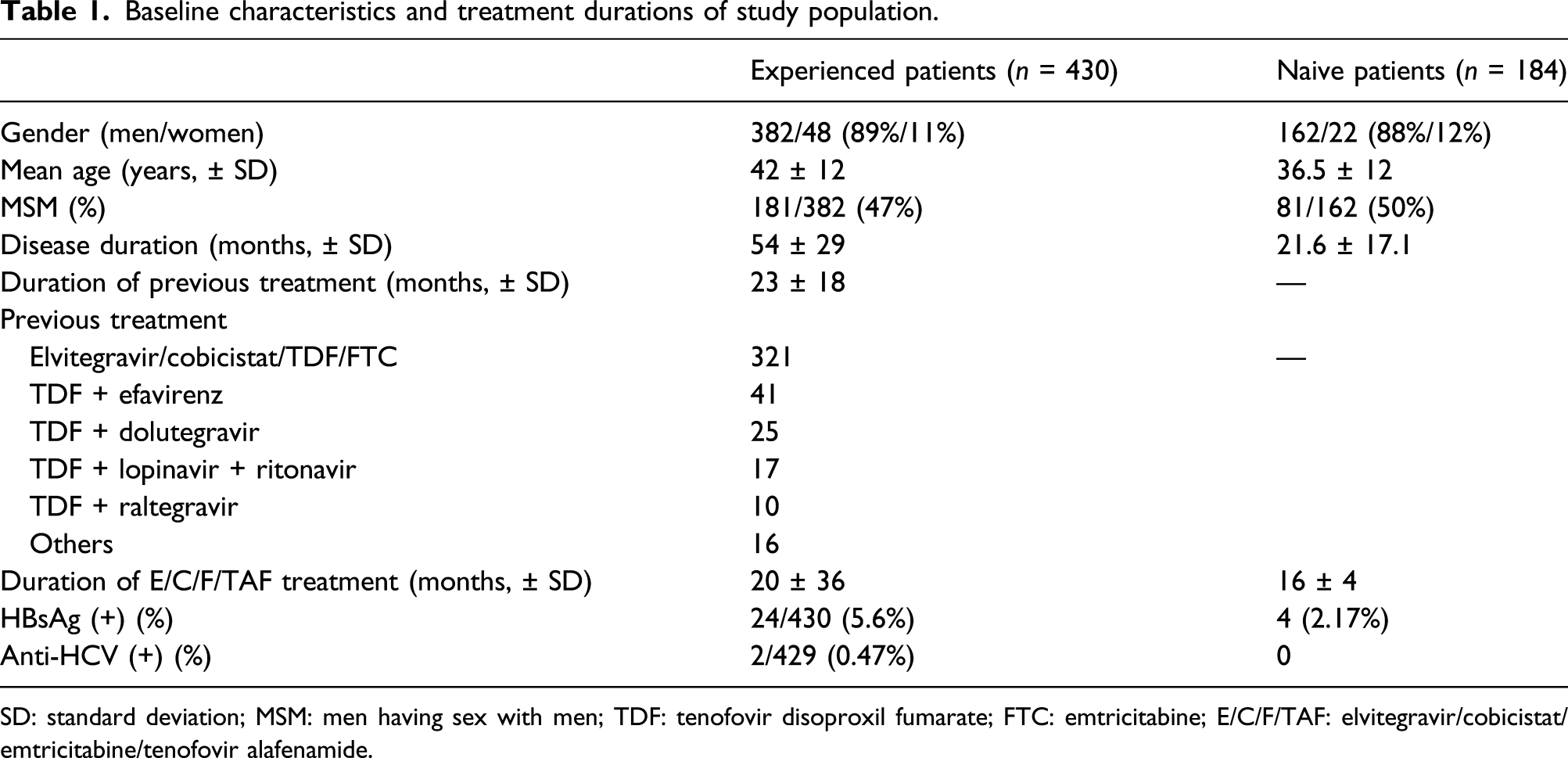
SD: standard deviation; MSM: men having sex with men; TDF: tenofovir disoproxil fumarate; FTC: emtricitabine; E/C/F/TAF: elvitegravir/cobicistat/emtricitabine/tenofovir alafenamide.
Virological and immunological characteristics before and after elvitegravir/cobicistat/emtricitabine/tenofovir alafenamide treatment.
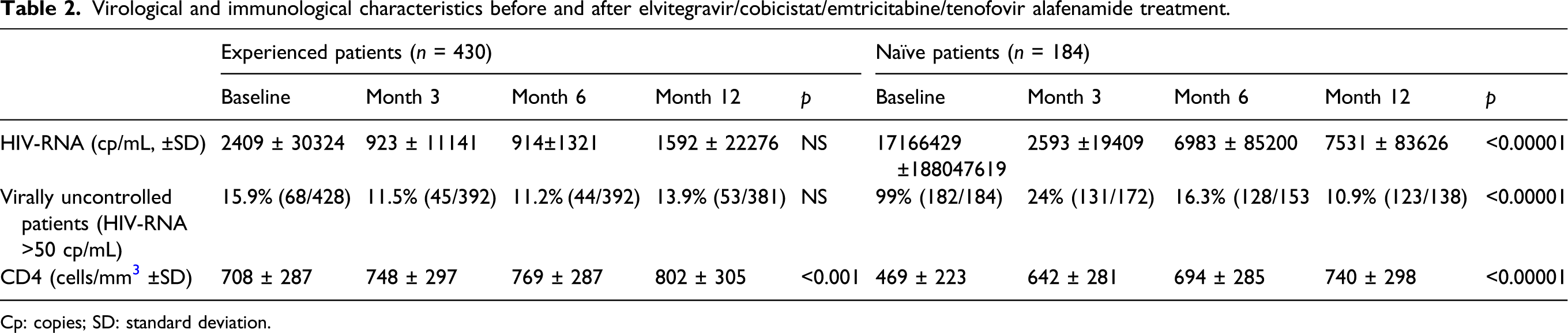
Cp: copies; SD: standard deviation.
E/C/F/TAF treatment was generally well tolerated. Eight patients discontinued the treatment (drug interaction: 3; pregnancy: 1; pulmonary tuberculosis: 1; adverse event: 1; patient’s decision: 1; lost to follow-up: 1).
Renal functions and lipid profile before and after elvitegravir/cobicistat/emtricitabine/tenofovir alafenamide treatment.

SD: standard deviation; NS: not significant; eGFR: estimated glomerular filtration rate; TC: total cholesterol; LDL: low-density lipoprotein; HDL: high-density lipoprotein; TG: triglycerides.
aHigh creatinine= in women >1.1 mg/dL, in men >1.3 mg/dL.
bLow eGFR= <90 mL/min/1.73 m2 according to US National Kidney Foundation Classification..
cLow HDL= in women <55 mg/dL, in men <45 mg/dL.
Treatment-naïve patients
Demographic characteristics and clinical features of treatment-naïve patients treated with E/C/F/TAF are given in Table 1. Following the E/C/F/TAF regimen, HIV-RNA levels decreased, the rate of virologically suppressed patients decreased, and CD4 count increased significantly (Table 2).
E/C/F/TAF treatment was generally well tolerated. Three patients discontinued the therapy (drug interaction: 1; non-responder: 1; patient’s decision: 1).
Creatinine levels and those with stage 2 kidney disease increased within the first 3 months of therapy and then remained stable (Table 3). eGFR and those with high creatinine did not change. Total cholesterol levels, those with high total cholesterol, LDL level, triglyceride level and those with high triglyceride increased. HDL level increased while those with low HDL decreased.
The rate of adherence was 98.1% and 98.4% for 1 year in treatment-experienced and treatment-naive patients, respectively.
Discussion
A total of 614 patients were analysed in this retrospective study of treatment-experienced or treatment-naïve PLWH who were prescribed the co-formulated E/C/F/TAF regimen. The study showed that the INSTI-based co-formulated regimen is effective in providing a viral suppression rate of 86% and 90% after 12 months of therapy in treatment-experienced and treatment-naïve patients, respectively. These results are comparable with other real-life clinical studies yielding 67%–88%26–29 and 75%–96%28–30 in treatment-experienced and treatment-naïve patients, respectively. Clinical studies, real-life data, meta-analyses and systematic reviews support the efficacy of INSTIs-based regimens.31,32
The tolerability was optimal in both treatment-experienced and treatment-naïve patients. Among INSTI-based regimens, there have been unexpectedly high discontinuation rates, mainly due to the neuropsychiatric side effects of dolutegravir. Discontinuation rates were 4%–6%.12–14 Elvitegravir use was not associated with this side effect in our cohort. The high rate of adherence in our cohort is probably multifactorial. The study includes five dedicated HIV centres which have much fewer barriers to HIV care. A multidisciplinary approach to complicated challenges of HIV care increases the patients’ adherence to a given centre. Moreover, taking one co-formulated pill obviously decreases the pill burden and increases adherence, thus sustains viral suppression and improves the quality of life.33–34
Renal function remain a concern in tenofovir-containing regimens. TAF contains much less tenofovir than TDF, and renal adverse events are expected less and milder in severity. Although our study is an observational one, in the treatment-experienced patients’ cohort, the vast majority of the patients were switched from a TDF-containing regimen to a TAF-containing one. This switch resulted in improved renal functions in some cohorts.35,36 During the switch and in the following 12 months, there were no significant changes in renal functions in our study. Baseline eGFR was suggested as a significant predictor of the change in eGFR; patients on TDF with poorer baseline renal function would benefit more from switching to TAF. 37 Baseline renal functions were optimal in our treatment-experienced patients, which may explain why any such positive impact of TDF–TAF switch was not observed.
Lipid parameters showed significant changes in both treatment-experienced and treatment-naïve patients. There were significant increases in the proportions of patients treated with TAF-containing regimens with more severe dyslipidemia in other cohorts.38–40 This change was suggested to be reversible after switching back to TDF. 41 A post hoc study evaluated the impact of lipid changes on predicted atherosclerotic cardiovascular disease (ASCVD) risk and statin eligibility in treatment-naïve 1774 adults living with HIV treated with TAF or TDF. 42 In that study, lipid changes (increases in total cholesterol, LDL and HDL) with TAF as part of co-formulated regimens did not substantively affect CVD risk profiles compared to TDF. However, considering the increasing age and other cardiovascular risk factors of patients living with HIV, changes in lipid parameters should be followed up closely and for the long term.
Our study has some limitations inherent to its retrospective design. Most patients in our study were young men with optimal renal functions and relatively high CD4 counts. Fewer comorbidities and favourable baseline patient characteristics decrease the significance of difference, which is expected from a real-life study. The second limitation is the relatively short duration of the cohort study. Both renal functions and lipid parameters may be further affected in the long term, and in order to reach conclusions from this treatment regimen, a longer time of follow-up is required.
Our observational real-life study showed that starting with or switching to E/C/F/TAF in PLWH effectively suppresses HIV infection, is associated with an increase in CD4 cell count and is well tolerated in a real-life setting. Renal functions remained stable during the treatment. E/C/F/TAF use was associated with increases in LDL-cholesterol, triglyceride and also HDL-cholesterol levels, which may require closer long-term follow-up for their probable clinical significance.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Gilead Sciences İlaç Tic. Ltd.Şti. (Istanbul, Turkey). Gilead Sciences İlaç Ltd.Şti. was not involved to the content of the publication; no involvement to the analysis or interpretation of data/no involvement to the decision to submit for publication.