
Abstract
Background
We provided sexually transmitted infection (STI) screening and facilitated partner notification and treatment among women participating in a periconception HIV prevention program in southwestern Uganda to understand follow-up STI incidence.
Methods
Women at-risk for HIV exposure while planning for pregnancy completed laboratory screening for chlamydia, gonorrhea, trichomoniasis, and syphilis at enrollment and 6 months of follow-up and/or incident pregnancy; facilitated partner notification and treatment were offered for those with positive tests. We performed a logistic regression to determine correlates of follow-up STI.
Results
Ninety-four participants completed enrollment STI screening with a median age of 29 (IQR 26–34); 23 (24%) had ≥1 STI. Of the 23 participants with enrollment STI(s), all completed treatment and 19 (83%) returned for follow-up; 18 (78%) reported delivering partner notification cards and discussing STIs with partner(s), and 14 (61%) reported all partners received STI treatment. Of the 81 (86%) who successfully completed follow-up STI screening, 17 (21%) had ≥1 STI. The STI incidence rate was 29.0 per 100 person-years. In univariable regression analysis, enrollment STI, younger age, less education, and alcohol consumption were all significantly associated with follow-up STI.
Conclusions
We demonstrated high enrollment and follow-up STI rates and moderate participant-reported partner treatment among women planning for pregnancy in Uganda despite partner notification and treatment. Novel STI partner notification and treatment interventions are needed to decrease the STI burden, especially among women planning for and with pregnancy.
Keywords
Introduction
In 2020, an estimated 374 million curable sexually transmitted infections (STI) occurred globally, including Chlamydia trachomatis (chlamydia), Neisseria gonorrhoeae (gonorrhea), Trichomonas vaginalis (trichomoniasis), and Treponema pallidum (syphilis). 1 The World Health Organization (WHO) identified the African Region as having the highest STI burden, with an estimated 96 million STIs diagnosed in 2020. 1
Reasons for the high global STI prevalence and incidence are likely multifactorial. The STI burden in sub-Saharan Africa and elsewhere is due in part to HIV and curable STI synergy, with HIV increasing the transmission and acquisition of STIs and vice versa.2,3 Additionally, in many resource-limited settings, STI laboratory diagnostics are unavailable due to low laboratory capacity and prohibitive costs. Instead, STIs are managed syndromically, where individuals with STI symptoms are diagnosed and treated according to WHO-defined STI syndromes.4,5 Syndromic management can lead to both over and underdiagnosis of STIs. 6 Accordingly, in much of the world there is ambiguity around STI diagnosis, complicating STI treatment, cure, and partner notification.7–9 Untreated STIs contribute to a high STI incidence, 10 and those who do receive STI treatment without adequate screening and/or treatment of sexual partners risk STI reinfection. 11 Thus, more comprehensive STI treatment programs are needed, especially as point-of-care STI diagnostics are developed and disseminated.12,13
STIs are particularly concerning among pregnant women and women planning for pregnancy, since untreated STIs can cause significant neonatal morbidity and mortality.14,15 STI management in pregnancy is perhaps most pressing in sub-Saharan Africa because this region carries the highest, global, fertility rates in addition to having the highest STI incidence and HIV prevalence. For example, in Uganda, the 2020 estimated fertility rate was 4.7 children per woman. 16 The STI acquisition risk is only exacerbated among women planning for pregnancy given the need to engage in condomless sex to conceive. However, little is known about STI incidence in sub-Saharan Africa, its associated correlates, and prevention methods among women. One strategy for STI prevention is partner notification and treatment to prevent ongoing STI transmission and post-treatment reinfection, though data linking partner notification and treatment to STI incidence is mixed and real-world practices vary. Understanding STI incidence, correlates, and prevention methods are critical to developing sexual and reproductive healthcare. HIV and pre-exposure prophylaxis (PrEP) programs provide an opportunity for such STI care delivery and integration.
We conducted a longitudinal cohort study in southwestern, rural Uganda among women at risk for HIV exposure, with pregnancy plans, and participating in a periconception HIV prevention program. For those with an enrollment STI, we monitored partner notification and STI treatment. All women were assessed for STI at 6-months and/or incident pregnancy. Our aims were to demonstrate: (1) follow-up STI incidence and correlates, (2) a modified STI care cascade incorporating STI partner notification and treatment, as developed by our team.17,18
Methods
Parent study design and participants
This study was embedded in the Healthy Families PrEP Study (NCT03832530), a mixed-methods, prospective cohort study with the primary aim of assessing PrEP uptake and adherence among a cohort of women at risk for periconception HIV exposure. Participants were women living in rural, southwestern Uganda, age 18–40, without HIV, in a relationship with a man living with HIV or of unknown HIV serostatus, and with personal or partner plans to conceive a child in the next year; all were fluent in the local language (Runyankole) or English. Potential participants were recruited through the Mbarara Regional Referral Hospital (MRRH) 19 HIV clinic and surrounding clinics, including Mbarara Municipal Council, Bwizibwera, Kinoni, Kakoba, and the general MRRH outpatient clinics.
Parent study procedures
Participants were recruited from January 2018 to April 2019 and attended study visits at enrollment and every 3 months. Participants with incident pregnancy were followed through pregnancy completion. Participants exited the study at 9 months if not yet pregnant, after pregnancy outcome, or if they acquired HIV.
Laboratory screening
Etiologic STI laboratory screening was added to the protocol for all new enrollments starting June 2018; this analysis is limited to participants who underwent this screening. Participants underwent etiologic STI screening at enrollment and 6-months and/or incident pregnancy. Participants provided self-collected or nurse-collected vaginal swabs for chlamydia, gonorrhea, and trichomoniasis screening via NAAT with GeneXpert. For syphilis, participants provided blood for immunochromatographic testing to screen for treponemal antibodies with confirmation testing via rapid plasma reagin (RPR) to screen for non-treponemal antibodies. Due to power instability and resource constraints, GeneXpert screening was not always performed same-day and took place within 6 weeks of sample collection. Vaginal specimens were stored in GeneXpert chlamydia/gonorrhea and trichomoniasis tubes at 2–15 degrees Celsius. Syphilis was diagnosed per the US Centers for Disease Control and Prevention (CDC) Guidelines. 20 All participants completed rapid HIV testing and pregnancy testing with urine HCG at each study visit.
STI treatment
Participants who underwent etiologic STI screening were notified of their results and those with an STI were instructed to return to the study site where they were offered free STI treatment and STI counseling including partner notification and treatment. All participants with STI were offered partner notification cards that outlined potential partner STI exposure, treatment recommendations, and informed partners that they could receive free treatment through the study. Participants with chlamydia, gonorrhea, and trichomoniasis were offered patient-delivered partner medication to take to partners with potential STI exposure. All STI and partner notification practices were in accordance with the Ugandan Ministry of Health guidelines. 21
Counseling and questionnaires
At each study visit, participants were offered safer conception care and counseling consisting of safer conception strategies, PrEP adherence, and STI prevention and treatment. At each visit, all participants also underwent STI syndromic screening by a study nurse per the Ugandan Ministry of Health guidelines. Participants completed a comprehensive questionnaire administered by a research assistant at study enrollment and exit that included questions on demographics, relationship/sexual history, and STI history. Participants enrolled after the addition of etiologic STI screening completed an additional STI partner notification questionnaire during their follow-up STI screening timepoint at either 6-months or incident pregnancy.
Measures
The primary outcome of this study was “follow-up STI”, defined as any STI measured at the follow-up timepoint of 6-months and/or incident pregnancy. Follow-up STIs were classified as “recurrent STI” if participants had the same STI at enrollment and follow-up, “different STI” if participants had an STI at enrollment and a different STI at follow-up, and “new STI” if participants did not have an STI at enrollment and had an STI at follow-up “(Supplementary Figure 1)”. The primary analysis of “incident STI” included person-years from all participants who completed follow-up STI screening in the denominator; however, events were only included for participants with “different STI” and “new STI” in the numerator. This method of analysis is based on a conservative approach that excluded “recurrent STI” events due to the possibility that these STIs could be persistent infections and is consistent with prior analyses.11,22 The sensitivity analysis of “incident STI” included person-years from all participants who completed follow-up STI screening in the denominator and included events for participants with “recurrent STI”, “different STI”, and “new STI” in the numerator. Additional outcomes were the proportion of participants who reported partner notification and partner treatment among participants with enrollment STI.
Statistical analysis
We compared participants characteristics who did and did not return for follow-up visits using Wilcoxon rank sum tests for continuous variables and Fisher’s exact tests for categorical variables. We used the same methods to compare characteristics of participants with and without follow-up STI. We calculated incidence rates for follow-up STI as well as a sensitivity analysis, defined above. We performed a univariable logistic regression to determine follow-up STI correlates. Covariates were considered significant at the α=0.05 level. Due to a small number of follow-up STIs, a multivariable regression could not be performed. Instead, bivariable logistic regression analyses were conducted with the primary covariate of interest, enrollment STI, along with key covariates that have previously been shown to correlate with STI, including age, education, alcohol consumption, pregnancy, and PrEP use.22–24 Data were analyzed with Stata version 15.
Ethics
All participants provided verbal and written informed consent to participate in study procedures. Ethical approval was obtained from Mass General Brigham, the University of Alabama at Birmingham, and Mbarara University of Science and Technology. Additional regulatory approval was also obtained from the Uganda National Council of Science and Technology.
Results
Participant enrollment STI prevalence and follow-up visit retention
Participant characteristics at study exit by presence of 6M incident STI among women at-risk for HIV acquisition while planning for pregnancy and participating in a periconception HIV prevention program.

*The sexual and relationship power scale is a summation of 23 questions.
Enrollment STI care cascade from participant diagnosis to partner treatment
Among the 94 participants who completed etiologic STI screening at enrollment, 23 had an STI and all received treatment at the study site (Figure 1). Of the 23 participants with enrollment STI, 19 (83%) returned for follow-up STI screening. 18 of the 23 participants (78%) reported distributing partner notification cards and discussing their STI diagnosis with all sexual partners. One participant did not deliver her partner notification card due to fear of intimate partner violence. 14 participants (61%) reported that all partners received STI treatment; 13 participants reported that partners took the patient-delivered partner medications and one participant reported her partner sought medical treatment at a clinic. STI care cascade among women diagnosed with enrollment STI, at-risk for HIV acquisition while planning for pregnancy and participating in a periconception HIV prevention program.
Participant enrollment STI prevalence in relation to follow-up STI
Of the 94 participants who completed etiologic STI screening at enrollment, 23 had an STI. Among the 23 participants with an enrollment STI, 9 (39%) did not have a follow-up STI (i.e., achieved STI cure), 6 (26%) had a recurrent STI with the same pathogen, 5 (22%) had a different STI, 3 (13%) were lost to follow-up or electively exited the study prematurely, and 1 (4%) did not complete follow-up STI screening (1 participant had STI coinfection and thus had both recurrent STI and STI with a different pathogen). Among the 71 participants with no enrollment STI, 55 (77%) had no follow-up STI, 7 (10%) had a new STI, 6 (8%) were lost to follow-up or electively exited the study prematurely, and 3 (4%) did not complete follow-up STI screening (Figure 2). Schematic of prevalent, enrollment STI and outcomes of follow-up STI screening among women at-risk for HIV acquisition while planning for pregnancy and participating in a periconception HIV prevention program.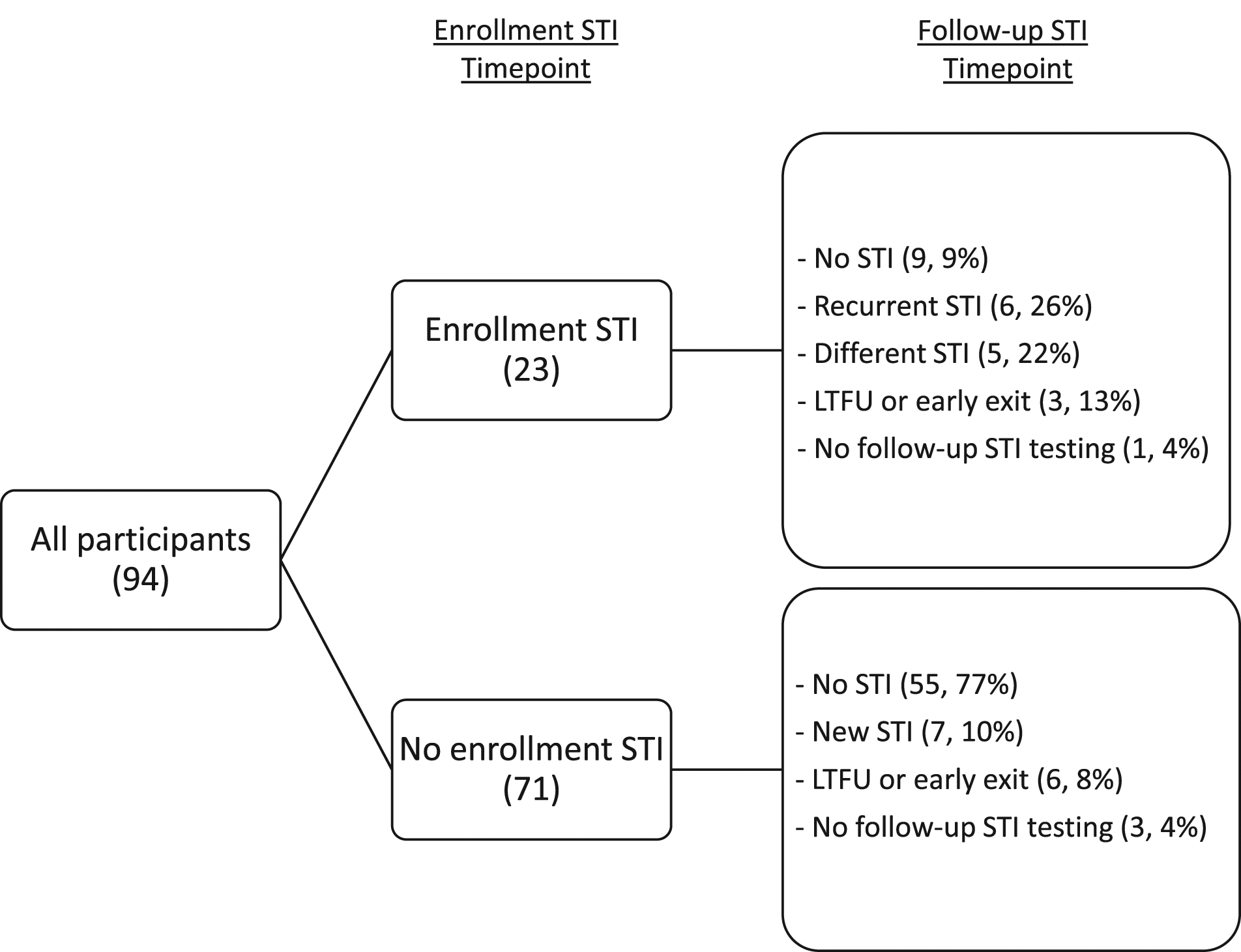
Follow-up STI and STI incidence
The median person-time to follow-up STI screening was 182 days. Of the 81 participants who completed follow-up STI screening, 17 (21%) participants had 1 or more STIs including 5 with chlamydia (6%), 4 (5%) with gonorrhea, 3 (4%) with trichomoniasis, and 6 (7%) with syphilis (1 participant had co-infection with chlamydia and gonorrhea) (Figure 3). The proportion of follow-up STIs among participants who reported enrollment STI partner treatment (6/14; 43% - 4 recurrent STIs, 3 different STIs [one participant had STI coinfection]) was smaller compared to those who did not report enrollment STI partner treatment (3/4; 75% - 2 recurrent STIs, 1 different STI), though these findings were not statistically different (p = .58). The primary analysis demonstrated an STI incidence rate of 29.00 per 100 person-years. The sensitivity analysis demonstrated an STI incidence rate of 41.05 per 100 person-years. Notably, one participant who was diagnosed with and completed treatment for enrollment syphilis and 6-month gonorrhea was found to have acquired HIV at her 9 month follow-up. Enrollment and follow-up STI among women at-risk for HIV acquisition while planning for pregnancy and participating in a periconception HIV prevention program. *One participant had STI coinfection with chlamydia and gonorrhea at follow-up testing.
Follow-up STI correlates
Factors associated with follow-up STI using univariable linear regression among women at-risk for HIV acquisition while planning for pregnancy and participating in a periconception HIV prevention program.

*Bold font indicates statistically significant values (p = .05).
Discussion
We demonstrated a high enrollment STI prevalence and incidence rate despite comprehensively supporting participant treatment and partner notification and treatment with counseling, partner notification cards, and patient-delivered partner medications. Further, among participants with enrollment STI, approximately 50% had an STI at the follow-up timepoint with half of this group having the same STI at enrollment and follow-up, raising concern for reinfection or persistent infection. Finally, we demonstrated moderate participant-reported partner notification and treatment. All participants in this cohort were at risk for HIV exposure while planning for pregnancy with 22% having an incident pregnancy during the study period and 1% having HIV seroconversion. Women in the periconception period are an important group for HIV/STI acquisition given common engagement in condomless sex and potential for subsequent morbidity for women and infants.25–27 These data emphasize that risk and demonstrate the need for increased STI care for women prior to and during pregnancy in sub-Saharan Africa and elsewhere.
The high STI incidence rate among women at risk for HIV exposure while planning for pregnancy is consistent with the few studies assessing STI incidence in sub-Saharan Africa. Two South African studies screened women with and without HIV for chlamydia, gonorrhea, and trichomoniasis using vulvovaginal swabs via polymerase chain reaction assays at the first antenatal clinic visit and postpartum. These studies found an enrollment STI prevalence ranging from 27-40% and an STI incidence rate ranging from 15 to 43.8 per 100 person-years.11,22 In comparison, our study of women without HIV found an STI prevalence of 24%. Our STI incidence rate of 29.00 or 41.05 (depending on the definition of incident STI) per 100 person-years was high for a population without HIV and who had received comprehensive partner notification and treatment support. Potential factors contributing to high STI incidence and recurrence include our study screening for syphilis, which the two South African studies did not include. The high syphilis prevalence at our testing site 28 coupled with the testing limitations of demonstrating syphilis infection resolution likely contributed to our high STI recurrence. Additionally, our study population’s pregnancy plans and PrEP use likely contributed to the high proportion of participants engaging in condomless sex and increased STI transmission and acquisition.
Nearly all participants attending follow-up visits self-reported partner notification, and participants with self-reported partner treatment had fewer follow-up STIs compared to participants without self-reported partner treatment. A South African randomized controlled trial compared STI education sessions, sexual risk reduction sessions, and enhanced partner notification sessions (the most robust intervention). Participants with STI in the enhanced partner notification arm referred 10% more partners to clinic compared to other groups, though this increase in partner referral did not translate to decreased 12-month STI incidence. A major limitation was the reliance on syndromic management. 29 A systematic review also found mixed results regarding the effect of partner referral on persistent or recurrent STI. However, this same review analyzed five studies and found that participants randomized to patient-delivered partner medication trial arms had decreased persistent or recurrent STI compared to control group participants30,31 with a risk ratio of 0.73 (CI 0.57–0.93). While our study was not powered to assess the effect of STI partner notification and treatment on follow-up STI, we found a signal that patient-delivered partner medications decreased follow-up STI.
We found that enrollment STI, younger age, less education, and alcohol consumption were significantly associated with follow-up STI in univariable regression analyses. These factors have previously been associated with STI.22,23,32 It is unclear whether “recurrent STIs” indicate persistent infection or reinfection. However, persistent infection is less likely because all participants with enrollment STI reported taking free STI treatment through our study. Additionally, persistent infection due to antimicrobial resistance is unlikely as Uganda has low rates of gonorrhea resistance. 33 The diagnosis of recurrence was most challenging for syphilis, given the diagnostic limitations of treponemal and non-treponemal syphilis testing, though we followed US CDC guidelines. 20 Notably, research across the world has demonstrated that prior STI and multiple partners are major predictors of subsequent STI.10,34
Limitations
A major limitation of our study is the small sample size. However, given the few studies on STI incidence, and fewer still among women planning for pregnancy, our study addresses important knowledge gaps. Compared to participants who attended follow-up study visits, participants who did not return for follow-up were younger, had fewer pregnancies, and increased condomless sex, indicating this latter group may have increased risk for follow-up STI and our study may have underestimated STI. Additionally, this study is limited by participant self-report of partner notification and treatment data which can lead to overestimates due to social desirability bias and underestimates due to participant knowledge deficits of partners’ sexual behavior and care. Our study had several strengths including the use of etiologic STI diagnostics and comprehensive partner notification and treatment methods. Finally, since there is no standard method for defining STI incidence, our analysis analyzed “incident STI” using two methods to better understand and facilitate literature comparisons.
Conclusions
Our study is one of the first to measure etiologic, laboratory diagnosed STIs longitudinally among a cohort of women at risk for HIV exposure while planning for pregnancy and considering PrEP uptake. We demonstrated high enrollment STI prevalence as well as high follow-up STI despite optimizing partner notification and treatment. Much STI research has focused on pregnant women, but given that prior STI is predictive of subsequent STI, we recommend increased focus on people planning for pregnancy. Novel STI prevention and surveillance methods are needed for this population to prevent perinatal STI transmission and support the health of women and their families.
Supplemental Material
Supplemental Material - STI prevalence, incidence, and partner notification among women in a periconception HIV prevention program in Uganda
Supplemental Material for STI prevalence, incidence, and partner notification among women in a periconception HIV prevention program in Uganda by Pooja Chitneni, Winnie Muyindike, Mwebesa Bosco Bwana, Moran Owembabazi, Kasey O’Neil, Paul Kato Kalyebara, Bethany Hedt-Gauthier, David R Bangsberg, Jeanne M Marrazzo, Angela Kaida, Jessica E Haberer and Lynn T Matthews in International Journal of STD & AIDS
Footnotes
Acknowledgements
We would like to thank our participants for their contributions to this study. We would also like to thank several colleagues including, Deogratious Tukwasibwe, Alice Najjuma, JohnMary Tumwine, Catherine Kyampire, Sylvia Natukynda, Adolf Byamukama, Yona Mbalibulha.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study is funded through the Doris Duke Charitable Foundation. PC received funding from the National Institute of Allergy and Infectious Diseases under award number T32 AI007433, and from the Fogarty International Center and National Institute of Mental Health under award number D43 TW010543 all under the National Institutes of Health. JEH is supported by K24MH114732. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author’s note
Conflicts of Interest and Source of Funding: Cepheid Inc. provided GeneXpert cartridge donation and Gilead Sciences provided pre-exposure prophylaxis (TDF/FTC PrEP).
Data availability
Raw data were generated at Mbarara University of Science and Technology. Derived data supporting the findings of this study are available from the corresponding author PC on request.
Supplemental material
Supplement material for this article is available in online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.