
Abstract
Background
In rare cases, people living with chronic human immunodeficiency virus (HIV) infection do not develop antibodies despite demonstrable infection. Delayed or missed diagnosis of HIV infection leads to a lack of timely therapy, resulting in rapid disease progression with opportunistic infections or malignancies.
Case Report
A 44-year-old Chinese man presented with sore throat, oral leukoplakia, fever, dyspnoea and diffuse ground glass-like lesions in both lungs. Serum cytomegalovirus DNA was detectable, and CD4+ T-cell count was low. The patient was suspected of being a person living with HIV despite of the repeatedly negative HIV antibody tests using enzyme-linked immunsorbent assay and Western blot. Subsequently, high-plasma HIV RNA viral load was found on two repeated tests, while HIV DNA was also positive. Thus, the patient was confirmed as presenting with HIV-seronegative acquired immunodeficiency syndrome (AIDS). The symptoms improved in response to effective anti-fungal and anti-retroviral therapy after diagnosis.
Conclusion
This is the third reported case of an HIV-seronegative AIDS patient in China, which are also rarely reported globally. HIV nucleic acid testing is important to screen out HIV infection, especially in those who present with severe immunodeficiency but remain HIV serogenative.
Introduction
It may be insufficient to diagnose all subjects with HIV infection by detecting HIV antibodies alone. 1 In rare cases, people living with chronic HIV infection do not develop antibodies despite demonstrable infection.
Case presentation
On 17 June 2021, a 44-year-old Chinese man presented to our hospital with complaints of sore throat and ulcerous stomatitis for two months, and fever for two weeks. He reported a history of psoriasis, and underwent 300 mg infliximab intravenous infusion in March and April 2021 thrice. Two days after his last injection, his illness started with a sore throat and ulcerous stomatitis. He was treated with oral antibiotics for one month without improvement. On 3 June 2021, he developed oral leukoplakia and low-grade fever, and was admitted to a local general hospital. An ELISA result was negative for HIV-1 antibody. He was clinically diagnosed with oral Candida albicans infection, and was treated with nystatin and fluconazole for two weeks. Sore throat and oral leukoplakia was improved. However, he developed high-grade fever with chills.
At our hospital, physical examination revealed fever (39.3°C) and shortness of breath. On June 18, the examinations upon admission showed white blood cell (WBC), 8.12×109/L; lymphocyte ratio, 37.4%; CD4+ T cells, 360/μL; and CD8+ T cells, 1190/μL. The immunoglobulin (Ig) series showed IgG, 10.30 g/L (normal range: 7–16 g/L); IgA, 2.58 g/L (normal range: 0.7–4 g/L); and IgM, 2.53 g/L (normal range: 0.4–2.3 g/L). The result of HIV-1 antibody was negative, and so were antibodies for Toxoplasma gondii, rubella virus, Cytomegalovirus (CMV), herpes simplex virus-1/2, syphilis, hepatitis viruses, tuberculosis and autoimmune diseases. Tuberculin pure protein derivative test T-SPOT TB test were negative. Serum Epstein-Barr virus DNA was undetectable, but CMV DNA was detectable. Chest CT showed diffuse ground glass-like lesions in both lungs (Figure 1(a)). Treatment was initiated with voriconazole, but his condition deteriorated. The extent of pulmonary infection increased (Figure 1(b)). On June 26, his WBC reduced to 3.76×109/L (lymphocyte ratio: 20.2%), CD4+ T cells count reduced to 115/μL; CD8+ T cells, 420/μL; and B cells, 39/μL. On revisiting the medical history, the patient reported unprotected male-male sexual contacts two years ago prior. HIV-1 antigen-antibody complex test was then performed twice by an automatic fourth generation assay kit (HIV-1 p24 antigen; HIV-1 gp41, HIV-1 sub.O, HIV-2 gp36; Sysmex Corporation, Shanghai, China) and by a manual fourth generation assay kit (HIV-1 p24 antigen; HIV-1 1A98 and HIV-2 1B16; InTec Products, Xiamen, Fujian Province, China), respectively, but the result was still negative. Importantly, HIV nucleic acid results showed plasma HIV RNA 1.85×107 IU/mL and HIV DNA 4.14×104 copies/mL reported on June 26. Blood sample was also sent to Xi’an Center for Disease Control and Prevention. HIV-1 antibody test by Western blot was negative, but HIV RNA was 2.00×106 IU/mL reported on June 27. Thus, HIV infection was confirmed. Antiretroviral therapy was started with elvitegravir, cobicistat, emtricitabine, and tenofovir alafenamide fumarate. Treatment for pulmonary infection was changed to trimethoprim/sulfamethoxazole, caspofungin, and clindamycin. The fever resolved and radiological appearances of pneumonia improved (Figure 1(c)), and he was discharged on 17 July 2021. The blood sample of the patient was sent for HIV RNA sequencing. The viral subtype was B+C, and no drug resistance was found (Supplementary data). On October 26, the patient received another HIV-1 antigen-antibody complex test 3 months after antiretroviral therapy initiation. The result was indeterminate in a grey zone. Serial chest computed tomography examination showed (a) diffuse ground glass-like lesions in both lungs, (b) enlarged extent of pulmonary infection, and (c) improved condition of pneumonia.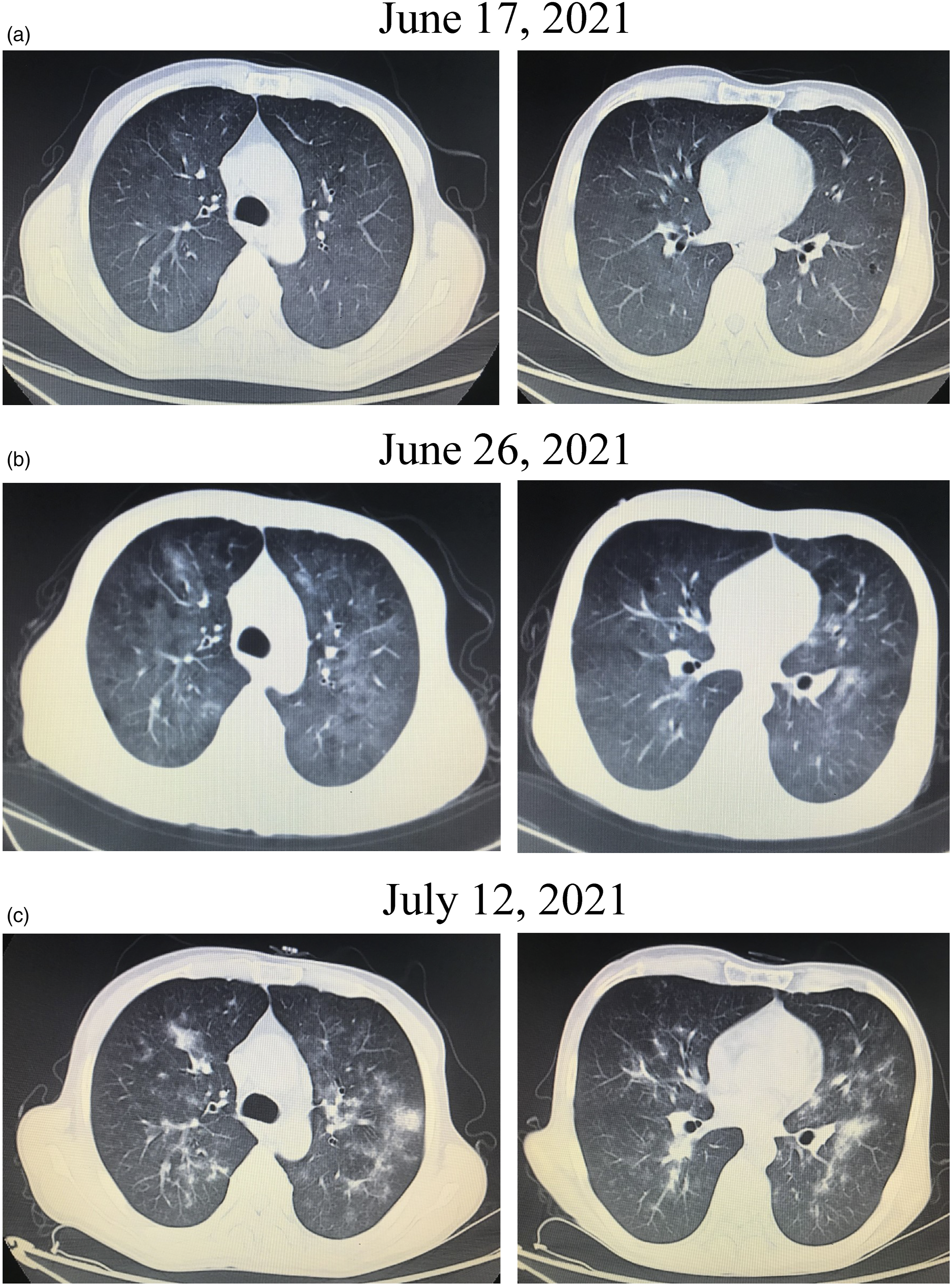
Discussion
Seronegative HIV infection rarely occurs beyond an acute infection phase. Twenty-eight cases of seronegative chronic HIV infection have been reported globally, 2 and two of them were Chinese.3,4 All patients presented as immunocompromised, and were diagnosed by HIV viral load test and/or viral culture. Most of the patients showed rapid disease progression and poor prognosis. However, the second reported case in China, who presented as Pneumocystis jirovecii pneumonia (PJP), improved due to rapid diagnosis of AIDS and early administration of antiretroviral therapy. 4 Similarly, our patient was diagnosed with AIDS 10 days post admission, and antiretroviral therapy was immediately administrated. Effective anti-fungal strategy also contributed to the improvement. Thus, it is pivotal for early diagnosis of HIV infection in immunocompromised patients who were even seronegative for HIV antibodies.
The reasons for HIV seronegativity in patients presenting with AIDS are still not fully understood. The most probable reason may be infection with rare HIV strains, 5 which could not be detected by the current HIV antibody screening methods. These rare strains displayed strict geographic distributions. However, our patient never travelled abroad and showed a B+C subtype, which he may have acquired 2 years before presentation. Moreover, the patient showed normal Ig levels, but both T cells and B cells were profoundly down-regulated. Immune cells functional deficiency might contribute to defects on antibody secretion. 6 However, two kits which detect both antigen and antibody did not detect viral antigen when virus RNA and DNA are clearly found. This might partly be due to the insufficient or low affinity of tested antibodies. Furthermore, the patient developed immunocompromise shortly after administration of infliximab, a TNF-α antagonist for psoriasis treatment. Anti-TNF-α therapy seemed to be well tolerated in people living with HIV, 7 but infliximab could induce opportunistic infections, such as histoplasmosis, 8 Mycobacterium marinum infection 9 and Listeria monocytogenes meningitis. 10 Thus, infliximab administration might contribute to HIV activation and AIDS progression. Use of immunosuppressive therapy may give rise to atypical presentation of HIV-1 infection.
The patient suffered with opportunistic infections, and initially diagnosed as oral Candida albicans infection. Chest CT manifested as interstitial pneumonia, which might be induced by systemic active cytomegalovirus and/or fungal infection. Due to the history of potential Candida albicans infection, he was primarily treated by a broad-spectrum anti-fungal agent. However, his condition worsened. Both sepsis/drug therapy and rapid progressive HIV-1 infection might contribute to the decline in CD4+ T cell count and disease progression. Thus, we changed the anti-fungal agents mainly targeting Pneumocystis jirovecii after confirmation of HIV infection. Combined with antiretroviral therapy, the anti-PJP strategy improved the patient’s condition. We did not use anti-CMV drugs, but CMV DNA was undetectable when discharged. Thus, Pneumocystis jirovecii infection was probably the main cause of pulmonary infection in this patient.
Here we report the third case of HIV-seronegative AIDS in China. HIV nucleic acid testing is important to screen out HIV infection, especially in those who are in immunocompromised condition and present with severe immunodeficiency.
Supplemental Material
sj-pdf-1-std-10.1177_09564624221074507 – Supplemental Material for A human immunodeficiency virus-seronegative acquired immunodeficiency syndrome patient with opportunistic infections: A case report
Supplemental Material, sj-pdf-1-std-10.1177_09564624221074507 for A human immunodeficiency virus-seronegative acquired immunodeficiency syndrome patient with opportunistic infections: A case report by Ye Zhang, Yuan-Yuan Wang, Xiao-Feng Li, Chun-Yan Ma, Jing Li, Wen Kang, Wen-Zhen Kang, Lin-Xu Wang, Chang-Xing Huang, Yong-Tao Sun and Jian-Qi Liana in International Journal of STD & AIDS
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Patient consent has been obtained for this report.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.