
Abstract
Prevalence of HIV in Slovenia is low, and men who have sex with men (MSM) have the highest risk for infection. Rates of enrolment into HIV care, initiation of antiretroviral therapy and reaching an undetectable viral load in HIV-infected patients are very high. Prevention of HIV infection for MSM with PrEP is not formally available in Slovenia. The aim of this study was to demonstrate possible implementation of PrEP in Slovenia. Sixty-nine (n = 69) MSM with increased risk for HIV received PrEP with oral tenofovir disproxil fumarate /emtricitabine and acquisition were followed for a mean of 566.6 days. They had 71 episodes of STIs (incidence 61.7 per 100 person-years). No one got acquired HIV infection. Estimated glomerular filtration rate (EGFR) was significantly lower 4 (p = 0.014) and 19 (p = 0.021) months after inclusion; however, there was no clinically significant renal failure (mean EGFR 110–115 mL/min). Self-reported body weight significantly increased after 7 months (p < 0.05). Overall EGFR and self-reported body weight did not change significantly. No significant change in adherence (overall mean 81.0%; 95% CI 77.5%–84.6%; p = 0.728), condom use (p = 0.077) and number of sexual partners (overall mean 2.36 per 30 days; 95% CI 2.06 to 2.65; p = 0.235) was found throughout the study. Participants reported 110 graded adverse effects (AE), 104 (94.5%) grade 1–2 and 6 (5.5%) grade 3–4. No participant discontinued PrEP due to AE. The study showed successful implementation of PrEP among MSM at high risk for HIV infection in Slovenia. Based on the results of our study, PrEP should be formally available in Slovenia.
Introduction
Pre-exposure prophylaxis (PrEP) of HIV with oral tenofovir disoproxil fumarate/emtricitabine (TDF/FTC) was introduced in the early 2010s and has shown high efficacy in HIV prevention among men who have sex with men (MSM).1–4 The European Centre for Disease Control (ECDC) and the World Health Organization (WHO) recommended, in 2015 and 2016, respectively, PrEP as part of a combination strategy to end the HIV pandemic.5,6 By the end of 2019, >30 countries worldwide implemented PrEP either through national health services, in specific healthcare settings or via pilot/research/demonstration projects. 7
Slovenia is a country with low HIV prevalence. From 2010 up to 20 November 2020, the yearly HIV incidence ranged from 2.9/100,000 inhabitants in 2016 to 1.3/100,000 inhabitants in 2020. In comparison, the average HIV incidence in the European Union and the European Economic Area was 5.1/100,000 inhabitants in 2018. The predominantly affected group in Slovenia is MSM. 8
The core of HIV prevention among MSM in Slovenia has been safe sex education, good access to HIV and sexually transmitted infection (STI) testing, counselling within the MSM community, early linkage to care and early treatment of people living with HIV. 9 The HIV National Strategy from 2017 to 2025 recommends implementation of post-exposure prophylaxis (PEP) and PrEP. 9 In 2020, 704 HIV patients were involved in care, 92% were on therapy and of those 96% were undetectable; PEP is available through infectious diseases outpatient services. 8 PrEP was not formally available in Slovenia due to insufficient information on PrEP implementation. This demonstration project enabled formal PrEP for MSM at highest risk for HIV infection.
The objectives of the study were to provide information for the national stakeholders on possible implementation of PrEP for MSM in Slovenia, to demonstrate the presence of MSM willing to participate in such a preventive programme and to monitor adherence and safety of PrEP, incidence of STIs, and use of alcohol and drugs at sexual intercourse in this population.
Methods
We conducted a prospective single centre demonstration study assessing possible PrEP delivery in Slovenia. The participants were recruited through social media, nongovernmental organisations, STI outpatient services, HIV anonymous testing sites and oral dissemination in the MSM community. MSM age ≥18 years with ≥1 inclusion criteria in the previous 12 months (self-reported condomless anal sex, a diagnosed STI or any use of PEP) were included. The exclusion criteria were a positive fourth generation HIV test at inclusion (tested <7 days prior to inclusion), estimated glomerular filtration rate (EGFR) <60 mL/min, use of medications influencing renal function, chronic liver disease, HBsAg/anti-HBc positive, current PEP use, and conditions/diseases influencing adherence or safety. The participants used TDF/FTC 245/200 mg in tablet form. The regimen was ‘on demand’: 2 tablets 2–24 h before sex (or 1 tablet if they took ≥1 tablet in the previous 1–6 days), following 1 tablet QD until 48 h after the last sex (2 + 1 + 1). 3 Participants with frequent risk of exposure were counselled to switch to daily regimen. Following the inclusion visit (V0), they were assessed after 1 (V1M), 4 (V4M), 7 (V7M), 10 (V10M), 13 (V13M), 16 (V16M) and 19 (V19M) months. The study drug was dispensed by the researchers at visits until V16M. Safer sex counselling was offered at each visit.
At every visit, self-reported body weight, number of sexual encounters (with differentiation between with/without condom, insertive/receptive and anal/oral), number of sexual partners (without differentiation of the type of sexual partner and steady vs. non-steady) and condom, drug and alcohol use were collected for the period of 12 months before V0 and thereafter for the period in-between two visits. Participants kept monthly diaries on PrEP, sex, drug and alcohol use and adverse effects (AE). Condom, drug and alcohol use were measured by self-reported percentage of episodes of anal sexual intercourse (below 50%, about 50%, about 75% or about 100%) with a condom or with consumption of drugs/alcohol. The participants reported all STIs diagnosed prior to V0 and those diagnosed elsewhere during the study. Laboratory assessment of renal function, liver enzymes, analysis of urine, fourth generation HIV test, HBsAg, anti-HBs, anti-HBc, anti-HCV, VDRL and TPHA/TPPA, and PCR test on separate swabs of urethra, rectum and pharynx for Chlamydia trachomatis and Neisseria gonorrhoeae were performed. Grading of AE was done with the Division of AIDS (DAIDS) Table. 10 See Supplementary Appendix Table 1) for the detailed study protocol.
Renal function was assessed by measurement of serum creatinine and calculation of EGFR in mL/min (Cockcroft–Gault equation adjusted to the ideal body weight). Self-reported adherence to PrEP was defined as the proportion of episodes of sexual intercourse with appropriate timing and dosing of TDF/FTC (2 + 1 + 1) and calculated from the monthly diaries. The incidence of STIs was calculated as the sum of STIs diagnosed elsewhere and STIs confirmed at the study visits (excluding all viral hepatitis) and was adjusted for time in the study (mean duration from first to final visit). All newly diagnosed STIs were treated according to guidelines.
The statistical analysis with Microsoft® Excel® for Microsoft 365 MSO (16.0.13328.20262) was done using descriptive statistics, paired two sample test for means, one-tailed p-value for self-reported body weight and EGFR (comparing values at specific visit to V0) and single factor ANOVA for overall self-reported body weight, EGFR, adherence, number of sexual partners and condom, alcohol and drug use.
The study was approved by the National Medical Ethics Committee (approval number 0120-15/2018/10), and written informed consent was obtained from all participants.
Results
Baseline characteristics of the participants.
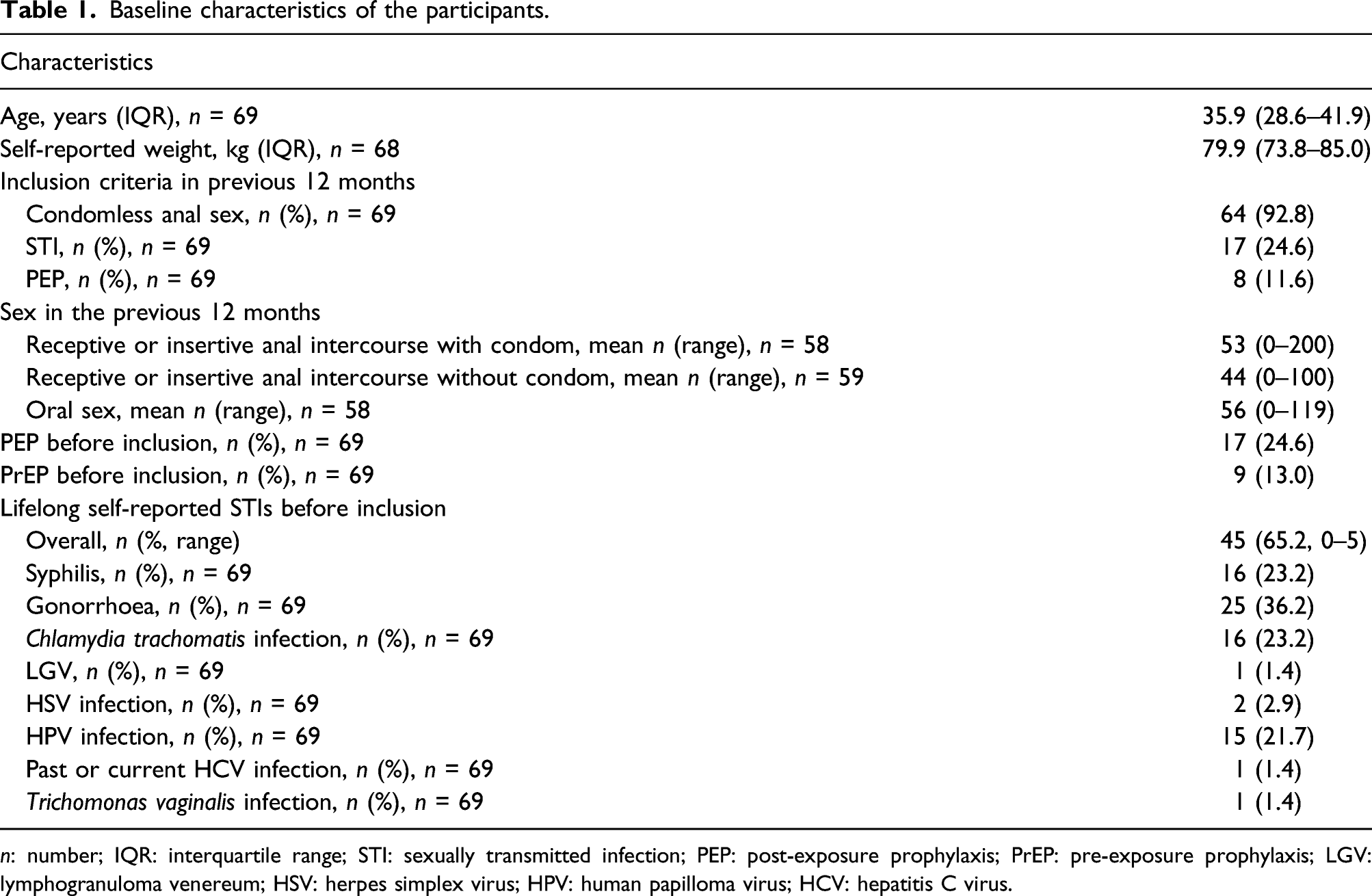
n: number; IQR: interquartile range; STI: sexually transmitted infection; PEP: post-exposure prophylaxis; PrEP: pre-exposure prophylaxis; LGV: lymphogranuloma venereum; HSV: herpes simplex virus; HPV: human papilloma virus; HCV: hepatitis C virus.
During the study, 71 episodes (41 in the study and 30 elsewhere) of STIs in 36 different participants were diagnosed (gonorrhoea 32, C. trachomatis infection 20, syphilis 9, Mycoplasma genitalium 4, HCV 3, HAV 1, HBV 1 and unspecified urethritis 1). HBV infection was diagnosed between V16M and V19M. All three HCV infections were newly acquired, diagnosed by positive anti-HCV in participants previously negative and confirmed by PCR tests. The estimated yearly incidence of STIs (excluding HAV, HBV and HCV) adjusted for the period in the study was 61.7 per 100 person-years. None of the 69 included MSM tested positive for HIV during the study.
Self-reported body weight, serum creatinine, EGFR, proteinuria, adherence, condom use and number of sexual partners.
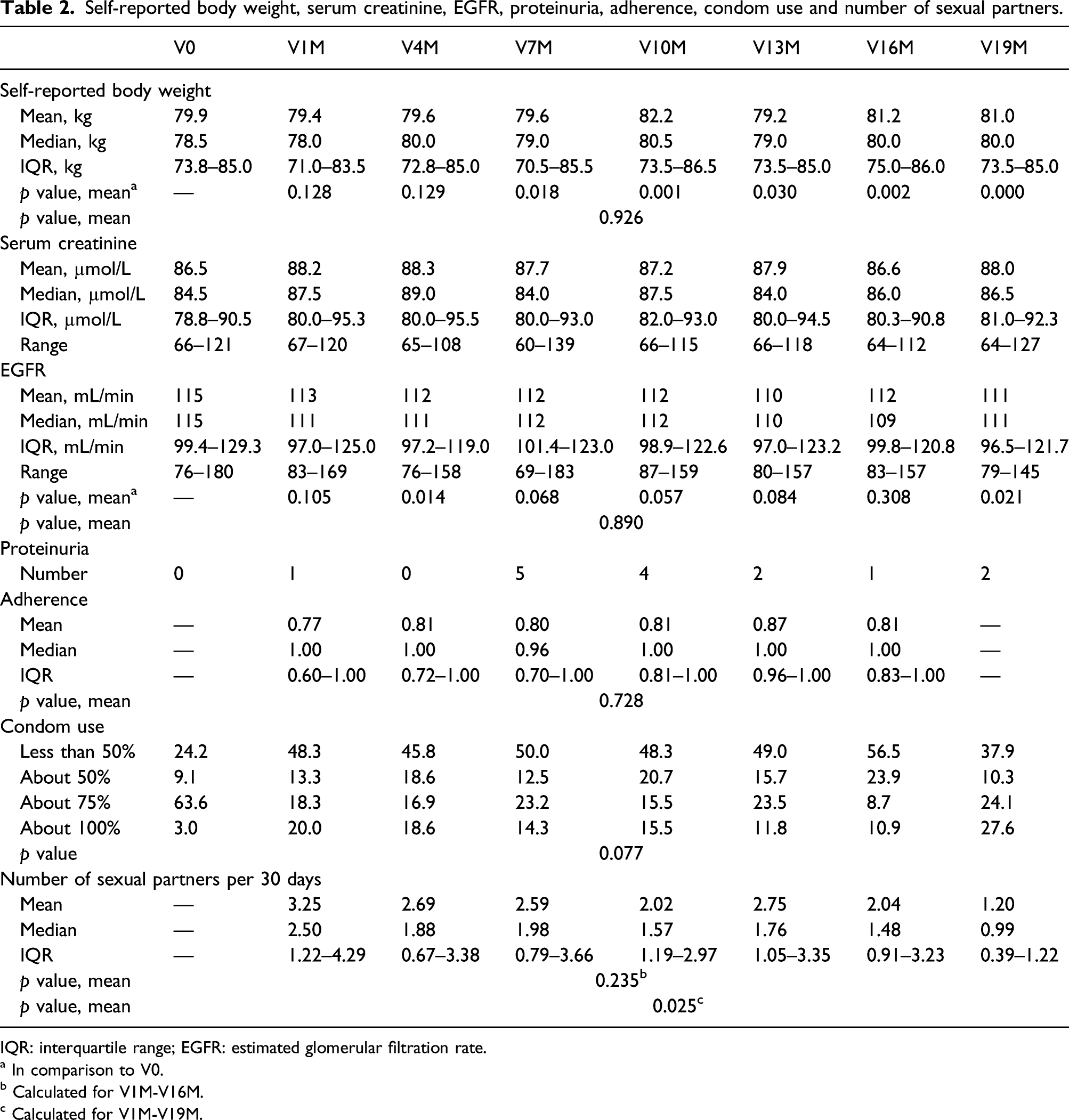
IQR: interquartile range; EGFR: estimated glomerular filtration rate.
a In comparison to V0.
b Calculated for V1M-V16M.
c Calculated for V1M-V19M.
Adverse effects.

AE: adverse effects; AST: aspartate aminotransferase; ALT: alanine aminotransferase; ULN: upper limit normal.
a Excluding participants with same grade elevation at V0.
b 1 participant had hepatitis C virus infection.
c 3 participants had hepatitis C virus infection.
d 1 participant had hepatitis B virus infection.
e Vertigo, headache, myalgia, bone pain, other neurological symptoms, other gastrointestinal symptoms, malaise, chest pain, kidney stones, tachycardia, cold, unspecified.
Discussion
Before this study, formal PrEP for MSM in Slovenia was not available. With the study, we demonstrated the need and feasibility of such a preventive programme in Slovenia, as 69 MSM were successfully included. The participants were at increased risk for HIV infection, as they had frequent condomless anal sex (92.8%), high numbers of sexual partners (2.36 per month) and had extremely high incidence of STIs (61.7 per 100 person-years); incidence in Slovenia in 2018 was 0.07 per 100 person-years. 11 Multiple factors affected this high incidence. As the majority of extragenital gonorrhoea and C. trachomatis infections are asymptomatic, regular screening for STIs in the study would yield higher incidence in comparison to the general population, that is not regularly screened. 12 Also, the inclusion criteria describe sexual behaviour with higher risk for STIs. Although the incidence was high in comparison to the general population, similar incidence rates were demonstrated by others (e.g. AMPrEP).13,14 After conclusion of the study, PrEP was not available to the high risk MSM, which resulted in one HIV infection.
The number of sexual partners was lower than in the PROUD study (≈10 per month) or the IPERGAY study (≈4 per month); however, it might be underestimated as this was not included in the primary protocol and the last visits were often done during the SARS-CoV-2 epidemic.2,3 There was no significant change in the number of sexual partners or condom use throughout the study (excluding data at V19M due to the SARS-CoV-2 epidemic which introduced measures to limit spread of the virus). From March until May 2020, these measures in Slovenia included closure of public transport, schools, nonessential shops, bars, clubs and restaurants, introduction of police curfew, banned gatherings and restriction of movement outside of the municipality of residence; from May until the end of the study, most of the restrictions were lifted. Effect of the introduced measures is shown through the significant decrease in the number of sexual partners at V19M.
During the study, we did not encounter AE requiring exclusion of participants from the study. The majority of the 110 graded AE were grade 1–2 (94.5%), and only 6 (5.5%) were grade 3–4 (one nausea, one diarrhoea and four grade 3–4 liver AE all caused by viral hepatitis). This safety is supported by other studies. 15 Although EGFR was significantly lower at V4M and V19M, this statistical significance did not translate into clinically significant renal failure and no participant had EGFR <60 mL/min. There were also no grade 3–4 serum creatinine elevations. Self-reported body weight significantly increased from V7M onwards and was highest at V10M (+2.9% from V0); similar increase at 96 weeks however was found in a Californian study. 16 Increase in body weight could result from many factors (e.g. ageing, seasonal variability and lockdown) and cannot be directly attributed to TDF/FTC. Safety of PrEP is also supported by the fact that the overall EGFR and self-reported body weight did not significantly change.
Adherence is crucial for efficacy. In the substudy of Partners trial, >80% adherence was associated with 100% efficacy (95% CI 83.7–100). In our study, self-reported adherence to PrEP was estimated at 81.0% overall and did not significantly change throughout the study, although proper dosing was discussed at every visit. Participants with more opportunities for PrEP transitioned from ‘on-demand’ to daily PrEP. Comparison of adherence to other studies is difficult because of different methodology and their subjective component. With this in mind, we demonstrated similar self-reported adherence to others.17,18
Estimation of PrEP efficacy was not the objective of this study, as this was done by others on a higher number of participants1–3; however, we have demonstrated that there is a group of MSM in Slovenia with increased risk for HIV infection, who would benefit from such a programme. In this group, PrEP was safe and properly used. Participation of MSM with increased risk for HIV in such a programme could also provide an important point of access to STI testing, could improve their sexual health and could have measurable public health impact.
Major limitations of our study were small number of participants and self-reported (not measured) body weight and height. More detailed grading of all AE could shed more light on this subject, and in future research, differentiation between symptomatic and asymptomatic gonorrhoea and C. trachomatis infection should be done. There was also the effect of the SARS-CoV-2 epidemic with social distancing, lockdown and decreased availability of our services at V16M and V19M.
Supplemental Material
sj-pdf-1-std-10.1177_09564624211019876 – Supplemental Material for Pre-exposure prophylaxis for HIV with oral tenofovir disoproxil fumarate/emtricitabine in men who have sex with men: Slovenian national demonstration project
Supplemental Material, sj-pdf-1-std-10.1177_09564624211019876 for Pre-exposure prophylaxis for HIV with oral tenofovir disoproxil fumarate/emtricitabine in men who have sex with men: Slovenian national demonstration project by Blaž Pečavar, Barbara Kokošar Ulčar, Manja Kordiš, Maja Pleško, Gabriele Turel, Tomaž Vovko and Janez Tomažič in International Journal of STD & AIDS
Footnotes
Acknowledgements
We would like to thank all participants for their participation in this study. We also acknowledge important contribution of our nursing and administrative staff.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Ministry of Health, Republic of Slovenia and the Slovenian Research Agency (project number V3-1717).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.