
Abstract
Introduction: Understanding and following HIV self-testing (HIVST) instructions is a critical step in the use of HIVST kits. We analyzed data on pregnant women and their partners’ self-assessment on the usability of kits delivered by their pregnant women. Methods: Quantitative data were collected on 399 pregnant women and 238 male partners enrolled in the intervention arm of a large cluster-randomized HIVST trial. Each pregnant woman received HIVST demonstrations, detailed pictorial instructions on how to use OraQuick HIVST kits, and two kits; for herself and her male partner. Follow-up was at one month (baseline for male partners) and 3 months. Descriptive statistics were conducted to compare understanding and following of HIVST instructions by age and education level. Results: The proportion of those who understood HIVST instructions was almost the same (98%) for women and their partners, although partners (26.5%) were nearly twice as likely than women (16.0%) to report needing pretest counseling (Odds ratio [OR] = 1.9, 95% CI: 1.27–2.79). Partners’ understanding of the HIVST instructions did not vary by education level, but 4.4% of women with primary education reported difficulty in understanding HIVST instructions compared with 0.5% and 0% of those with secondary and university education, respectively (p = 0.05). However, 5.6% of women aged 30–68 years and 3.3% of partners aged 20–24 years found it more difficult to understand the HIVST instructions. Conclusion: Both pregnant women and their male partners were correctly able to perform an HIVST without or (with minimal) support suggesting that this mode of delivery will help the national program reach more men. Because more male partners than women required HIVST pretest counseling support, male-targeted HIVST promotional messages may be needed to increase men's self-efficacy to perform HIVST unsupported.
Keywords
Introduction
Globally, 79% of adults living with HIV 1 and 76% in East and Central Africa know their HIV status. 2 These figures reflect a marked improvement toward achieving the first goal of the United Nations’ 90–90–90 targets, in which 90% of all people with HIV should know their status by the year 2020. 3 However, East and Central Africa still contain 2.7 million people living with HIV who do not know their status. 2 Therefore, innovative HIV testing strategies like HIV self-testing (HIVST) are still needed to fast track this target. HIVST refers to a process in which a person collects his or her specimen (oral fluid or blood), performs a test, and interprets the result, often in private or with someone they trust. 4
Although HIVST was first proposed as an alternative testing approach of HIV-testing services in the 1980s, it did not reach Africa until 2017. 5 The novel strategy of HIVST was expected to address poor access and uptake of HIV services by men and young adults who are reluctant to utilize the conventional modes of HIV testing.6,7 HIVST has the potential to reach many people who cannot or choose not to access health facilities8–10 for HIV testing services. Secondary distribution of HIVST kits through pregnant women attending antenatal care (ANC) clinics to give to their male partners is a promising strategy to increase testing coverage among men. 11 In Malawi, between 87% and 95.4% of partners of pregnant women randomized to HIVST arms tested for HIV. 12 In Kenya, partners randomized to the HIVST arm with an improved invitation letter were 12 times more likely to test compared to the standard of care arm. 13 Partner testing rates have been increasing from 79.1% 14 to 90.8% 15 and recently to 95%. 16 In Uganda, 77.2% of partners self-tested and the strategy also promoted couple testing and disclosure. 17 Ninety-one percent couple testing was reported in Kenya among partners of female sexual workers. 18 However, it is not clear whether the partners found the testing instructions easy to understand. HIVST may also help reduce the burden on the health facilities and health workers. 19 Knowledge of HIV status is critical as it facilitates timely initiation to HIV treatment, prevents mother-to-child transmission, 20 improves male partner testing, and can guide safer sexual decision-making among sex workers. 21 Previous studies in the United States (US), India, Malawi, and Kenya have reported that HIVST is highly acceptable with rates above 80%7,22–24, except for a 2014 study conducted among men who have sex with men in Los Angeles where acceptability was at 66.3% 25 and in Kenya where only 53.8% of women chose oral HIVST. 26 Reasons for high acceptability include autonomy, self-management, empowerment, privacy protection, and convenience since HIVST is done in the absence of a health worker.27–29 However, factors such as low education levels may limit its use, mainly among the poorly educated facing difficulty in interpreting test results. 30
HIVST studies conducted among different populations in Los Angeles, 25 San Francisco, 22 India, 24 Democratic Republic of the Congo (DRC), 31 and Kenya 23 , whether supported24,31 or unsupported22,23,25, have reported the test to be either easy or very easy to use. However, 18.7% of participants in India 24 , 20.8% in DRC, and 8.9% in Kenya 23 reported needing assistance from a healthcare provider or someone else before they conducted the test. Factors such as age and low education levels among participants have inhibited people’s ability to use the HIVST kits effectively. 31 Results from a multicountry study conducted in three sub-Saharan African countries revealed that less than 25% of low-educated participants performed each step of the self-test correctly even after receiving pictorial and written instructions in both English and local languages. 32 Forty-four percent and 73.6% 31 of participants with lower education levels versus 70% and 90.6% with higher education levels were able to correctly comprehend instructions and interpret test results, respectively. In a study conducted in Malawi, illiterate individuals; those with lower levels of schooling, from rural areas, and unfamiliar with standard pictorial images 34 ; and women requested significantly more assistance when self-testing for HIV. 7 Participants with primary and secondary school education and those aged 18 years and older in Kenya, found it very easy to understand user instructions for the HIVST kit, read test results and take the cheek swab. 13 This study reported results about ease of understanding HIVST instructions in general; hence, it is not clear how easy it was for partners to understand the testing instructions. Although more than 90% of the male partners in Kenya who used the oral HIV self-test kits reported that it was easy to take a sample and read the test results, 14 it is still unclear if age and educational level had an impact on the usability of the kits. Whereas the previous studies above31–33 assessed use of kits by index clients, there is observed variability in the ability to comprehend and correctly use the self-test kits among primary testers.
To address these gaps, we conducted context-specific assessments on usability of self-test kits by pregnant women and their male partners who used self-test kits delivered by their pregnant women to guide client education and support.
The government of Uganda has, in its testing policy, added HIVST as one of the HIV testing strategies to improve uptake of HIV testing, especially among men. At the moment, it is not clear if people will be able to easily understand the HIVST instructions or follow the steps accurately. Our study aimed to determine the usability of HIVST kits by pregnant women attending antenatal care and their male partners to inform the planned scale-up of HIVST in Uganda.
Methods
Study design and population
A total of 1514 pregnant women aged 15–49 years were enrolled; 777 in the intervention and 737 in the control arm. The ANC clinic days were randomized into either control or intervention days. Women who came on control days received treatment as usual including encouragement of partner testing at the health facility or other convenient place, but no HIVST kits were provided. The HIVST kits were distributed on intervention days. 17 This article is based on the 777 pregnant women who were randomized to the intervention arm. A total of 637 participants (399 women and 238 male partners) who performed the HIVST themselves were assessed prospectively at month one and three to determine if they found it difficult to understand as well as follow the HIVST instructions including conducting the HIV self-test. The questions used to collect data for this sub-study were the same at months 1 and 3. However, participants tested at different points within the follow-up period of 3 months, and thus, we present results for months 1 and 3.
Study sites
The study was conducted between July 2016 and February 2017 in the three public health facilities of Mpigi Health Center IV (HCIV), Entebbe Hospital, and Nakaseke Hospital in central Uganda (all supported by Mildmay Uganda). These sites were selected because they had low rates of testing for HIV among the male partners of pregnant women attending ANC. Entebbe is urban; Mpigi is semi-urban, while Nakaseke is rural. Between July 2014 and June 2015, Entebbe Hospital registered 7034, Mpigi HCIV registered 3245, and Nakaseke Hospital registered 1523 pregnant women attending their first ANC visit. At the time of initiating the study, only 6% (466) of male partners in Entebbe, 3.1% (102) in Mpigi, and 31.5% (480) in Nakaseke previously tested for HIV, based on the routine health facility records.
Overview of the HIV self-testing intervention
We randomly allocated clinic days to intervention or control, based on a sequence of random numbers generated in Microsoft Excel. We also generated separate lists of random numbers for each study day to randomly select pregnant women from each clinic to approach for screening and recruitment into the study. Women with a primary partner they saw at least once a week, whose partner was of unknown HIV status, and had not tested for HIV in the previous six months, and women who were not anticipating any form of intimate partner violence were enrolled. Women who were too sick to consent for study participation were excluded from the study. Women randomized to the intervention arm received two OraQuick kits (OraQuick HIV-1/2 antibody test; OraSure Technologies)—one for themselves and the other for their male partner. These women received general and HIVST health education including clues on how to introduce the kit, pictorial instructions, and an individual demonstration on how to use the kits led by a nurse counselor. Women in the intervention arm were instructed on how to accurately interpret the results and watched a video clip in which HIVST instructions were demonstrated. The women were expected to orient their partners in HIVST instructions. The packets containing the HIVST kits were labeled and packed. The telephone number of a counselor was included in the information sheet delivered by the women to the partners and they could contact the counselor as needed, in case of emerging questions or counseling needs.
Data collection methods
Trained interviewers administered the questionnaires to study participants. Study data were collected and managed using both the Research Electronic Data Capture (REDCap) web application hosted at the Medical University of South Carolina 35 and the offline (mobile) application from Vanderbilt University. REDCap is a secure, web-based application designed to support data capture for research studies, providing (1) an intuitive interface for validated data entry, (2) audit trails for tracking data manipulation and export procedures, (3) automated export procedures for seamless data downloads to common statistical packages, and (4) procedures for importing data from external sources. Following challenges with use of the offline REDCap application, data were collected with paper questionnaires and entered using the web-based online REDCap system.
Measures
Our primary outcome variables for this analysis were self-assessed understanding and following HIVST instructions and were measured as a proportion of all participants who used HIVST kits themselves and found no difficulty in conducting each of the HIVST instructions (understanding instructions, swabbing the gum, timing the test, and reading and interpreting the test results). Self-assessed understanding and following HIVST instructions were measured by asking respondents if they found any difficulty in performing the instructions specified for each of the four HIV self-testing steps: (1) understanding the instructions inserted in the packets, (2) swabbing the gum, (3) timing the 20 min for the test, and (4) reading and interpreting the test results. These responses were provided on a three-level Likert scale: 1 = very difficult, 2 = somewhat difficult, and 3 = not difficult. In addition, for the current analysis, we dichotomized the three-level Likert scale by combining responses of 1 and 2 to compare somewhat or very difficult versus not difficult. For each participant, we created four primary outcome measures by integrating responses across the two follow-up timepoints at months 1 and 3 so that the participant was classified as having self-assessed difficulty if they reported somewhat or very difficult for a procedure at any timepoint. Finally, we also asked participants whether they needed additional counseling before or after self-testing for HIV. A response of “yes” to this question was because each male partner confirmed they called the helpline.
Questionnaire data were collected on relevant sociodemographic characteristics. We conducted a separate subgroup analysis to explore the effect of education level and age-group on the respondents’ understanding of HIVST instructions. Respondents’ education level was recoded into three categories: individuals with no formal education and those who went to school but stopped at nursery or primary level were categorized as having “primary education” because the number with no formal education was too small to stand alone as a group. Participants with vocational and secondary school were categorized as having “secondary education”, while those who attended college and university were categorized as having “university education.” Age categories were based on the Uganda Demographic and Health Survey categorization. 36
Data analysis
Pregnant women and male partners’ understanding and following of HIV self-test instructions at baseline and 3-month follow-up.
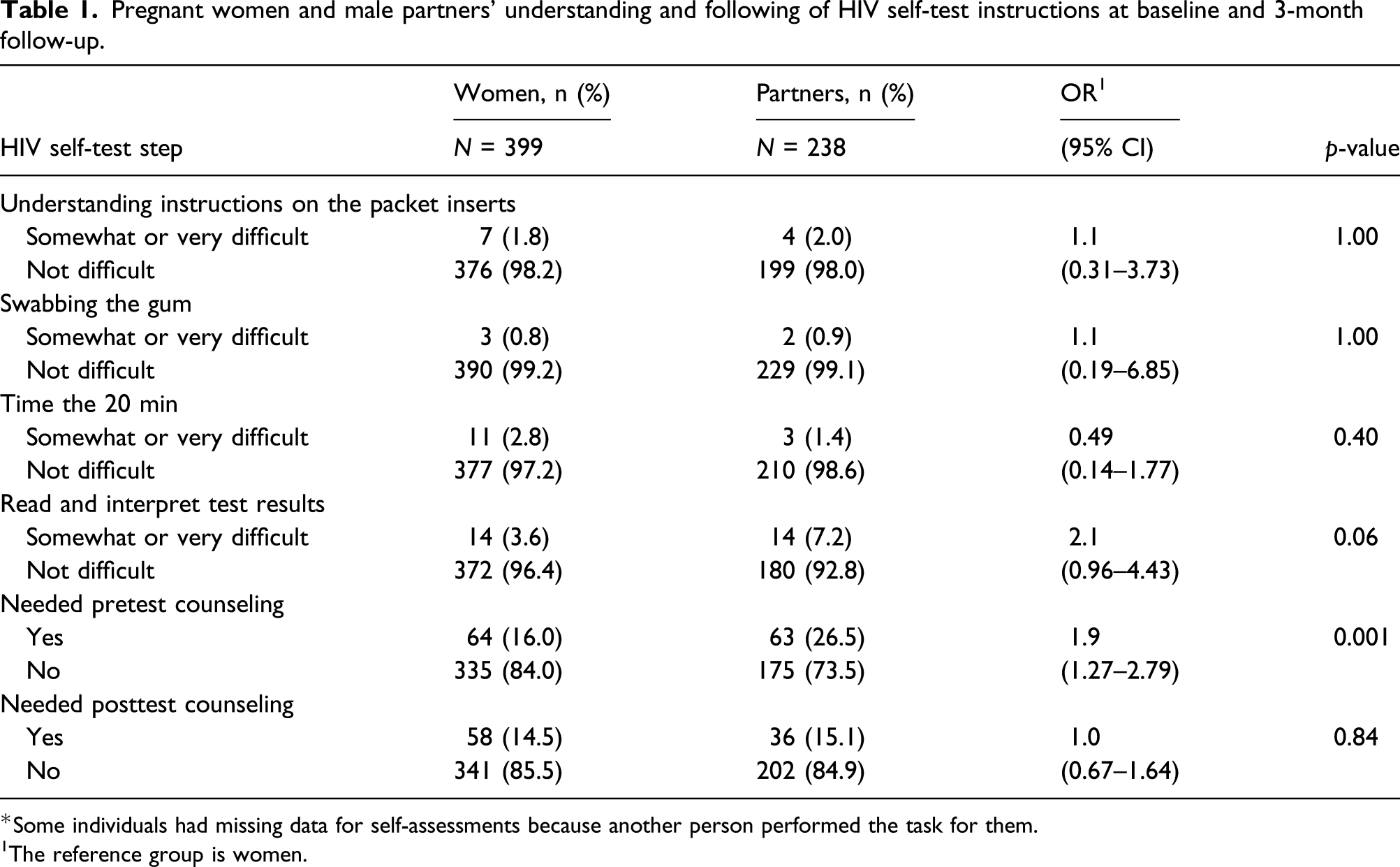
*Some individuals had missing data for self-assessments because another person performed the task for them.
1The reference group is women.
Level of education and understanding and following of HIV self-test instructions at baseline and 3-month follow-up.
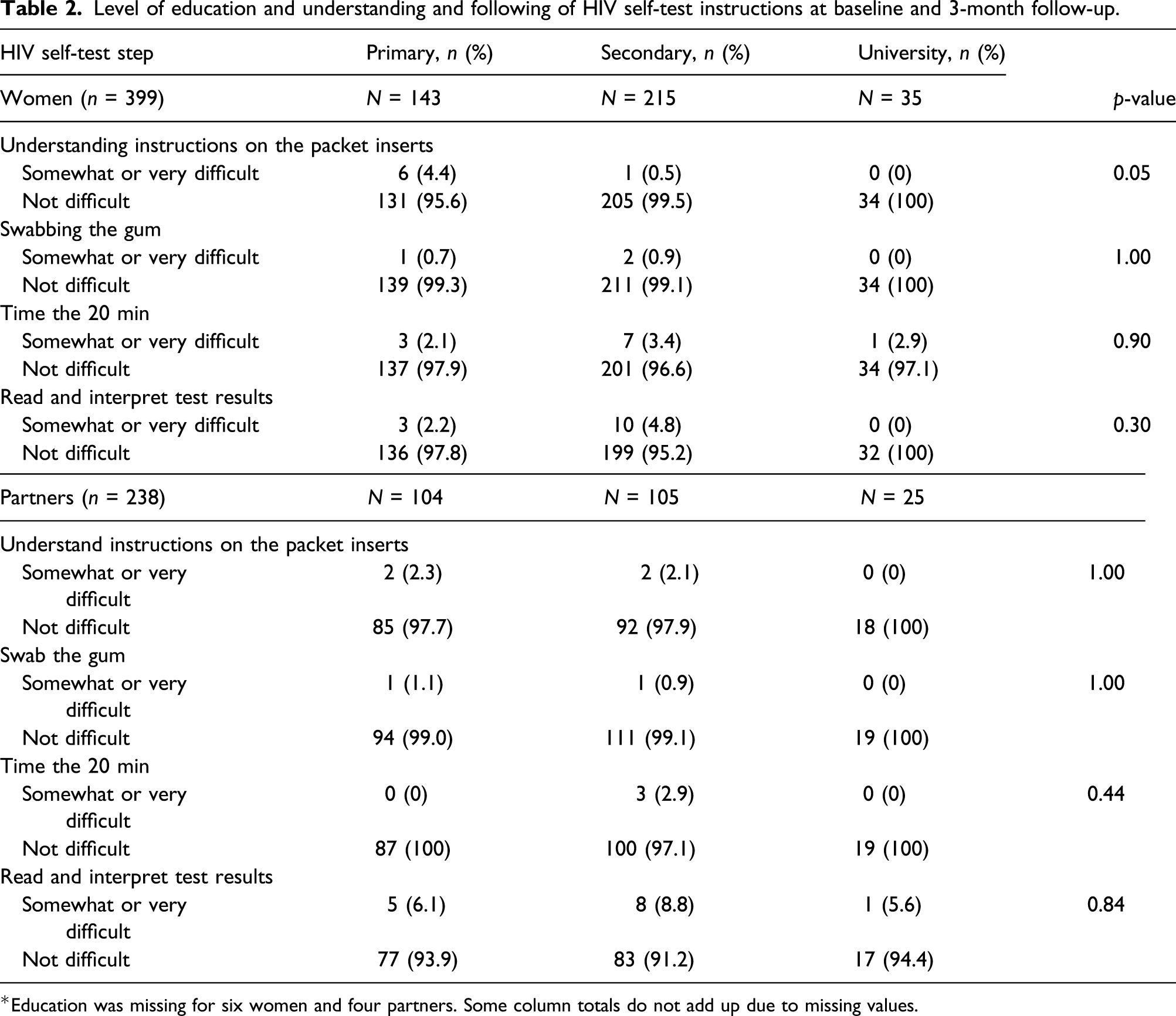
*Education was missing for six women and four partners. Some column totals do not add up due to missing values.
Age and understanding and following of HIV self-test instructions at baseline and 3-month follow-up
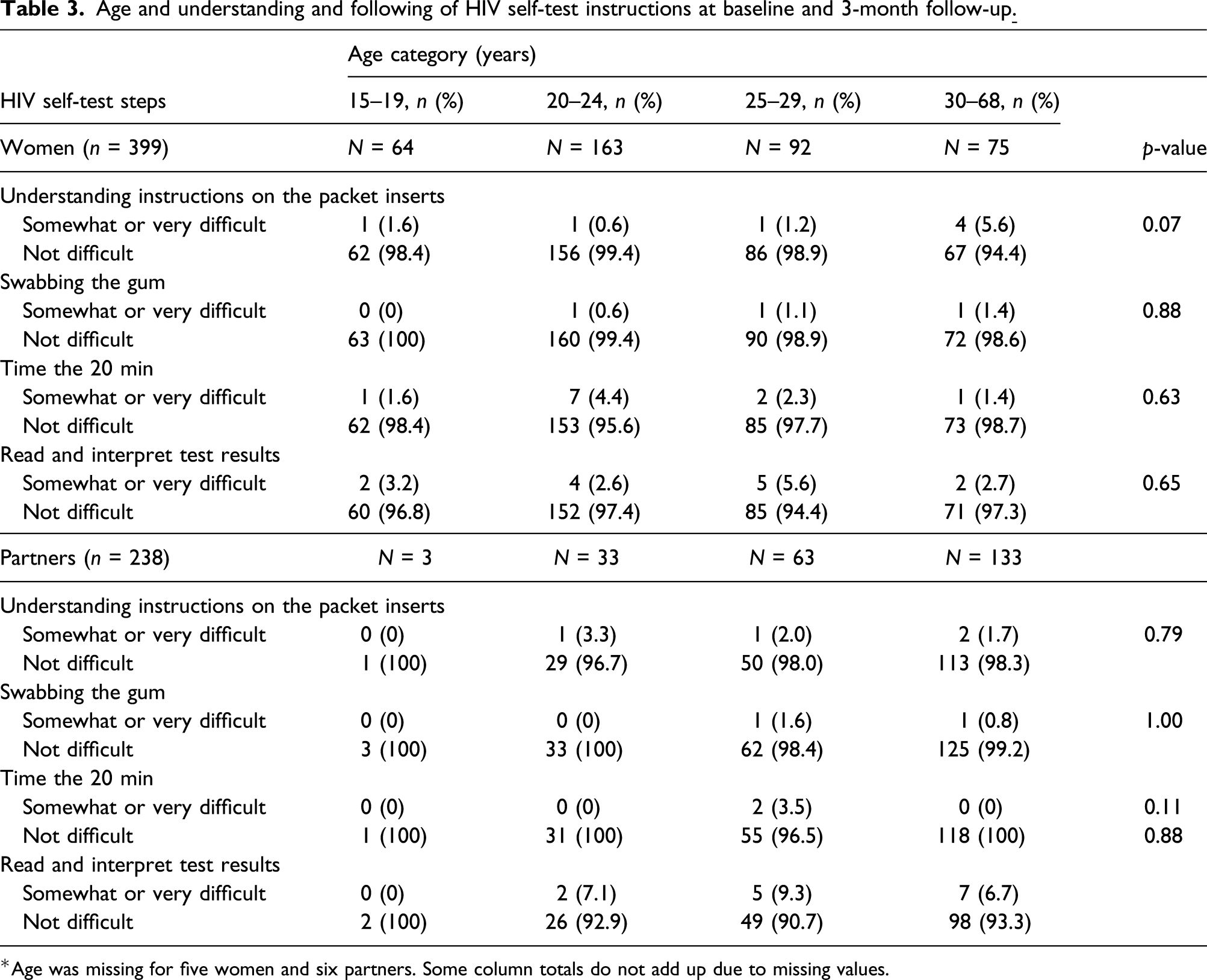
*Age was missing for five women and six partners. Some column totals do not add up due to missing values.
Ethics approval and consent to participate
The study was approved by Makerere University School of Public Health Higher Degrees Research and Ethics Committee, Uganda National Council for Science and Technology, and the Medical University of South Carolina Institutional Review Board. The study was registered with 3ie’s Registry for International Development Impact Evaluations (RIDIE-STUDY-ID-56e1817442fbf).
Results
Respondents’ characteristics
Respondents’ characteristics.

*Some column totals do not add up due to missing values.
Understanding and following HIV self-testing instructions among pregnant women and male partners
Table 1 shows the pregnant women and male partners’ understanding and following of HIVST instructions, stratified by sex. Nearly all women (98.2%, n = 376) and partners (98.0%, n = 199) reported no difficulty in understanding the instructions inserted into the HIV self-testing package. Difficulty reading and interpreting the HIVST results was reported by 14 women (3.6%) and 14 partners (7.2%) each; however, there was not a statistically significant difference (p = 0.06). Partners (26.5%) were twice as likely to report needing pretest counseling as women (16.0%) (OR=1.9, 95% CI: 1.27–2.79; p = 0.0014). The two groups did not differ significantly with regard to self-assessed difficulty swabbing the gum, timing the test, or requiring posttest counseling.
Education level and understanding and following HIV self-testing instructions
Table 2 shows the results of a subgroup analysis to explore the effect of education level on understanding and following HIVST instructions among 399 pregnant women and 238 male partners. Nearly all women, regardless of education level, indicated that they did not find it difficult to understand the instructions on the HIV self-testing package inserts. However, women with primary education were more likely to report difficulty in understanding the instructions compared to those with secondary and higher education although there was not a statistically significant difference by education level (primary: 95.6%; secondary: 99.5%; university: 100%, p = 0.05). These proportions were similar among partners, especially those with primary education (primary: 97.7%; secondary: 97.9%; university education: 100%, p = 1.00), suggesting that more partners than women with primary education had difficulties understanding HIVST user instructions.
The percentage of women who reported no difficulty swabbing the gum (99%–100%) did not differ by education level. A similar observation was made among the partners. Almost 94% of partners with primary education, 91.2% with secondary education, and 94.4% with university education level found it easy to read and interpret the test results. Among women, reading and interpreting the results ranged from 95.2% for those with secondary education to 97.8% and 100% for women with primary and university education levels, respectively.
Age and understanding and following HIV self-testing instructions
Women in the 30–68-year-old age category (94.4%) were less likely to understand HIVST instructions than their younger counterparts in the 15–19, 20–24, and 25–29 age categories (98.4%, 99.4%, and 98.9%, respectively) (see Table 3). On the other hand, the percentage of partners who had no difficulty in understanding the instructions inserted in the packets was higher than that of the women for the youngest age category (15–19 years), although this only represented one man. Difficulty in understanding the instructions was reported among partners aged 20–24 years (3.3%), 25–29 years (2.0%), and 30–36 years (1.7%). A greater proportion of women aged 20–24 years and partners aged 25–29 years reported difficulty timing the test, whereas difficulty in reading and interpreting the test results was reported by 2.6%–5.6% of women across all age categories and 6.7%–9.3% of partners aged ≥ 20 years.
Discussion
Our study assessed the usability of HIVST kits by pregnant women and their male partners. We found that almost no respondents experienced difficulty in understanding the user instructions, and this was largely unaffected by education level or age although slightly more women in the lowest education category had difficulty in understanding the package insert instructions. However, partners were significantly more likely to report needing pretest counseling support than women. This could be because male partners received HIVST instructions from their female pregnant partners who could have missed a step or two in explaining the HIVST process as opposed to women who actually received individual instructions and an HIVST demonstration from members of the study team in addition to watching a demonstration video. Nevertheless, our findings suggest that HIVST instructions can be used with ease by both male partners and women and across education levels and age.
The finding that there was no significant differences in understanding or following HIV self-test instructions by education level may be linked to the various forms of health education women received prior to getting the kits. The multiple instructional materials and demonstrations including materials translated into the local language could have helped the poorly educated women to understand the instructions without difficulty. This could further explain why almost all women with primary education (almost 96%) found reading and interpreting the results not difficult, with a proportion comparable to the middle (99.5%) and highly educated (100%) women. This high frequency of the ease of reading and accurate interpretation of results by the poorly educated was similarly found Kenya, 13 but the assessment did not differentiate between sex. However, the results are inconsistent with a study in three countries in sub-Saharan Africa 32 where only 25% of lay users conducted all HIV self-test steps correctly using test prototypes.
Regardless of age, more male partners than women reported no difficulty conducting the HIV self-test although there was not a significant difference among women and partners by age category. Women aged 30–68 years were less likely to understand user instructions inserted in the HIVST packets than women in other age categories (5.6% vs. 0.6% to 1.6%, respectively). This finding is consistent with a study in Kenya where participants aged 18–34 years and 35 years and older found it very easy to understand user instructions for HIV self-testing kit, read test results, and take the cheek swab. 13 This is possibly because the study did not differentiate between sex. With this striking finding, it is plausible that people including those who receive HIVST through secondary distribution mechanisms can understand instructions with minimal help.
Similar understanding and following of HIV self-test instructions between male partners and women imply that the demonstrations and videos could have minimally impacted on the women’s understanding. A similar finding was observed in Zambia where it was reported that the video demonstration did not further improve understanding of HIV self-test instructions among respondents who participated in hypothetical HIVST. 37 The reasonable difference observed in reading and interpreting results could be due to the partners’ failure to read all the steps in the pictorial instruction sheet due to time constraints or a lack of willingness to completely read the test kit instructions. This is a probable explanation without scientific evidence and urges future research to explore it further. Our findings are consistent with other studies in this area.14,15
Study strengths and limitations
This study is the first to report about the ease of understanding HIVST instructions among secondary self-testers (partners who used kits delivered by their pregnant women) by age and education level.
Despite that, there are some limitations of our study as we did not directly observe participants as they administered the self-testing kits. Our findings are based on participants’ self-reports which may have led to social desirability bias. However, this was minimized by interviewing women and their partners separately since they reported about each other’s experience. Even though we promoted HIV self-testing because the HIV self-test was conducted elsewhere, some self-testers did not perform all of the HIVST user instructions steps unsupported. Hence, those who reported conducting the HIV self-test with support were left out of the analysis.
In addition, while women watched in-person demonstrations conducted by the nurse counselor and the demonstration video, they still found it difficult to swab the gum and time the 20 min for the test. Although it would have been interesting to know why women found these two particular instructions difficult, we did not ask them the reasons for their experience.
Considering the high HIV testing rates reported among male partners, it would have been perhaps more interesting to ask if they had ever heard of HIV self-testing versus HIV in general.
Finally, this study was conducted among pregnant women and their male partners in central Uganda; thus, findings may not be generalizable to other populations.
Conclusion
Both pregnant women and their male partners were correctly able to perform an HIVST without or (“with minimal”) support suggesting that this mode of delivery will help the national program reach more men. Because more male partners than women required HIVST pretest counseling support, male-targeted HIVST promotional messages may be needed to increase men's self-efficacy to perform HIVST unsupported.
Footnotes
Acknowledgements
The authors acknowledge the support from field staff, data entrants, and study participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded through a grant to Makerere University from the International Initiative for Impact Evaluation (3ie) grant agreement no. TW2.2.28.