
Abstract
Introduction
Due to the global COVID-19 pandemic, the Belgian government imposed several physical distancing and mitigation measures in 2020 in an attempt to control the spread of SARS-CoV-2 virus. During the first wave of COVID-19 infections (18 March to 11 May), Belgian citizens were recommended to stay at home (telework was mandatory, only essential travel was allowed, and only food stores remained open) and to avoid any social contact beyond the household. It has been suggested that these social restrictions would translate in reduced incidence of sexually transmitted infections (STIs). 1
Furthermore, nonessential healthcare services were halted. This meant that all booked consultations for the HIV, STI, and PrEP (pre-exposure prophylaxis) clinics were abruptly cancelled, including STI screening in the low-threshold clinics. The only patients that were still allowed were patients with a request for postexposure prophylaxis, patients with STI symptoms, and “vulnerable” HIV patients, whereby the treating physician considered that a face-to-face contact with the patient was necessary.
The first wave of the COVID-19 epidemic ended in May and was followed by relaxing measures. All healthcare clinics could be accessed again. Measures that could influence sexual behavior included an increased number of allowed physical contacts. Commercial sex clubs and saunas remained closed, but sex work was allowed under strict circumstances. From September onward, Belgium, as the whole of Europe, experienced a second wave of COVID-19 cases. This forced the government to reimpose strict measures on November 2. Singles were allowed to have one close contact and one regular extra contact but with physical distancing. Henceforth, close contact with nonsteady sexual partners or anonymous sexual contacts through dating applications, nor commercial sex work were allowed. A major difference between the first and second lockdowns was the accessibility of services, which was limited during the first lockdown, but fully accessible during the second one including the provision of PrEP. In Belgium, PrEP is almost exclusively taken by men who have sex with men (MSM) at high risk for acquiring HIV. Therefore, physical distancing measurements are expected to cause a reduction in the number of STIs found among PrEP users. 2
Several publications investigated the impact of physical restrictions and closure of sexual health services of the first lockdown on the number of STI cases, with varying results. For example, a reduction in the number of STI cases was reported by several countries during the first lockdown period.3–5 In Italy, however, a slight increase in secondary syphilis and gonorrhea was reported. 6 Furthermore, a reduction in casual sex was noted in several countries, including Belgium, during the first lockdown.5,7–9
However, few studies are available which investigate the trend of STIs after a lockdown period, and to our knowledge, none of them explored the effect of the mitigating efforts of the second COVID-19 wave in Europe.
Therefore, our aim was to explore whether the different restriction measures had an impact on the trends of number of tests and diagnoses of Chlamydia trachomatis (CT)/Neisseria gonorrhoeae (NG) before, during, and after the two lockdowns in Belgium in 2020 by comparing them with the same period in 2019. We looked at the trends for all STI patients and PrEP users separately.
Methods
Study setting
Number of CT/NG tests done at ITM in year 2019 and 2020 including demographic information of the patients and the reason of visit.
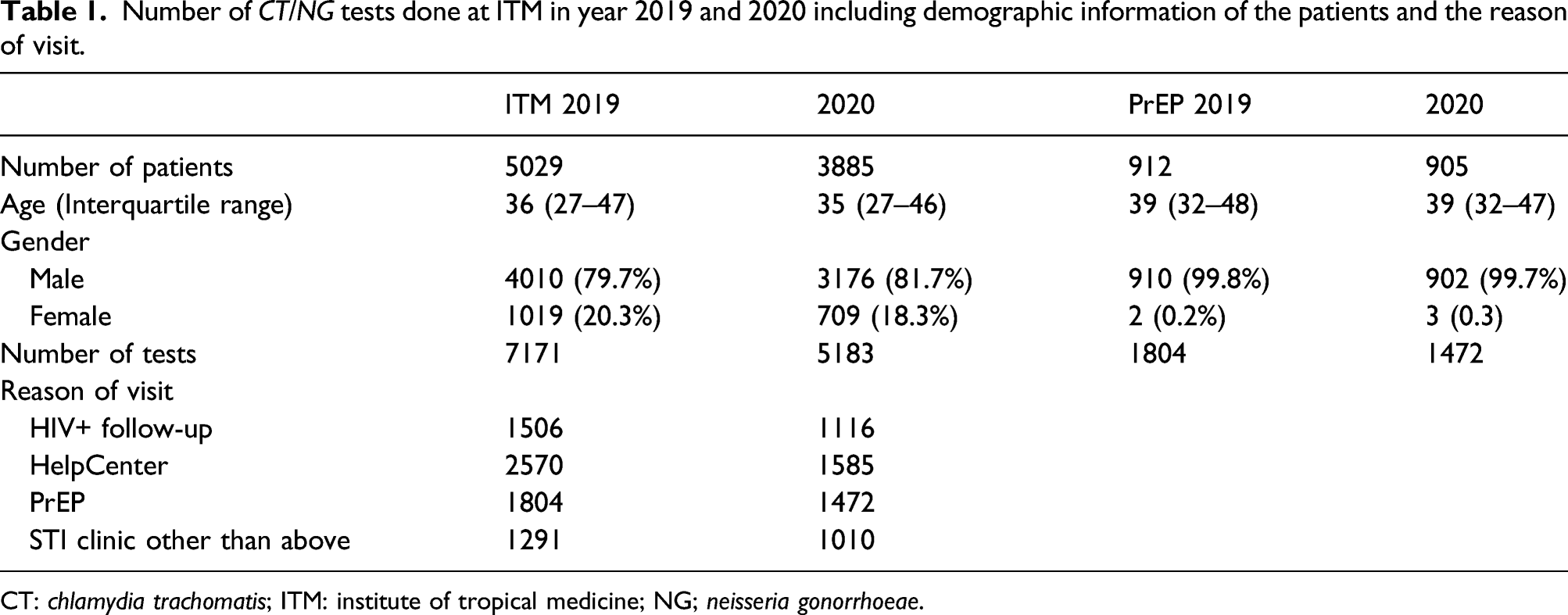
CT: chlamydia trachomatis; ITM: institute of tropical medicine; NG; neisseria gonorrhoeae.
For this analysis, all CT/NG molecular data were collected for the period 2019 until the end of 2020. Data were extracted for two cohorts. The “whole clinic” cohort comprised all tests from individuals attending the STI clinic. The “PrEP-only” cohort was limited to tests from PrEP users.
Testing for CT/NG was performed using molecular amplification assays. Samples were tested with the Abbott RealTime (RT) CT/NG assay (Abbott Molecular Inc. Des Plaines, IL, USA) according to the manufacturer’s instructions. In case a positive NG result was obtained in an extragenital site, confirmation was performed by an in-house real-time PCR assay based on previously published primer sets. 10
Statistical procedures
Duplicate CT/NG results within 30 days were removed from the database to exclude treatment failure. Descriptive analyses of the number of CT/NG tests, number of positive CT or NG cases, and the positivity rate for both STIs were performed for 2019 and 2020 for both cohorts. Specifically, we divided both years into four different periods: 1) pre-lockdown (pre-LD): 01 January to 17 March (11 weeks); 2) lockdown 1 (LD1): 18 March to 10 May (8 weeks); 3) after lockdown 1 (after LD1): 11 May to 01 November (25 weeks); and 4) lockdown 2 (LD2): 02 November to 31 December (8 weeks). All clinical services at ITM restarted after the end of lockdown 1. We estimated weekly testing rates for each period, and we used mixed-effects logistic regression with the individual as random intercept to explore statistical significant changes between CT/NG diagnosis rates in both years and between the corresponding time periods of 2019 and 2020. p-values less than 0.05 were considered to be significant. All statistical tests were performed using Stata 15.1 (StataCorp).
Ethical clearance
According to ITM’s Institutional Review Board, laboratory data of patients can be used for research if the patients’ identity is not disclosed to third parties and the patient does not explicitly state his/her objection. No additional ethical approval or informed consent was necessary.
Results
Table 1 tabulates the number of CT/NG tests including demographic data and the reason why the patient visited the clinic in the years 2019 and 2020.
Whole clinic analysis
Overall STI trends
Weekly number of tests and positivity rate for CT, NG, or both for the whole years and for the different time periods in both years for the ITM cohort. The OR and 95% CIs of period 2020 were calculated using mixed-effects logistic regression.

CIs: confidence intervals; ITM: institute of tropical medicine; LD: lockdown; OR: odds ratio; CT: chlamydia trachomatis; NG: neisseria gonorrhoeae.
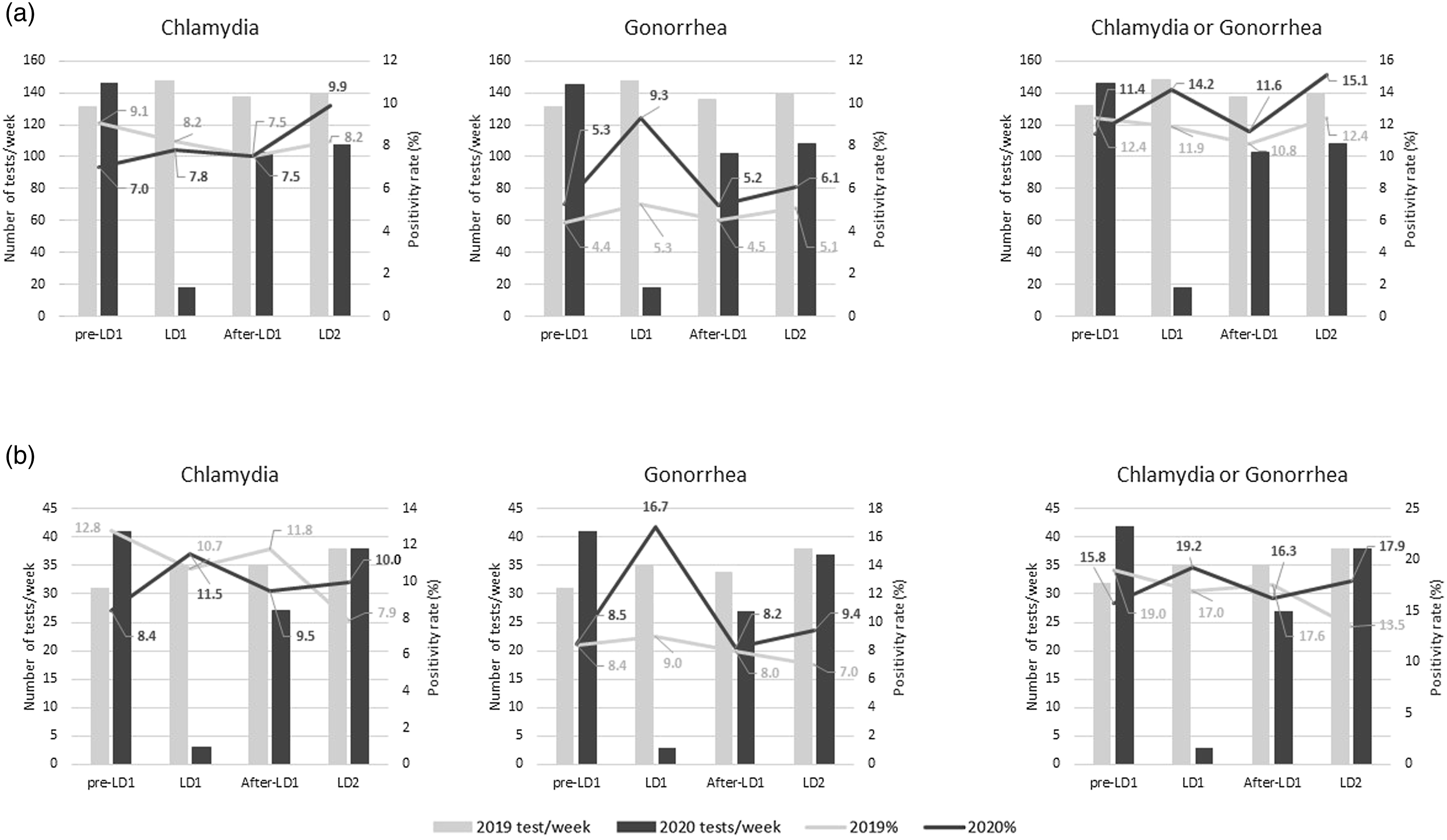
Number of weekly requests (bars) and positivity rate (line) of chlamydia and gonorrhea for the different periods of 2019 and 2020 for the whole clinic cohort (a) and for PrEP users only (b). LD = lockdown. PrEP: pre-exposure prophylaxis
Trends between different time periods of 2020 compared to 2019
Although the positivity rate of CT of pre-LD1 was lower compared to the period in 2019 (p = 0.028), the highest positivity rate was detected during LD2 (9.9%). For NG, a sharp increase in the positivity rate was found during LD1 (9.3%); however, this was not found to be statistically significant (Table 2). During the other periods, no differences were found between 2019 and 2020. Noteworthily, the highest positivity rate for CT and/or NG was found during LD2 in 2020 (15.1%).
PrEP users only analysis
Overall STI trends
Analysis of the trends of STIs of PrEP users only, showed the same trends (Figure 1(b) and Table 3). The overall positivity rate of CT (11.2% in 2019 and 9.3% in 2020) and NG (8.1% and 8.7%, respectively) did not differ (p ≥ 0.05).
Trends between different time periods of 2020 compared to 2019
Weekly number of tests and positivity rate for Chlamydia trachomatis, Neisseria gonorrhoeae or both for the whole years and for the different time periods in both years for the PrEP cohort. The OR and 95% CI of period 2020 was calculated using mixed-effects logistic regression.
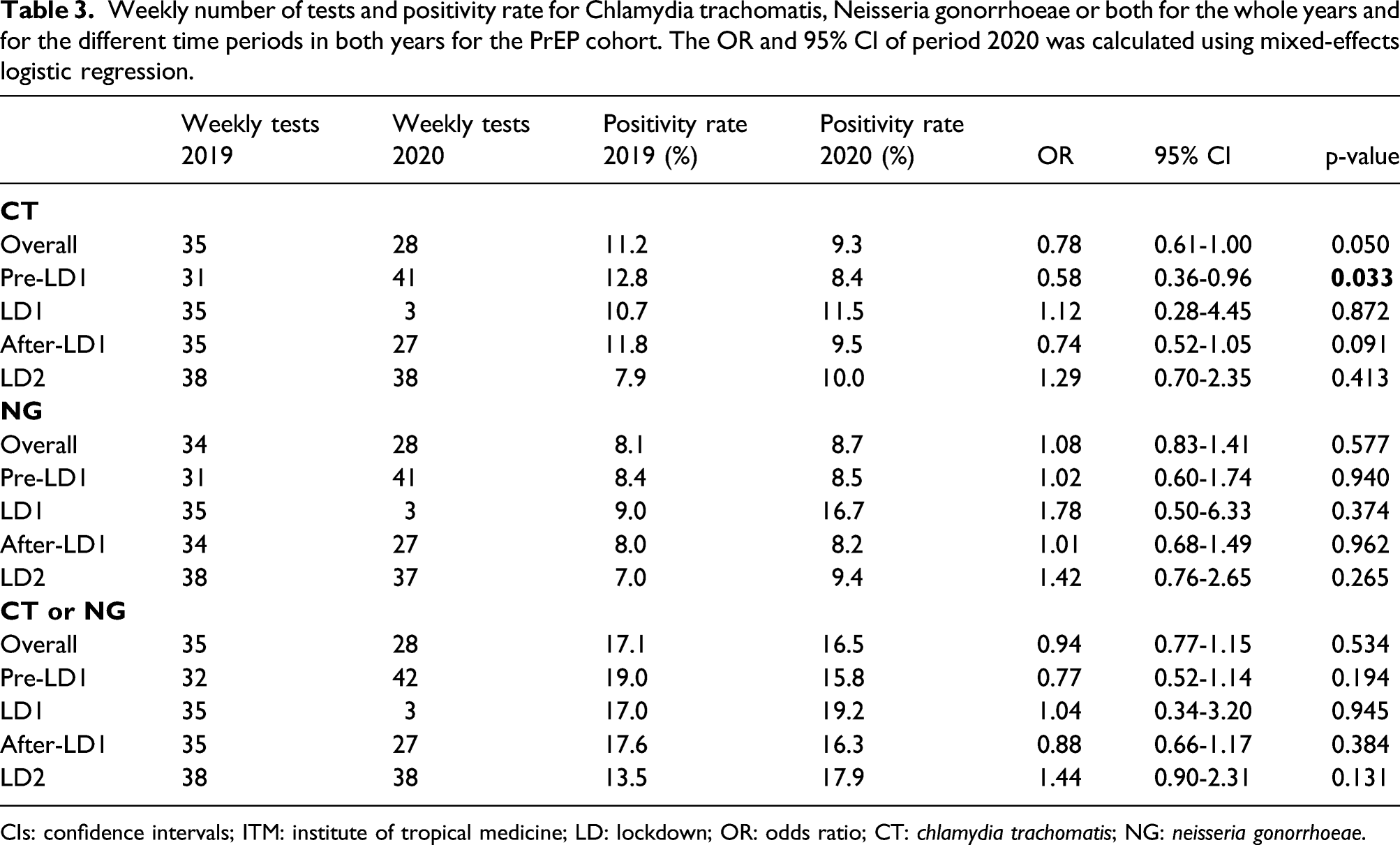
CIs: confidence intervals; ITM: institute of tropical medicine; LD: lockdown; OR: odds ratio; CT: chlamydia trachomatis; NG: neisseria gonorrhoeae.
Discussion
In this Belgian study, we documented an extreme reduction in the number of weekly CT/NG tests and an increase in positivity rate of NG during LD1. This was however anticipated as only urgent STI consultations were permitted during that period. After LD1, all services of the ITM clinic including follow-up of PrEP users and HIV-positive individuals and the low-threshold clinic restarted and remained open. No other significant change in CT/NG trends was found in our STI clinic during the other time periods. During LD2, we reported the highest CT/NG positivity rate at our center for the whole cohort and PrEP users only since 2019. This suggests that the requested physical distancing measures were not stringently followed during LD2. This is in strong contrast with LD1. Indeed, in LD1, an online survey indicated that Belgian MSM reduced their sexual activity with nonsteady partners with 85%. 7 Although no Belgian sexual activity data are available for LD2, personal communication with patients indicate regular sexual activity through internet dating and in private encounters during this period, despite the social measures and the threat of being fined by the authorities.
Our study has several limitations. First, we do not have any information concerning the presence of symptoms which could improve our understanding why individuals visited the clinic in the different time periods. Moreover, due to the fact that our population is mainly male and MSM, the results of our clinic may not be generalizable to the Belgium population.
Our data are in line with other studies investigating the impact of COVID-19 on STI trends. Most of the studies do report a drop in STI infections during the first lockdown followed by a rebound in STI infections.11–13 There are few reports that include results from subsequent lockdowns. Taken in conjunction with other types of evidence such as those detailed above, our results suggest that the decline in the number of diagnoses of CT/NG in LD1 was a result of both reduced testing and changes in behavior. When testing practice returned to normal, the number of positive CT/NG tests and positivity rates rapidly returned to baseline 2019 levels. There was no drop in number of tests or positivity rate during LD2. This finding is compatible with less of a decline in casual sexual contacts than during the first lockdown. There is evidence of physical distancing fatigue in the society as a whole. 14 Although it is possible that part of the differences in CT/NG diagnoses between the two lockdowns could be explained by differences in testing strategy, further behavioral research is needed to compare the compliance with physical distancing measures and sexual activity during the two lockdown periods.
Footnotes
Acknowledgements
We thank the NRC-STI Research groups: Saïd Abdellati, Vicky Cuylaerts, Hilde Smet, Amina Taïbi, Yolien De Caluwe and Sergio Garcia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.