
Abstract
The World Health Organisation advice for post-partum women living with HIV (WLHs) in low- and middle-income countries is to breastfeed on suppressive antiretroviral treatment and use infant postnatal prophylaxis. In resource-rich settings, where formula feeding is safe, avoidance of breastfeed is advised. A questionnaire was created to survey attitudes to breastfeeding in WLHs in the United Kingdom. This was offered to all eligible pregnant women in the third trimester or within 3 months post-partum who attended HIV outpatient clinics from 2017 to 2018. Ninety-four women completed the questionnaire, 69% were Black African and 92% had an undetectable HIV viral load. Thirty eight percent stated they would like to breastfeed and 89% said they would breastfeed if they were HIV negative. Sixty two percent had community members question why they did not breastfeed, and 66% felt forced to invent a reason why they were not breastfeeding. Current UK guidelines recommend formula feeding, proposing a harm reduction approach to support women with suppressed HIV who wish to breastfeed. Over a third of respondents said they would like to breastfeed because stigma and secrecy remain an issue for WLHs. This suggests that over time more women may choose this option.
Background
Every year in the United Kingdom (UK), around 1200 women living with HIV (WLHs) become pregnant. 1 Vertical transmission (VT) can occur during pregnancy, birth or breastfeeding. Studies carried out in low- and middle-income countries (LMICs) showed that without antiretroviral therapy (ART), the risk of transmission of HIV through breastfeeding is approximately 16%. 2 Recent findings from the Promoting Maternal and Infant Survival Everywhere (PROMISE) study showed a 0.7% (95% confidence interval (CI) 0.3–1.4) risk of overall transmission at 1 year, where either the mother was on combination ART or the infant on daily nevirapine prophylaxis (iNVP) continued until 18 months after delivery or breastfeeding cessation, infant HIV-1 infection, or toxicity, whichever occurred first. 3 Factors that increase the risk of postnatal transmission include reduced adherence to ART by the mother, increased duration of breastfeeding, presence of mastitis and impaired gastrointestinal health of the mother and infant.4–7 ART is found at varying levels in breast milk, and the implications of this low level ART exposure for the infant remain unclear.8,9 If an infant acquires HIV in this setting, there is the risk of transmission of resistant virus, which may reduce options for treatment.
The British HIV Association (BHIVA) guidelines continue to recommend formula feeding for mothers living with HIV as there is zero risk of postnatal HIV transmission. 10 However, women on suppressive ART can be supported to breastfeed (BF) with additional monitoring of both the mother and baby. Availability of free or subsidised formula milk for WLHs who cannot afford this is variable across the UK and is mainly dependent on charitable funds.11,12
The World Health Organisation (WHO) recommends breastfeeding for women on suppressive ART due to increasing evidence that the risk of HIV transmission from breastfeeding is outweighed by the increased morbidity and mortality of non-breastfed infants in LMICs. 13 Encouragement of breastfeeding is also accepted as an important public health strategy due to its numerous benefits to the infant, both in the short term and long term, as well as the reduction of depression, breast and ovarian cancers in the mother.14,15 Similarly, the long-term risk of hypertension, type 2 diabetes mellitus and obesity is significantly lower in individuals who breastfed in infancy.16–18
In addition, there are a variety of social, financial and cultural pressures for women to breastfeed, which can cause difficulties for WLHs who are advised not to breastfeed. These pressures may cause personal distress, and difficult questions may arise about their reasons for not breastfeeding, which may on occasion result in breastfeeding against medical advice. 19 In one study, women felt an acute sense of personal loss and avoiding breastfeeding came at significant emotional cost. 19 One participant in this study chose to breastfeed against medical advice due to fear of disclosing her HIV status and financial constraints, arising from her uncertain immigration status with no leave to remain in the UK, and not being able to access public funds. 19 An evidence base and research into the prevalence of unreported breastfeeding in WLHs in the UK is lacking. There is also limited exploration of the views of women with HIV about breastfeeding, the cultural and social pressures to breastfeed they may experience and their understanding of the current national recommendations for women with HIV. The PACIFY study (Positive Attitudes Concerning Infant Feeding) sought to explore the views, concerns and issues surrounding breastfeeding in WLHs.
Methods
Study design
There were no previous questionnaires to explore this issue hence using formative research a six-page anonymised questionnaire was designed by the London HIV Pregnancy Network group with considerable input from WLHs.
We aimed to administer 100 questionnaires over a 6-month period from participants to assess views, concerns and attitudes towards breastfeeding in the UK. This was based on what was feasible in clinical services over the time period, taking into consideration participating clinics and pregnancy rates. The questionnaire received approval from Imperial College Healthcare NHS Trust Sexual Health and HIV Research Committee and North West London Research Ethics Committee (Integrated Research Application System (IRAS) number 221952).
Study settings and population
Participants were recruited by clinicians from 12 HIV clinics across England (South East, West Midlands and West Yorkshire) between June 2017 and June 2018. Participants were given the study patient information leaflet and consent form when they attended their regular pre- or postnatal outpatient appointment and, if they agreed to participate, they completed the anonymised questionnaire (Supplemental Appendix X) during the same visit. All the questionnaires were collated at Imperial College Healthcare NHS Trust.
Eligible participants were WLHs over the age of 18 years who were either within 3 months post-partum or in the third trimester of pregnancy and able to read and write in English.
Data collection
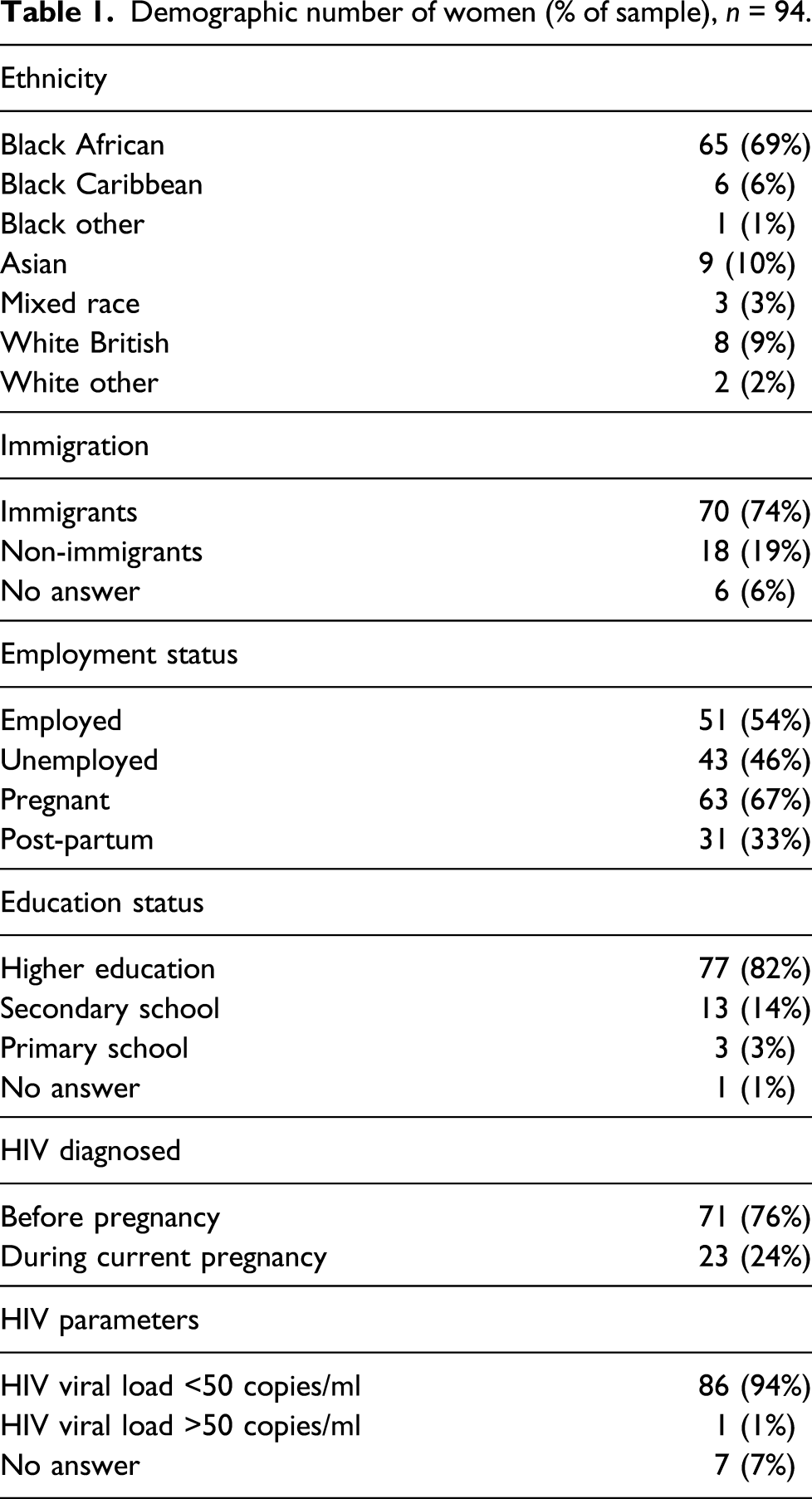
Demographic number of women (% of sample), n = 94.
Results
Of the 94 participants who completed the questionnaire, 69% (65/94) were Black African women and the median age was 36 years (IQR 31–39). Seventy four percent (70/94) identified as immigrants and 54% (51/94) were employed.
Two-thirds (63/94) were currently pregnant, and one-third (31/94) were post-partum. Twenty three percent (24/94) reported that they were diagnosed with HIV during the current pregnancy. Median CD4 count was 618 cells/mm3 and 92% (87/94) had an “undetectable” HIV viral load (<50 copies/ml).
Knowledge and experiences of breastfeeding among women living with HIV – expressed as number of women (% of sample), n = 94.
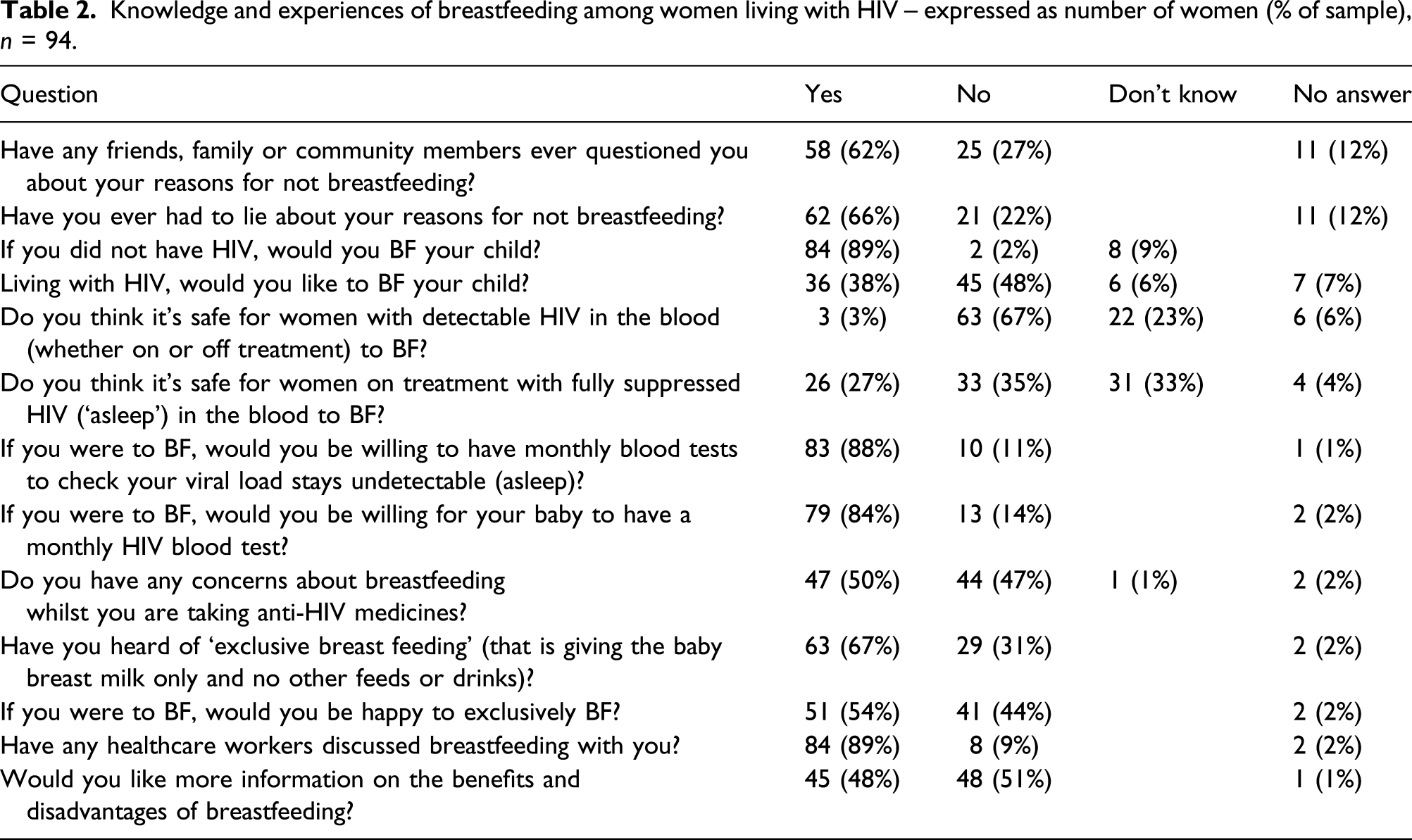
The majority of women reported that healthcare workers discussed breastfeeding with them, but the quality and depth of those conversations were unclear. Participants did not appear to fully understand that scenarios where breastfeeding could be supported were HIV viral load dependent. Only two-thirds of participants understood it was not safe to breastfeed with a detectable HIV viral load. Answers on whether it was safe to breastfeed with an undetectable HIV viral load were also variable, and a quarter of participants thought it was safe to do so.
Discussion
Significant differences between breastfeeding guidelines for WLHs in LMICs have caused confusion amongst WLHs in resource-rich settings. The World Health Organisation guidance for WLHs in LMICs is to breastfeed if on suppressive ART; however, BHIVA recommends formula feeding as this reduces the risk of postnatal transmission to zero.5,10 Currently in the UK, a WLH with fully suppressed viral load will be supported if she chooses to breastfeed, with the aim of minimising harm to herself and her infant. Recommendations include monthly clinic visits and blood tests for both the mother and baby during the duration of breastfeeding. 10 Over 80% of respondents said they found attending for monthly HIV viral loads acceptable; however, 5% of participants that agreed to this were concerned about the pressure of monthly blood tests on their baby.
Half of participants had concerns about breastfeeding while taking ART. Participants were concerned about passing on HIV and potential side effects of ART in breast milk. As already discussed, ART can be transmitted in breastmilk and the amount of ART present is dependent on the type of drug. 8 The consequences of this ongoing exposure are unknown, and if an infant were to have acquired HIV, there is a risk of transmitted viral resistance.
Participants highlighted that although they had discussions with clinicians around breastfeeding, they still wanted more information. Recent clinical trials have shown that sexual partners with undetectable HIV viral load (<200 copies/ml) for 6 months or more on suppressive ART have a zero risk of sexual transmission.20,21 This resulted in the launch of the Undetectable = Untransmittable campaign in 2016. More research is required into ascertaining whether this can also be applied to the infant exposure during breastfeeding; indeed, at present it cannot be said that U = U for breastfeeding.
The respondents to the PACIFY questionnaire certainly highlight the need for clinicians to give better information on breastfeeding and rationale of current guidelines, so women have a clear understanding of how best to make their choice for infant feeding.
Over half of participants had friends, family and community members who questioned why they were not intending to breast feed, and two-thirds of participants had to invent reasons for not breastfeeding. This highlights the fact that HIV stigma and secrecy remain a significant issue for WLHs in their choice of infant feeding, and as clinicians, we should be mindful of this. An analysis of global breastfeeding prevalence found that in the UK, only 34% of babies are receiving some breast milk at 6 months, which is amongst the lowest rates in Europe. 22 Studies in LMICs show that extended family and community members contribute to decision-making around infant feeding.23,24 Culturally, in these settings, the expectation is that women will choose to breastfeed and not breastfeeding may be considered a way of disclosing their HIV status.23–25 It is also important to consider the immigration status of patients as they may be at risk of deportation to LMICs where guidance and cultural settings, as well as the risk/benefit for BF, may be different. Provision of peer support may certainly help women to mitigate some of the hurdles discussed above. 26
Limitations
Our study involved completion of a questionnaire, and although there were patient and public involvement in the creation of the questionnaire, there is always the potential that some of the questions may have been misunderstood, leading to incorrect or no answers being provided. We did not ask participants’ questions on whether they had any HIV-infected children or where their children were born. This may have affected responses to our questionnaire. Our sample size may have been small but provides preliminary data for future qualitative research which can explore emotional and more complex psycho-social aspects for WLHs concerning breastfeeding.
Unfortunately, it was not possible to ascertain the number of women who refused to complete the questionnaire, their demographics or their reasons for refusal, although this was rare, according to clinic staff. This may have led to our sample being unrepresentative; however, the questionnaire was offered to all eligible women who attended the participating clinics within research time frame.
Conclusion
Whether “Undetectable = Untransmittable” (U = U) for breastfeeding cannot yet be affirmed, however even in this context, WLHs on suppressive ART may still want to breastfeed. Stigma and secrecy remain an important issue for the women who felt compelled to disguise their reasons for not breastfeeding. This questionnaire has highlighted that HIV clinicians in resource-rich settings should have more open dialogue with women around current evidence on breastfeeding with HIV, including the risks and benefits of breastfeeding on suppressive ART, as well as the consequences of stigma. Support, both clinical and peer mentor, for women who choose to breastfeed is essential, to minimise any risk to themselves or their infants.
Supplemental Material
sj-pdf-1-std-10.1177_0956462421999951 – Supplemental Material for Over a third of childbearing women with HIV would like to breastfeed: A UK survey of women living with HIV
Supplemental Material, sj-pdf-1-std-10.1177_0956462421999951 for Over a third of childbearing women with HIV would like to breastfeed: A UK survey of women living with HIV by Farai Nyatsanza, Jessica Gubbin, Thomas Gubbin, Paula Seery, Pippa Farrugia, Adam Croucher, Yvonne Gilleece, Melanie Rosenvinge, Sherie Roedling, Liat Sarner, Dayawathie Nayagam, Clare Stradling, Angelina Namiba, Nicola Fearnley, and Hermione Lyall in International Journal of STD & AIDS
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.