
Abstract
There are currently no reliable epidemiological data for estimating the burden of sexually transmitted infections (STIs) in Oman. STIs such as gonorrhoea and chlamydia are often asymptomatic and associated with sexual and reproductive morbidity. An exploratory study was conducted in an antenatal clinic in Muscat, Oman, to assess the acceptability and feasibility of testing for gonorrhoea and chlamydia. Two hundred and twenty-one women were recruited over 14 weeks between July and October 2020. There were three cases of chlamydia (3/221, 1.36%); no cases of gonorrhoea were identified. Acceptability and feasibility for testing in this cohort of pregnant women were good despite anticipated cultural sensitivities surrounding sexually transmitted infections.
Keywords
Introduction
Chlamydia trachomatis and Neisseria gonorrhoeae are two of the commonest sexually transmitted infections (STIs) in the world. If left untreated, these infections have been associated with adverse maternal and birth outcomes, as well as increasing the risk of HIV acquisition and mother-to-child transmission.1,2,3
In Oman, as in other countries, diagnosis of STIs is primarily through a syndromic approach that utilises an algorithm to classify symptoms and clinical signs into STI syndromes, and patients are treated with standardised drug regimens without reliance on microbiological tests. 4 As a result, little is known about the prevalence of Chlamydia trachomatis or Neisseria gonorrhoeae in the Omani general population. As these infections are often silent, the syndromic approach lacks sensitivity, potentially missing asymptomatic infections and lacks specificity, which can lead to patients unnecessarily exposed to antibiotics.
Notwithstanding sociocultural sensitivities surrounding STIs and religious norms discouraging sex outside marriage, 5 the World Health Organisation (WHO) has estimated that for women aged 15–49 years living in the east Mediterranean Region, the prevalence of chlamydia is 3.8% and 0.7% for gonorrhoea with trends indicating an increase in prevalence of both infections since 2012, 6 while a recent comprehensive review of genital Chlamydia trachomatis infection in the Middle East and North Africa (MENA) has estimated the prevalence in the general population of 3.0% (95% Confidence Interval (CI) 2.3–3.8). 7 Among Gulf Cooperation Council countries, of which Oman is a member state, there has only been one previous study from Saudi vArabia reporting the prevalence of chlamydia of 11.1% (16/144) (as tested by nucleic acid amplification) in a cohort of pregnant women. 8
The aims of this study are threefold: to develop and assess a methodological framework for testing STIs in pregnant women in Oman; to evaluate the acceptability and feasibility of STI testing and treatment among this cohort and finally to provide preliminary estimates of the prevalence of chlamydia and gonorrhoea in this setting.
Methods
Study design and population
We conducted a prospective cohort study over 14 weeks, between July and October 2020 and recruited pregnant women from Al Wattayah antenatal clinic, Muscat, using a modified WHO protocol. 9 Women were eligible if they were 18 years or older, were mentally competent to understand informed consent and were willing to return to the clinic for follow-up care.
The Al Wattayah antenatal clinic is situated in the Muttrah wilayat (district), in the north-east of Muscat city. It also serves as a referral centre for complex pregnancies, and approximately 5500 pregnant women attend the service each year. 10
Women were screened for eligibility by interview with trained medical staff and review of their obstetric records. If eligible, they were given additional printed information in Arabic or English about Chlamydia trachomatis and Neisseria gonorrhoeae infections in pregnancy. The information covered the nature of these infections, the possible consequences to pregnant women and infants and the recommended treatments. Women were verbally informed, either in English or Arabic, about the testing procedure using their first-catch urine samples and the need for retest to evaluate cure after 2 weeks (gonorrhoea) or 6 weeks (chlamydia) if the results were positive. Women were told that if they test positive, they were to inform their spouses to attend for treatment. Women who tested positive for gonorrhoea had additional endocervical swabs for gonococcal culture and antimicrobial sensitivity testing.
Women were contacted about their results by text message, usually within 48 hours. If they tested positive, treatment was provided free of charge and in line with US Centres for Disease Control 2015 guidelines. 11
Measurements
After obtaining verbal and signed written consent, patients were asked to complete a confidential questionnaire, either in Arabic or English, to include information on their age, marital status, education level, current gestational age, birth history and HIV and syphilis serostatus. We also collected information about prior STI diagnoses and current symptoms (dysuria, vaginal discharge, genital ulceration, lumps and bumps and dyspareunia) that could be associated with an STI. Women who declined enrolment had information recorded about their age, parity and reasons, if any, for declining. To further assess acceptability, women were also asked about their opinions on STI testing in pregnancy.
From convenience sampling, between 2 and 7 women were recruited each day during the study period, and their urine samples were retrieved and tested for the presence of Neisseria gonorrhoeae and Chlamydia trachomatis nucleic acid with the GeneXpert nucleic acid amplification system (Xpert® CT/NG assay, Cepheid®, Sunnyvale, CA, USA) in the nearby Microbiology Department at Khoula Hospital. Recruitment capacity was limited by the availability of trained medical staff and restrictions imposed during the study period to prioritise testing for SARS-CoV-2 on suspected coronavirus disease 2019 (COVID-19) samples sharing the same Xpert® platform.
Statistical analysis and estimates
All laboratory, demographic and questionnaire data were entered and tabulated on Microsoft Excel®. We used descriptive statistics to characterise the study population. We used the regional population prevalence of chlamydia (3%, 95% CI 2.3–3.8%) from a recent detailed meta-analysis 7 to derive a minimum sample size of 125 to estimate the prevalence of infection in our cohort with a desired precision of 0.03 and 95% confidence level. 12 The positive predictive values (PPVs) for the Xpert® CT/NG assay are 93.8% for a hypothetical chlamydia prevalence of 3% and 97.3% for a gonorrhoea prevalence of 1%. Negative predictive values for excluding either infections are >99%.13,14
Individuals with missing data were excluded only from the affected analysis. We used Student’s t-test to assess mean age differences among pregnant women who were either recruited to or declined the study.
The study received ethical approval from the Oman Research and Ethical Review and Approval Committee of the Directorate General of Planning and Studies, Ministry of Health (MoH/CSR/19/10943).
Results
Acceptability
Over the course of 14 weeks between July and October 2020, we invited 233 pregnant women and recruited 221 (95%) to the study. Reasons for non-acceptance in 12 women included lack of transport (1), not wanting additional testing (1), fear of a positive result (2) and needing to seek permission from their husbands (2); the remaining six did not give a reason. There was no significant difference in the mean ages between the two groups of women (two-tailed t-test p = 0.91, N.S. at p < 0.05). With practice and greater confidence shown by the recruiting team, there was a noticeable reduction in women who declined participation as the study progressed – 8/89 (9%) declined in weeks 1–5 and 0/63 (0%) declined in weeks 10–14.
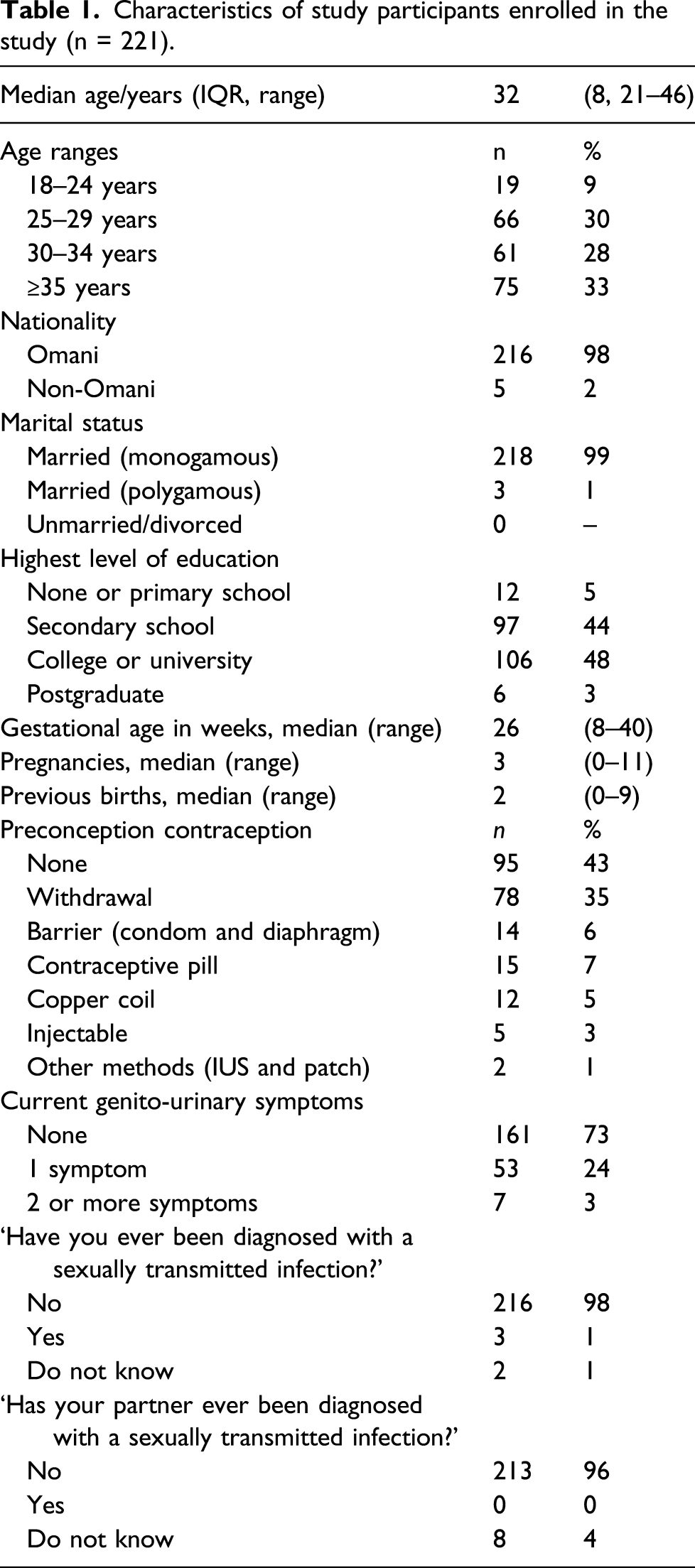
Characteristics of study participants enrolled in the study (n = 221).
Characteristics of pregnant women diagnosed with chlamydia.

Abbreviation: STI: sexually transmitted infection.
Feasibility
Among all the women who were eligible and consented to participate, 100% were successfully tested for Chlamydia trachomatis and Neisseria gonorrhoeae and given their results by text messaging, the majority within 48 hours. Two were recalled to re-submit urine specimens as their initial samples were volumetrically inadequate. No equivocal results were reported for either infection.
All three women who tested positive for chlamydia were treated; one patient received treatment when she was admitted in labour.
Questionnaire responses to provision of STI testing in pregnancy.

Abbreviation: STI: sexually transmitted infection.
Discussion
This is the first study conducted in Oman to assess the acceptability and feasibility for pregnant women to undergo rapid screening for gonorrhoea and chlamydia in a busy antenatal clinic based in its capital, Muscat. Using the GeneXpert system, the estimated prevalence of chlamydia in the population of pregnant women from which our study was drawn is 0.97% (95% CI 0–2.62), which is lower than the WHO global estimate of 4.2% and the Saudi Arabia study in pregnant women of 11.1%
8
but not significantly different from the regional population estimate for MENA (Figure 1). The low prevalence of chlamydia could be due to conservative cultural and social norms stressing the importance of fidelity in marriage; alternatively, some women may have declined recruitment and testing because they were aware they had STI symptoms or were worried they were at risk. The small number of infections detected in the study and the limited sexual behaviour measures we collected meant that we were unable to examine specific risk factors for infection.
Despite initial concerns that STIs are a sensitive sociocultural subject, we were encouraged to find acceptability for STI testing was high. And as measured by the majority of women who received their urine test results within 48 hours of enrolment, rapid intervention was also feasible. Apart from two instances, all enrolled women were able to provide an adequate, self-collected first-catch urine sample on their initial visit.
Women were recruited from a single publicly funded antenatal clinic in Muscat, which provides services for Omani women. As such, this sample may not represent expatriate or Omani women who elect to receive antenatal care from private health institutions. Furthermore, the lifestyles and attitudes of pregnant women living in Muscat may not reflect those living in rural or other communities elsewhere as over 50% of women in our study had received tertiary education. And because Al Wattayah antenatal clinic is a referral centre for complex pregnancies, women <25 years contributed only 9% to the cohort when younger age is a recognised risk factor for acquisition of STIs. Nevertheless, we were justified in recruiting an unselected group of women, irrespective of age or parity, as two of the women with chlamydia were in their mid-30s and multiparous.
While the majority of women found STI testing acceptable (Table 3), given the low prevalence of sexual infections in our study, the potential benefits and cost-effectiveness of testing will require further study in a wider range of antenatal settings.
A further concern, given the relatively low prevalence of gonorrhoea and chlamydia identified in this study, is the possibility of false-positive results from a lower PPV of the test than what we had anticipated. In retrospect, this could have been addressed by ensuring that a positive initial result was confirmed by retesting the sample with an alternative assay. In view of these findings, any future studies in this setting will need confirmatory tests using a different highly specific and sensitive assay. This is especially relevant when dual testing for chlamydia and gonorrhoea because the prevalence of gonococcal infection is lower than the prevalence of chlamydial infection, and the potential for false-positive N. gonorrhoeae results correspondingly greater. 15
Conclusion
This is the first study in Oman to assess testing of two important STIs in pregnant women. Despite our initial concerns, acceptability and feasibility were high. This exploratory study has helped us evaluate a framework for sentinel surveillance that, with methodological improvements, could be applied to other parts of Oman that may be at higher risk of STIs, as recommended by the WHO Global Health Sector Strategy on STIs (e.g. border towns, communities close to major transport hubs and corridors, as well as areas of social deprivation or high migration). 16 De-stigmatising STIs and normalising testing behaviour will better identify at-risk populations in Oman and inform policy and programming for culturally appropriate interventions that encompass prevention, treatment and control.
Supplemental Material
sj-pdf-1-std-10.1177_0956462421992263 – Supplemental Material for Acceptability and feasibility of testing for sexually transmitted infections among pregnant women in Muscat, Sultanate of Oman
Supplemental Material, sj-pdf-1-std-10.1177_0956462421992263 for Acceptability and feasibility of testing for sexually transmitted infections among pregnant women in Muscat, Sultanate of Oman by Richard Lau, Rula Eskander, Mubarak Al-Yaqoobi, Zeyana Al-Habsi, Ali Elgalib, Samir Shah, Maha Al-Fouri, Bader Al-Rawahi and Seif Al-Abri in Journal of International Journal of STD & AIDS
Footnotes
Acknowledgements
We thank the patients who participated in the study. The Xpert® CT/NG cartridges and urine specimen collection kits were kindly donated by Advance Healthcare Solution, Oman. The study would not have been possible without the dedication and support of the Al Wattayah antenatal team (Sisters Zainab Al-Wahaibi and Maimoona Al-Battashi, Drs Aditi Shinde, Dr Atika Al Hadhramy, Dr Abeer Al Hadhrami, Einas Al-Yaqoobi and Mrs Ruzaika Nasser (laboratory manager) and the microbiology team at Khoula Hospital (Mr Almuatasam Al-Barram and Ms Rahma Ali Al-Maaini)).
Author contributions
Zeyana Al-Habsi and Richard Lau were the principal investigators of the study. Rula Eskander was the antenatal clinical lead, and Mubarak Al-Yaqoobi was the microbiology lead. Ali Elgalib, Samir Shah, Maha Al-Fouri, Bader Al-Rawahi and Seif Al-Abri were involved in the initial design and discussion of the study proposal. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.