
Abstract
This study aimed to document the dermatoses and their relationships with CD4+ T lymphocyte counts and clinical stages of disease among people living with HIV followed by our Clinical Department, to investigate the effect of antiretroviral therapy (ART) on findings and to compare with real-world data. Medical records of people living with HIV were analyzed retrospectively in our outpatient clinic from January 2005 to June 2017. A total of 500 patient files were examined. 179 patients with dermatoses were included in the study. Demographic data, clinical and laboratory findings, dermatological findings, type and distribution of lesions, serological and histopathological examinations, diagnosis, treatment, and follow-up of patients were transferred to data forms. 84.4% of the patients were male and the mean age was 38.65 ± 11.6 years. The median CD4+ T lymphocyte count was 253/mm3 (range:0–1067). At least one dermatosis was present in 69.3% of the patients. Compared with their median CD4+ T lymphocyte counts, the ratio of CD4+ T lymphocytes was significantly lower in the group with three or more dermatoses (p = 0.019). Condyloma acuminatum (15.1%), drug eruption (13.4%), seborrheic dermatitis (11.7%), oral candidiasis (11.2%), dermatophytoses (11.2%), syphilis (8.4%), Kaposi’s sarcoma (8.4%), and telogen effluvium (8.4%) were the most common dermatoses. Kaposi sarcoma (KS), oral candidiasis, onychomycosis, and molluscum contagiosum were significantly higher in the CD4+ T lymphocyte <200/mm³ group when CD4+ T lymphocyte threshold value was determined as 200/mm³. Compared with other TDF/FTC-containing regimens, a significantly higher proportion of alopecia was reported in patients receiving TDF/FTC/EVG/c (p = 0.007). Dermatoses may be a good clinical marker for detecting clinical stage and diagnosing HIV infection; also, there may be a significant increase in the number of dermatoses in advanced stages. Although there are only a few studies in the literature, it should be kept in mind that ART-associated alopecia rates may increase nowadays when ART is targeted at everyone.
Introduction
Acquired immunodeficiency syndrome (AIDS) was first described in the United States of America in 1981 for five previously healthy men having sex with men (MSM) with Pneumocystis carinii pneumonia and 28 patients with Kaposi sarcoma (KS). 1 Today, HIV/AIDS is a chronic manageable condition thanks to antiretroviral therapy (ART). Mucocutaneous diseases are very important in the initial diagnosis of HIV infection and in determining the clinical stage of the disease. Mucocutaneous involvement can be seen in any stage of the disease in 90% or more of HIV-positive patients. 2 The high number of mucocutaneous lesions in people living with HIV is associated with poor prognosis and the development of AIDS in a short period.3,4 Therefore, an adequate dermatological examination may have an important role in determining the severity of HIV/AIDS. 5
Mucocutaneous lesions may differ between countries due to social, economic, cultural, hygienic, and climatic differences. Although the clinical spectrum and prevalence of mucocutaneous lesions have been well studied in Western and Asian populations, there are a paucity of data available from people living with HIV in Turkey.
This study aimed to document the dermatoses and their relationships with CD4+ T lymphocyte counts and clinical stages of the disease among people living with HIV followed up by our clinical department, to investigate the effect of ART on the findings and to compare with world data.
Patients and methods
In this retrospective study, we analyzed the medical records of adults living with HIV who were followed up at our outpatient clinic from January 2005 to June 2017; a total of 500 patient files were examined. One-hundred and seventy-nine (35.8%) patients with dermatoses were included in the study. Data about demographics, clinical and laboratory findings, the most recent CD4 count, viral load, ART, modes of HIV transmission, dermatological findings, type and distribution of lesions, serological and histopathological examinations, diagnosis, and treatment and follow-up of patients were extracted from case records by a single investigator. CD4+ cell count and CD4/CD8 ratio were studied by flow cytometry method (Becton Dickinson, USA) in Orhan N. Ulutin Hemostasis Laboratory of Istanbul University Cerrahpasa Medical Faculty Hospital.
HIV infection was evaluated according to the case definition and staging made by the Centers for Disease Control and Prevention (CDC) in 2008. The stage of laboratory-confirmed HIV infection was considered three regardless of the CD4 absolute count or percentage when an AIDS-defining illness had been diagnosed. 6
The Academic Committee of the Cerrahpasa Faculty of Medicine, Department of Infectious Diseases and Clinical Microbiology, and the Clinical Research Ethics Committee of the Cerrahpasa Faculty of Medicine have approved the study (89125526-302.14.01–30195).
Statistical analysis
Each categorical variable is expressed as the number and percentage of patients. Most continuous variables had non-normal distribution and are therefore presented as medians with interquartile range. Continuous variables with normal distribution are represented as mean ± standard deviation. Differences between groups were assessed by Fisher’s exact test or Chi-squared test for categorical variables. Normally distributed continuous variables were compared with the independent t-test, whereas non-normal ones were compared with Mann–Whitney U test. Continuous variables with more than two groups were analyzed with ANOVA test, and post-hoc analyses were performed by Tukey’s test. All statistical tests were performed with SPSS software, version 21.0 (IBM, Armonk, NY, USA). A two-tailed p < 0.05 was considered statistically significant.
Results
One-hundred and seventy-nine HIV-positive patients with a mean age of 39.1 ± 11.5 years were enrolled during the study period among the 500 files examined. One-hundred and fifty-one (84.4%) patients were male and 28 (15.6%) were female. one-hundred and seventy-one (95.5%) patients were Turkish and eight (4.5%) were foreigners.
Transmission of HIV infection could be identified in 155 (86.6%) patients. The most common mode of transmission was heterosexual contact (43%), followed by homosexual and bisexual contact (42%), intravenous drug use (0.005%), and blood transfusion (0.005%). One-hundred and sixty-eight patients (93.9%) had received antiretroviral drug therapy.
The median CD4 T cell count was 252 cells/mm3 (range, 0–1067 cells/mm3), and 39.1% of patients had CD4 T cell counts below 200 cells/mm3. Most of the included patients were in stage 3 of the CDC classification at initial diagnosis. The median HIV-RNA was 36,000 copies/mL (0–82.863.845). In 115 patients (64.6%), HIV-RNA was <100.000 copies/mL.
The association between the number of dermatosis and CD 4+ lymphocyte count.

a1 vs 3, p = 0.018, One way ANOVA (post hoc test: Tukey).
Distribution of the infectious dermatoses.
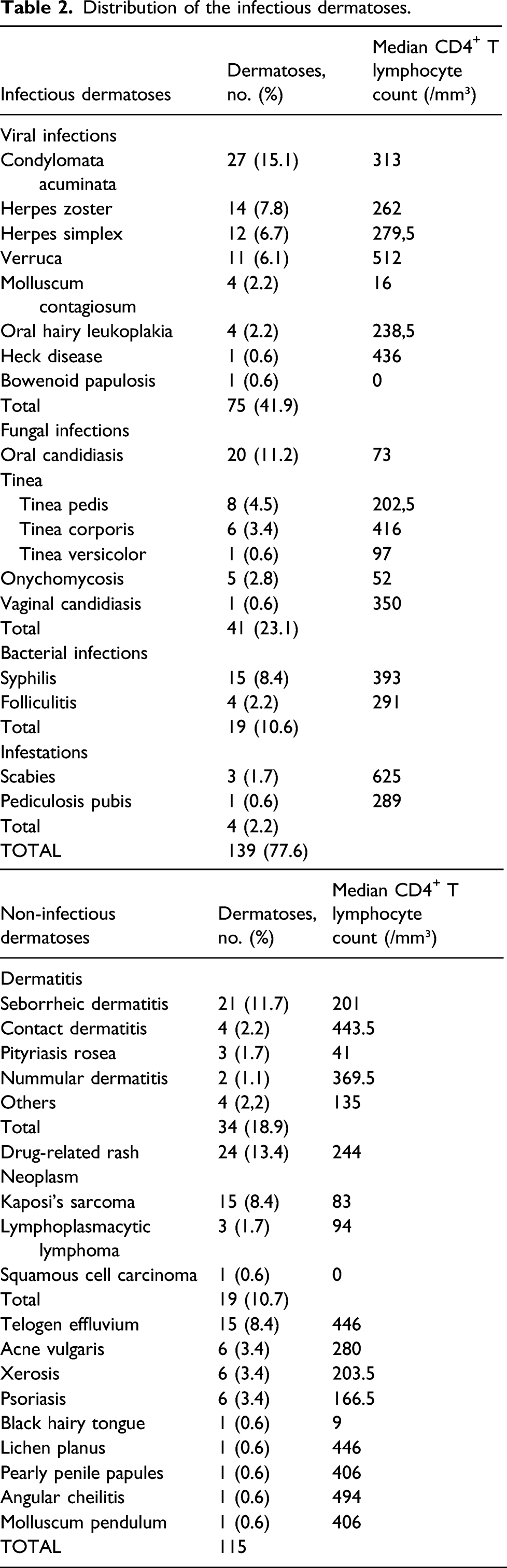
Viral dermatoses (n = 75, 41.9%) were the leading cause of infectious dermatoses, followed by fungal dermatoses (n = 41, 23.1%), bacterial infections (n = 19, 10.6%), and parasitic infestations (n = 4, 2.2%). In the general context, condylomata acuminata (n = 27, 15.1%) was the most frequent dermatological lesion, followed by drug eruption (n = 24, 13.4%), seborrheic dermatitis (n = 21, 11.7%), oral candidiasis (n = 20, 11.2%), dermatophytosis (n = 20, 11.2%), syphilis (n = 15, 8.4%), KS (n = 15, 8.4%), alopecia (n = 15, 8.4%), herpes zoster (n = 14, 7.8%), herpes simplex (n = 12, 6.7%), and verruca vulgaris (n = 11, 6.1%).
Prevalence of dermatoses according to the clinical stage of HIV infection and CD4+ T lymphocyte count.

CDC = Centers for Disease Control and Prevention.
Bold values indicate statistical significance at p<0.05.
aValue has not been computed because Kaposi sarcoma is an AIDS-defining disease, its occurrence concerned exclusively patients in CDC Stage 3.
Prevalence of dermatoses and their relationship to CD4+ T lymphocyte count (>400, 200–400, 50–200, and <50).

Bold values indicate statistical significance at p<0.05.
Four-hundred and eighty-two (96.4%) of the people living with HIV followed by our outpatient clinic were under ART. Of these patients, 219 were using combinations containing Tenofovir disoproxil fumarate/emtricitabine (TDF/FTC) and 77 were specifically using Tenofovir disoproxil fumarate/emtricitabine/elvitegravir/cobicistat (TDF/FTC/EVG/c) (Stribild®). Antiretroviral therapy-related alopecia was seen in seven of the patients receiving other regimens containing TDF/FTC and six of those using TDF/FTC/EVG/c. Patients with age-related androgenetic alopecia and alopecia due to other medical causes were not included in this category. Hair loss symptoms subsided 2–3 months following the cessation of the culprit drugs in the ART-related alopecia patients. The incidence of alopecia was significantly increased in patients receiving ART (Stribild®) (p = 0.007).
Discussion
In the course of HIV infection, different skin lesions may be the first sign of the disease. These lesions can occur at any stage of the disease and reflect the progress of HIV infection and affect the quality of life significantly. 7 Skin manifestations can be seen in 86%–96% of individuals living with HIV.8–10 Skin lesions and their combinations may be so unique that they should raise the suspicion of HIV/AIDS. Skin lesions often tend to occur in advanced stages of HIV infection and may be indicative of poor survival, likewise CD4 + T lymphocyte count.9,10
A total of 500 patient files were examined. Dermatological involvement was present in 179 patients (35.8%). This rate is lower than other studies. It may be due to missing file data and the retrospective nature of our study. Dermatological lesions may be rare since patients are diagnosed and treated earlier in the last years. Many centers have reported the incidence and clinical characteristics of dermatological lesions in people living with HIV; however, first, the trials from Western countries are relatively old and were carried out before the ART era, and thus, these findings may have been different if they could have been treated with modern HIV therapy. Second, relatively recent reports are mostly from the Far East countries like India, Thailand, or African countries, and the prevalence rate shows variability among countries. Data on dermatological lesions in people living with HIV from Turkey are very limited. 5
Two hundred and fifty-four dermatoses were detected in 179 patients. 30.7% of the patients had more than two lesions. Mignard et al., and Tzung et al.,2,10 reported an inverse relationship between the frequency of dermatoses and CD4+ T lymphocyte count. Our findings were also consistent with these reports. CD4+ T lymphocyte count was significantly lower in patients with more than two dermatoses.
In our study, we have sub-grouped the lesions into two groups: infectious and non-infectious. Infectious lesions constituted 54.7% of the dermatoses. Forty-two percent of infectious dermatoses and 48% of non-infectious dermatoses were seen when the CD4+ T lymphocyte count was below 200/mm³. No significant difference was found between the two groups when infectious and non-infectious dermatoses were compared according to CD4 + T lymphocyte levels (p = 0.44).
One-hundred and thirty-six (77.6%) of the patients had infectious dermatoses; 41.9% were viral, 23.1% were fungal, and 10.6% were bacterial. Among the infectious dermatoses, 27 (15.1%) of the patients had condyloma acuminata, 20 (11.2%) had oral candidiasis and 15 (8.4%) had syphilis infection.
Condylomata acuminata was the most common dermatoses among the infectious lesions and drug-related rash was the most prevalent in non-infectious lesions. The prevalence of condylomata acuminata was reportedly 3.1%–12.8% in previous studies.10,11 In our trial condylomata acuminata was the most frequent dermatological lesion (15% of all dermatological lesions). This may be due to the male-dominant nature of our study population; 89% of our patients were men, and sex between men was one of the most frequent ways of disease transmission in our patients. Most of the condylomata acuminata cases were in the MSM group (66%), and 88% of these patients had less than 200/mm³ CD 4+ T lymphocytes. Lesions were mostly in the anogenital area (Figure 1). Diagnosis of three patients was made histopathologically. The rest of the patients were diagnosed clinically. Palefsky et al. reported higher incidence rates of anal human papillomavirus infection in people living with HIV, especially in the MSM group, similar to our study.
12
Genital condyloma acuminatum.
In our study, herpes zoster was seen with a rate of 7.8%. Most of the lesions (61%) showed multidermatomal involvement. Shobhana et al. showed the incidence of multidermatomal herpes zoster as 6%, similar to our study. 13 The lesions were morphologically bullous, hemorrhagic, and necrotic. Five of the nine patients with CD4+ T lymphocyte counts below 350/mm3 had CD4+ T lymphocyte counts below 200/mm3. Herpes zoster was frequently seen in our patients with Stages 2 and 3. In total, 11 (78%) of 14 patients were in Stage 2 and Stage 3. In the study of Tzung et al. as in our study, most of the cases (89%) with herpes zoster were in the advanced stage. 10 The results of our study also support the findings that the incidence and involvement of herpes zoster elevate as immunosuppression expands.10,13
The incidence of HSV infection was reported as 5.5–22% from Southeast Asia.10,14 In our study, HSV infection was seen at a rate of 6.7% similar to these studies. Herpes genitalis was noticed in seven patients, herpes labialis in three patients, and herpes-related oral aphthae in two patients. In many studies, it has been shown that the CD4+ T lymphocyte count is below 200/mm³ in the vast majority of cases (54–66%) with herpes genitalis.12,15,16 Similar to these studies, in our trial, the CD4+ T lymphocyte count was below 200/mm³ in four (57%) of the seven patients with herpes genitalis. Five of the eight patients with a total CD4+ T lymphocyte count below 350/mm3 had a CD4+ T lymphocyte count below 200/mm3. Nine of the patients (75%) were in Stage 2 and Stage 3.
In our study, viral warts were observed in 11 patients (6.1%). Genital warts were in six patients. In the other five patients, the warts were on the face, hands, and feet. Nine of the patients (81.8%) had CD4+ T lymphocyte counts above 300/mm³. Mawenzi et al. reported that the CD4+ T lymphocyte count of the patients was above 300/mm³, similar to our study. 15
In our study, molluscum contagiosum (Figure 2) was seen in four (2.2%) patients. Jing et al. reported the incidence of molluscum contagiosum as 2.1%, similar to our study.
11
The median CD4+ T lymphocyte count of the cases was 16/mm³. Multiple skin-colored umbilical lesions were usually on the face, eyelids, and genitals. The CD4+ T lymphocyte count below 200/mm³ in all patients with molluscum contagiosum was statistically significant when the dermatoses and CD4+ T lymphocyte counts were compared (p = 0.022). Joseph et al. reported that molluscum contagiosum might be a good clinical marker in advanced HIV infection, similar to our study.
17
Molluscum contagiosum.
In our study, oral hairy leukoplakia was seen in four patients (2.2%). Kumarasamy et al. reported oral hairy leukoplakia with a frequency of 2.3%, similar to our study. 16 The median CD4+ T lymphocyte count was 238.5/mm³. Half of the patients were in stage 2, and the other half were in Stage 3.
Following viral dermatoses, fungal dermatoses were the second most prominent dermatoses in our study population. In agreement with previous trials, oral candidiasis was the most frequent fungal dermatoses.5,17 A statistically significant correlation with low CD4 + T lymphocyte counts was found for oral candidiasis.
Bacterial infections were relatively less frequent in our population, and there was no association with CD 4+ T lymphocyte count. The majority of patients with bacterial infections (79%) had CD4 + T lymphocyte counts above 200/mm³. The underlying disease was syphilis in most bacterial dermatoses. This finding was different from most of the previous trials which reported only a few syphilis cases in their respective patient populations.2,10,11 Only Tzung et al. reported a 12.5% prevalence of syphilis in the people living with HIV. 10 In our study, all patients with syphilis were sexually active young male patients with ART, without comorbid disease and opportunistic infection. Skin findings compatible with secondary syphilis were detected in all cases. Of the 15 patients, 13 (86%) had a CD4 + T lymphocyte count above 200/mm³. Eleven patients (73.3%) were in Stage 2. CD4 + T lymphocyte counts above 200/mm³ can be explained by the fact that all of the patients were in the young adult group receiving ART and without comorbid disease/opportunistic infection but with active sexual activity. Since in this group of patients mostly viral load is undetectable they may have had unprotected sexual activity.
Among the non-infectious dermatoses, 24 (13.4%) patients had the drug-related rash, 21 (11.7%) had seborrheic dermatitis, 15 (8.4%) had telogen effluvium, 15 (8.4%) had KS was seen. All patients with telogen effluvium were receiving ART and telogen effluvium was associated with ART.
In the non-infectious dermatoses group, drug-related rash was the leading cause. Adverse cutaneous drug reactions in people living with HIV, especially during the AIDS period, are ten times more common compared to the general population. 18 The skin of people living with HIV is a target organ for drug reactions. Although most skin reactions are mild and do not require discontinuation of treatment, sometimes severe skin reactions can be seen in patients. 8 In our study, drug-related rash among non-infectious dermatoses was seen in 24 (13.4%) patients. Morbilliform eruptions were quite common (n = 21, 87.5%). The rashes were usually on the trunk and extremities. The most common drugs causing rash were efavirenz (EFV) and trimethoprim-sulfamethoxazole (TMP-SMX). Diffuse macular and maculopapular rashes were seen in 11 (6.5%) patients after EFV and regressed with antihistamines. Erythematous macular eruptions developed in seven (4.1%) patients after TMP-SMX. In most of our patients, the rash subsided after the responsible drug was discontinued or changed. Two patients who had severe reactions after TMP-SMX required corticosteroid administration. Diffuse urticarial pruritic plaques were observed in a patient receiving a TDF/FTC-containing regimen. The median CD4+ T lymphocyte count of patients with drug-related rash was 244/mm³. Eighteen patients (75%) had CD4+ T lymphocyte counts below 350/mm³. In a study by Tzung et al., the drug-related rash was found to be more common in patients with AIDS, when AIDS and non-AIDS patient groups were compared. 10 Unlike Tzung et al., the incidence of drug-related rash was similar in both groups in our study. In addition, when patients with drug-related rash were compared in terms of CD4+ T lymphocyte levels (400 and above; 200–400, 50–200, and <50), a statistically significant correlation was found (p < 0.05) (Table 4).
Although the exact mechanism of seborrheic dermatitis among HIV patients remains unknown, the compromised immune system may play a key role. In different studies, the rates of atypical, widespread seborrheic dermatitis have been reported from 15.6% to 83%. Seborrheic dermatitis is considered an early clinical marker for HIV infection 10,18 In our study, seborrheic dermatitis was usually seen on the scalp and the face (Figure 3). Seborrheic dermatitis was observed in all stages, five patients were in Stage 2 and 10 patients were in Stage 3. Approximately half of the patients had CD4+ T lymphocyte counts below 200/mm3, and the median CD4+ T lymphocyte count was 201/mm3. Fascial seborrheic dermatitis.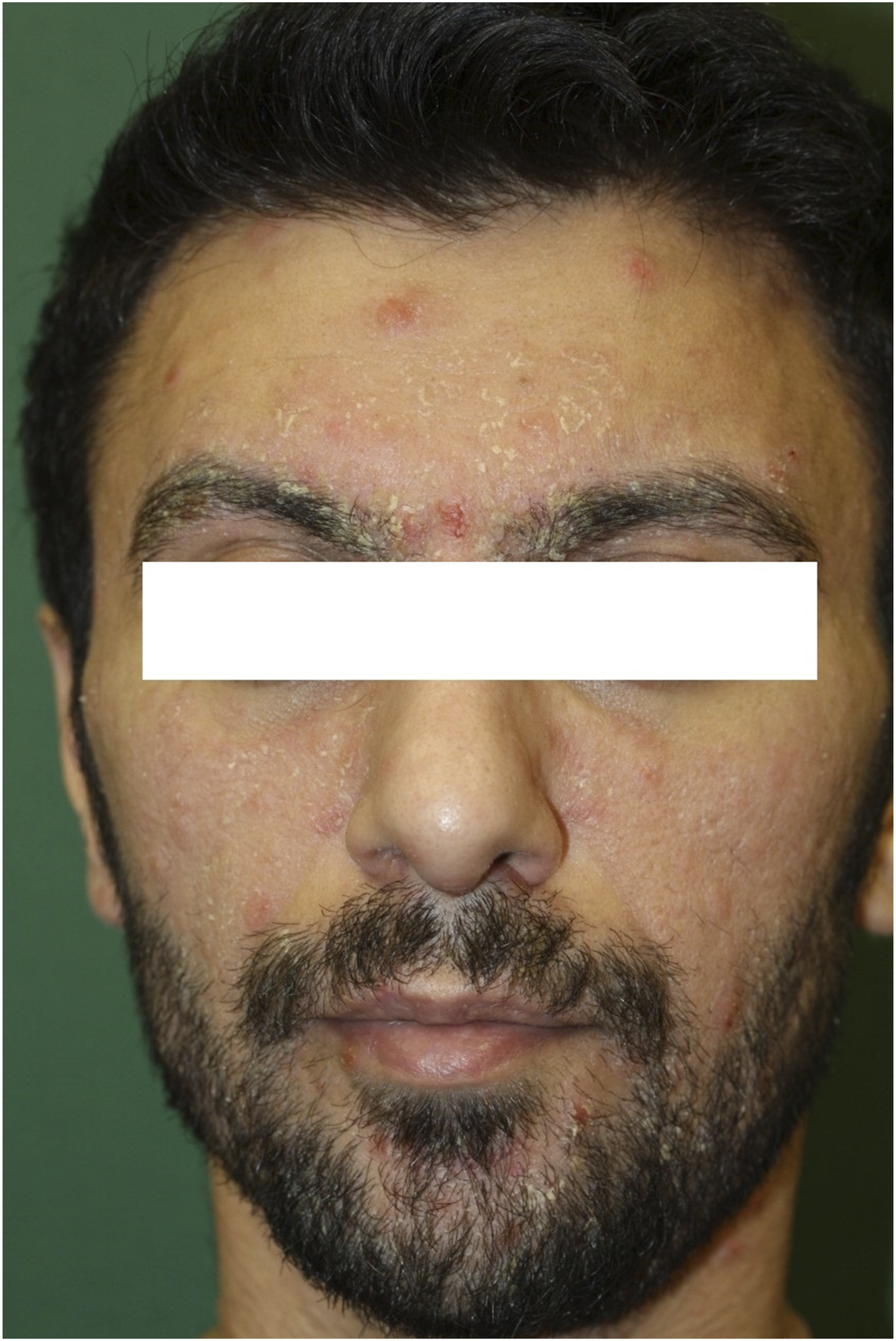
Xerosis, one of the non-infectious conditions, has been noted in six patients (3.4%) in our study. The prevalence of xerosis in our patients was considerably lower than in the other studies. Studies from Taiwan showed similar rates; nevertheless, studies from Malaysia reported higher incidence rates of xerosis, up to 27%.5,10,11,19 All of the patients in our study were in Stage 2 and Stage 3. The median CD4+ T lymphocyte count was 203.5/mm³. Half of the patients had CD4+ T lymphocyte counts below 200/mm³.
The incidence of psoriasis in people living with HIV is very high (25%), especially in Asian countries. 9 However, this rate is around 2–4% in the Western literature. 13 The incidence of psoriasis was found at 3.4% in our study, similar to the Western literature. CD4+ T lymphocyte count was below 200/mm³ in half of the patients.
In our study, KS was observed in 8.4% of our patients, and all of them were in CDC Stage 3. Inconsistent with our results, the prevalence of KS was less than one percent in some previous reports.11,13,17 Different from classical KS, AIDS-related KS predominantly appears on the face, oral mucosa, and upper extremities.
10
KS cases in our trial were in agreement with this information as most of them were seen in the upper extremity and oral mucosa. The intraoral site most commonly affected is the palate (Figure 4). The diagnosis was histopathologically confirmed in all patients with KS. The CD4+ T lymphocyte count was below 200/mm³ in 80% of the patients. These data also support that KS is frequently encountered in advanced HIV infection. AIDS-related Kaposi sarcoma.
Hair loss can also be seen in people living with HIV, which makes our patients very uneasy. Especially in the population living with HIV, sexually transmitted diseases (e.g., syphilis), metabolic and comorbid conditions may accelerate hair loss. The antiretroviral drugs used may also cause severe hair loss. The ART–alopecia relationship has not been investigated well in the literature. There are a total of 16 articles about ART-related alopecia in the literature. Considering that we are now starting ART in all people living with HIV, it can be thought that the frequency of ART-related alopecia will gradually increase.
Hair loss was regarded as telogen effluvium in our trial. Patients with age-related androgenetic alopecia and alopecia due to other medical causes were not included in this category. The vast majority of patients (85%) in our study were young men. The mean age was 32. Hair loss on the scalp and eyebrows was more prominent in our patients, and the findings were often seen in the second month after ART. Hair loss symptoms subsided 2–3 months following the cessation of the culprit drugs in the ART-related alopecia patients.
In our trial, 8.4% of patients had alopecia, and all of them were taking ART; moreover, CD 4+ T lymphocyte counts of these patients were >200/mm³. Therefore, this finding shows that alopecia in these patients is not associated with the severity of AIDS but with the presence of ART. The median CD4+ T lymphocyte count was 446/mm³. Although telogen effluvium was found to be statistically significantly higher in patients with CD4+ T lymphocyte count above 200/mm³, it was thought that this might be because all the patients started ART regardless of CD4+ T lymphocyte count in recent years. Hair loss on the scalp and eyebrows was more prominent in our patients, and the findings were often seen in the second month after ART. Hair loss significantly decreased after discontinuation of the causative drug. Tenofovir disoproxil fumarate/emtricitabine was the backbone of ART in all patients. Tenofovir disoproxil fumarate/emtricitabine caused alopecia in seven patients, TDF/FTC/EVG/c in six patients, TDF/FTC/EFV in one patient, and raltegravir in one patient. When all patients using ART regimen containing TDF/FTC with follow-up from our outpatient clinic were examined, it was found that the incidence of alopecia was significantly increased in patients receiving ART using TDF/FTC/EVG/c (p = 0.007). Compared to TDF/FTC, this high rate was thought to be due to the synergistic or additive effect of EVG/c.
Our study was limited by its retrospective nature and by it being a single-center study with relatively few patients. Prospective studies with a larger sample size will be required to demonstrate the recent prevalence and distribution of dermatological lesions among people living with HIV.
Conclusion
In conclusion, our data show that the prevalence of dermatoses increases as CD4+ T lymphocyte count decreases and the stage of HIV increases. Among the dermatoses, condylomata acuminata was the leading cause, whereas drug eruptions, seborrheic dermatitis, oral candidiasis, dermatophytosis, KS, syphilis, and telogen effluvium were also frequently observed. Although previous studies did not report an important association, we noticed that there was a significant relationship between ART and alopecia, and this finding was more prominent particularly with TDF/FTC/EVG/c.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.