
Abstract
Background
Non-occupational Post-Exposure Prophylaxis (nPEP) is an effective HIV prevention strategy in gay and bisexual men (GBM) taken after possible exposure. HIV Pre-Exposure Prophylaxis (PrEP) is also a highly effective HIV prevention strategy.
Methods
A retrospective audit of medical records of GBM presenting to a sexual health centre and provided with nPEP compared two periods to determine if nPEP usage changed following availability of PrEP. In the first period (P1) PrEP was available through extended trials. In the second period (P2) PrEP became more accessible through the Australian Pharmaceutical Benefits Scheme (PBS). Period comparisons were performed using a two-population test of proportions with one-tailed testing and significance set at P < .05 using SPSS Statistics Version 25.
Results
There were 232 GBM provided with nPEP in P1, and 202 in P2. A two-population test of proportions demonstrated that GBM presentations for nPEP decreased significantly from 302/4779 (6.3%) of GBM visits in P1 to 221/7205 (3.1%) in P2 when PrEP was more accessible (Z=8.53, P < .001). PrEP uptake after presenting for nPEP increased from 30 (12.9%) of total GBM visits in P1 to 69 (34.2%) in P2 (Z=5.26, p < .001).
Conclusions
GBM accessing nPEP decreased with statistical significance post introduction of PBS PrEP.
Keywords
Introduction
The HIV landscape has changed in Australia in the last five years with a 37 per cent reduction in the rate of new HIV diagnoses, and a 44 per cent reduction of new HIV diagnoses among gay and bisexual men (GBM). 1 Factors contributing to declining HIV diagnoses include increased HIV testing, early commencement of HIV treatments and a high uptake of PrEP in GBM.2–4 Australia is recognised as a leader in biomedical HIV prevention and has enabled access to HIV preventative strategies including occupational Post-Exposure Prophylaxis (PEP), non-occupational Post Exposure Prophylaxis (nPEP) and more recently, HIV Pre-Exposure Prophylaxis (PrEP).5–7
Biomedical prophylaxis against HIV has been used as a preventative measure since the late 1980s when HIV antiretroviral drugs were first used as PEP following occupational exposure to HIV. 8 Use has continued as an effective preventative measure for both occupational and non-occupational exposure to HIV. 9 nPEP is indicated after potential exposure to HIV via sex, shared injecting drug equipment, and mucous membrane or non-intact skin exposures. 5 Australia was one of the first countries to implement nPEP worldwide, with nPEP made available in New South Wales in 1998, Queensland in 1999 and Victoria and the Australian Capital Territory in 2001. 10 Australian guidelines recommend using either a 2-drug regimen of tenofovir disoproxil with lamivudine or emtricitabine or a 3-drug regimen consisting of a 2-drug regimen plus dolutegravir, raltegravir or rilpivirine, depending on the level of risk. nPEP should be initiated within 72 hours of HIV exposure, then taken daily for 28 days. 5
PrEP is a highly effective HIV prevention strategy and comprises the use of oral co-formulated tenofovir and emtricitabine taken by HIV-negative individuals who are at risk of HIV infection.7,11 Risks for HIV infection include serodiscordant sexual relationships in which the partner with HIV has a detectable viral load, having a bacterial sexually transmissible infection (STI), not using condoms, and sharing injecting equipment. 12 PrEP can be taken daily, or cis-gender men also have the option of on-demand dosing in line with sexual activity. 13 In 2016, tenofovir disoproxil combined with emtricitabine was approved for use in Australia as HIV PrEP, and was made available through large clinical trials, private prescription, or personal importation. 7 Medicare is the Australian universal healthcare system which subsidises costs associated with healthcare visits, laboratory and pharmaceutical costs for Australian citizens and permanent residents who hold a Medicare card. In April 2018, PrEP became available through the Australian Pharmaceutical Benefits Scheme (PBS) 14 which has enabled greater access to PrEP for those at risk of HIV who are Medicare eligible. Individuals born overseas who are not eligible for Medicare are unable to access subsidised PrEP, general practice visits or pathology testing in Australia, and may pay full price at an Australian pharmacy or access PrEP from international pharmacies or via charitable supply. 15
It is unclear whether nPEP use has lessened since widespread availability of PrEP. There is limited Australian exploration of this question, with one study of nPEP provision in South-East Queensland demonstrating a small but statistically significant decrease in nPEP in 2019 compared to 2016. 16
In the Australian Capital Territory (ACT) the majority of nPEP episodes are managed at one publicly funded sexual health centre, Canberra Sexual Health Centre (CSHC). Patients may present requesting nPEP, or the opportunity for nPEP may be identified by a clinician seeing the patient for other concerns. Patients may also be referred to the service for nPEP by other health professionals in the community, or for continuation of nPEP after commencement at one of the two ACT emergency departments or other emergency department or service within Australia or overseas. Additionally, individual patients may self-initiate nPEP from a personal supply of medication obtained from existing supply, which may include leftover nPEP or PrEP, or from another individual.
Objectives
This study aims to determine whether nPEP usage by GBM in the ACT changed after PrEP became available via clinical trial and listing on the PBS.
We hypothesize that there has been a decrease in the use of nPEP by GBM in the ACT with increased availability of PrEP.
Methods
Data were extracted retrospectively from the medical records of all GBM who were provided with nPEP at CSHC during the following 2-year time periods: - Period 1 (P1): 1 September 2015 – 31 August 2017 - Period 2 (P2): 1 April 2018 – 31 March 2020
In the first time period, PrEP was only available in the ACT on private prescription for self-importation. In the second time period, PrEP was initially available via two ACT study sites of EPIC-NSW, which commenced enrolment in September 2017. EPIC-NSW involved the rapid rollout of PrEP to GBM who were at high risk of HIV 4 with CSHC participants receiving up to 15 months’ supply of study PrEP. PrEP then became available on PBS prescription from 1 April 2018 or by continued participation in the EPIC-NSW study.
CSHC’s clinical record database was searched for patients who were provided with nPEP. Data were collected directly from clinical records using a purpose specific case report form and entered into an Excel spreadsheet. All participants were deidentified and given a unique study number. Data collection included demographic information including sex, age, country of birth, Medicare eligibility and sexual preference. Information regarding nPEP included prior use, the type of service where nPEP was commenced, and whether study participants self-initiated nPEP from a personal supply of medication. Details of PrEP use collected included prior, current and anticipated future use. Data were also collected on new HIV diagnosis in this patient group.
Data analyses were done using SPSS Statistics Version 25 (IBM; Armonk, NY). Comparisons between P1 and P2 were performed using a two-population test of proportions with one-tailed testing and significance set at p < .05.
Ethics
Ethics approval was obtained from the ACT Health Human Research Ethics Committee, Canberra. ACT HREC Reference Number: 2020.LRE.00002.
Results
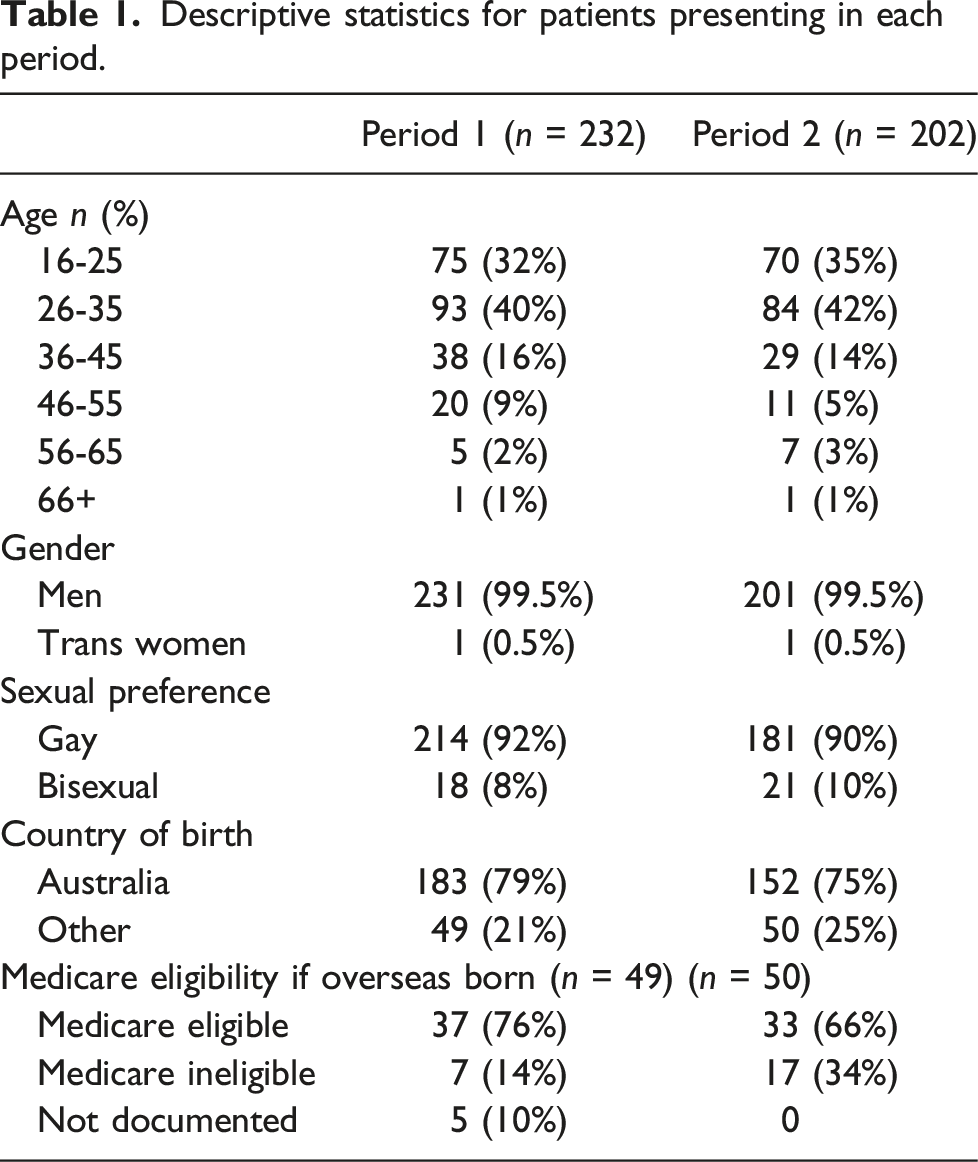
Descriptive statistics for patients presenting in each period.
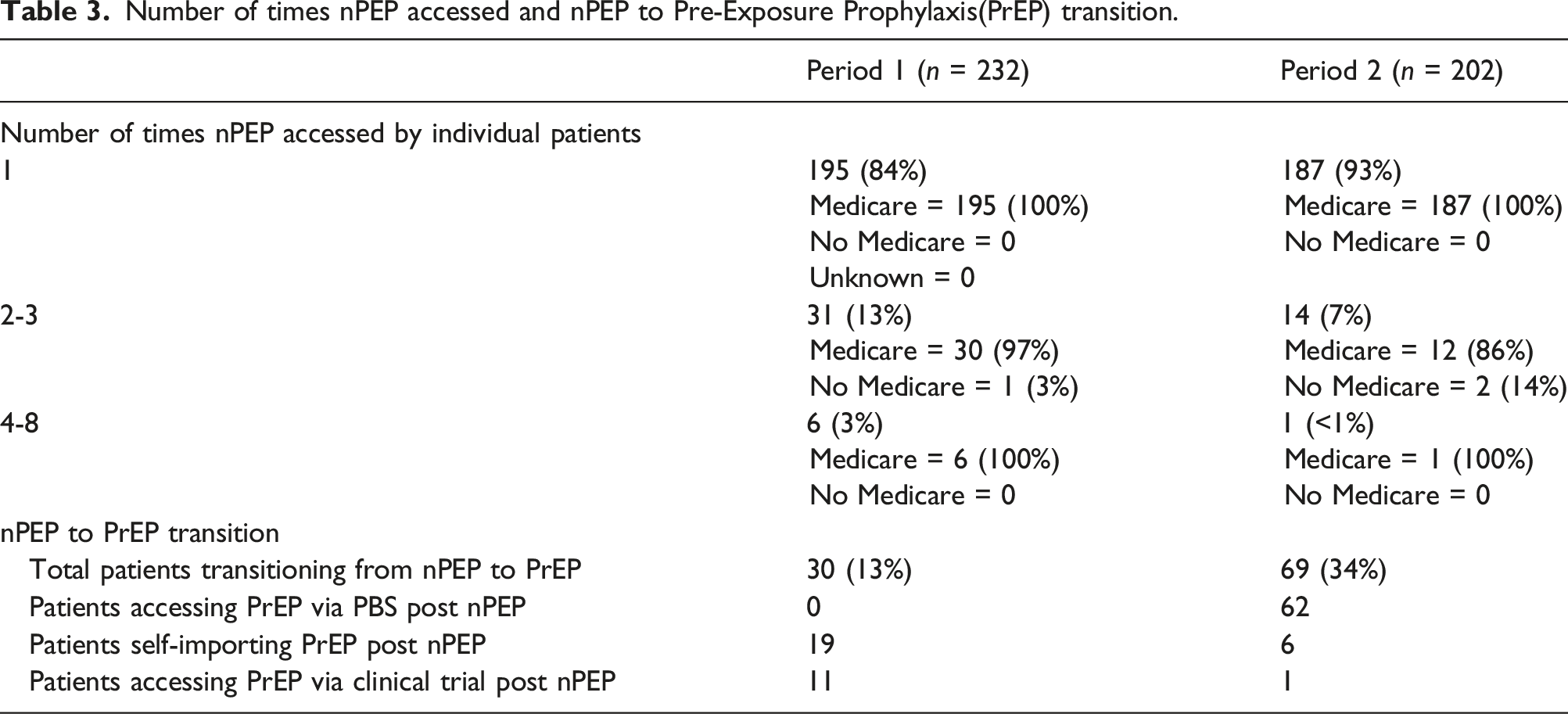
A two-population test of proportions demonstrated that GBM use of nPEP decreased significantly from 6.3% (n=302) of total GBM visits in P1 to 3.1% (n = 221) in P2 when PrEP was more widely available (Z=8.53, p < .001). Conversely, transition to PrEP after nPEP increased from 12.9% (n = 30) of patients in P1 to 34.2% (n = 69) of patients in P2 (Z=5.26, p < .001). In P1, the 30 patients commencing PrEP after nPEP included 19 self-importing PrEP and 11 accessing PrEP through clinical trial. In P2, the 69 patients commencing PrEP after nPEP included 62 accessing PrEP via PBS prescriptions, six by self-importation (four of whom were international students or visitors without Medicare therefore not PBS-eligible) and one continuing to access PrEP via a trial.
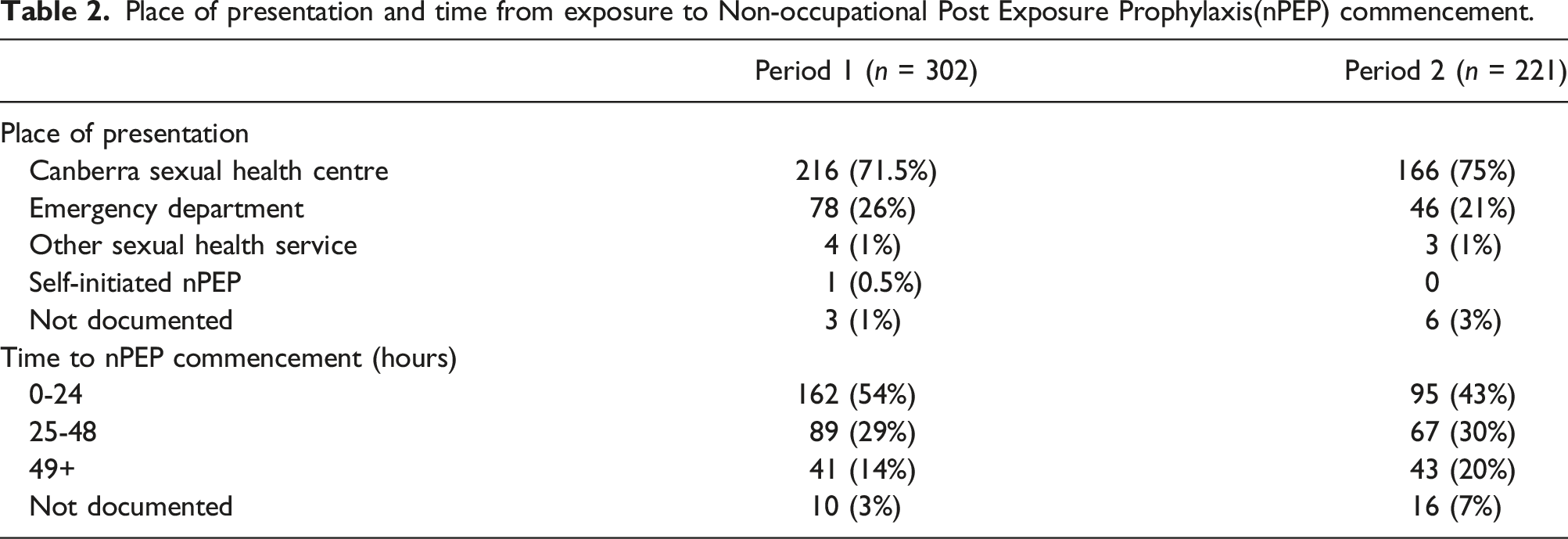
Place of presentation and time from exposure to Non-occupational Post Exposure Prophylaxis(nPEP) commencement.
The proportion of patients who presented for repeat nPEP presentations decreased from 16% (n = 37) in P1 to 7% (n = 15) in P2 (Z=2.73, p= .003).
Discussion
The primary aim of this study was to assess if the introduction of access to prevention with PrEP would affect the use of nPEP by GBM at risk of sexual or blood borne exposure to HIV. The number of GBM provided with nPEP decreased from 302 to 221 across the two time periods, with a reduction seen at both the sexual health centre and hospital emergency departments, the two main sites for accessing nPEP in the ACT at the time of this study.
There was a statistically significant decrease in nPEP provision as a proportion of clinic visits by GBM as PrEP became more widely available. Whilst this occurred in the context of a substantial increase in total number of presentations by GBM to the sexual health centre (P1: 4779, P2: 7205 visits) affecting denominator proportion calculations, the increase may be explained by more regular attendance for medication and ongoing care with PrEP access via EPIC-NSW study participation or by PBS prescription. There were no service delivery or policy changes at CSHC affecting access to nPEP, suggesting there was a reduction in the need for nPEP by GBM.
Similarly, there were no health service policy changes on the provision of nPEP at either of the two ACT hospital emergency departments. The proportion of nPEP initiation in ED compared to CSHC did not change substantially [P1 78/302 = 26%, P2 46/221 = 21%] for the two time periods. However, demonstration of an absolute reduction in nPEP initiation in the emergency departments (78 to 46 visits) supports the finding that nPEP use declined after PrEP became more available.
Our study identified a decrease in the proportion of GBM commencing nPEP less than 24 hours after HIV exposure across the two study periods [P1 162/302 = 54%, P2 95/221 = 43%]. There was an increase in P2 of GBM presenting after 49 hours. Whilst this change may not be statistically significant, it is a concerning change as earliest commencement of antiviral medication is likely to be more effective. 17 Time to presentation for nPEP is influenced by many individual factors including awareness of nPEP services and service access factors. It is unlikely that the delay in nPEP commencement is related to the higher number of GBM attending services in P2 as our clinic model was consistent throughout both P1 and P2 with no evidence that waiting times increased in P2 despite higher attendance. It is unclear if our patient cohort varied between periods. It is beyond the scope of this study to further explore this finding which may warrant further research investigation.
At CSHC, nPEP and related care is free to patients with and without Medicare access. Medicare is Australia’s universal healthcare system for Australian citizens, residents, and some overseas visitors. In our study, individuals presenting for nPEP were born in both Australia and overseas. In P1, 12/232 (0.5%) of patients were born overseas. Seven of these 12 individuals were not eligible to access Medicare, and eligibility was not recorded for 5. This compares to 17/202 (0.8%) born overseas with no Medicare in P2. Of these, 1/12 individuals (0.8%) accessed nPEP more than once in P1, versus 2/17 (0.11%) in P2. The proportion of overseas born patients presenting for nPEP was similar between the two time periods and due to incomplete information on Medicare eligibility it is not possible to assess if this changed.
Number of times nPEP accessed and nPEP to Pre-Exposure Prophylaxis(PrEP) transition.
Only one individual self-initiated nPEP, suggesting that this situation is rare in the ACT. This sub-group of GBM is at risk of HIV and are probably least likely to present to a health service. Two Canadian studies designed to allow self-initiation of nPEP have demonstrated that having access to a prescription for HIV antiretrovirals at home, and appropriate education on when to use it, may be a useful mode of HIV prevention.18,19 Although small study populations, the authors showed that self-initiated nPEP may eliminate some of the barriers associated with nPEP use including access within a 72-hour timeframe, and attendance at emergency departments and sexual health clinics, whilst enabling patients to be proactive about HIV prevention.18,19 Further research needs to be undertaken to determine the role of self-initiated nPEP as a HIV prevention method.
During P1, patients were more than twice as likely to present more than once to access nPEP compared to during P2 when PrEP was available through PBS. This is unsurprising as patients presenting for nPEP even once would be encouraged to consider transitioning to PrEP and no longer rely on repeated nPEP use.
Whilst there is limited published research exploring relationships between nPEP and PrEP use, GBM presenting at a health service requesting nPEP are very likely to meet the guideline recommendations for PrEP. Assessment of ongoing risk of HIV exposure and consideration of transfer to PrEP on completion of a course of nPEP should be part of the overall management of nPEP and be included in clinical policies and procedures. 20 Consideration of transition to PrEP is recommended in the current Australian PEP guidelines. 5
Published research that pre-dates the introduction of PrEP has demonstrated a lack of awareness of nPEP in GBM at risk of HIV 21,22 and it has been suggested that HIV PrEP delivery and usage will increase awareness of nPEP by discussion of a range of HIV prevention strategies. 23 In sequential Gay Community Periodic Surveys of GBM in Canberra, awareness of nPEP has increased from 72.6% in 2011 to 87.9% in 2019, and in 2019 92% of respondents were aware of PrEP. 24 It is unlikely that PrEP will be universally used for all situations with a risk of HIV exposure, and nPEP will remain an important HIV prevention strategy. 20 The broader question is not “nPEP or PrEP” but how to promote all effective HIV prevention strategies to those at risk as individual needs may vary over time.
There are limitations to this study which looks only at GBM who attend a single sexual health service for nPEP initiation or continuation. A small number of HIV-prescriber general practitioners could provide nPEP on prescription during P1, and this is not captured. In P2, it is unknown whether PrEP for nPEP was provided in general practice after PrEP was available via PBS prescription. As discussed above, self-initiation and completion of nPEP without contact with a health service could occur and is not reflected in this study population.
Conclusion
nPEP remains an important HIV prevention strategy. Increased access to PrEP reduced commencement of nPEP in GBM attending a publicly funded sexual health clinic in the ACT. Whilst discussion of nPEP to PrEP transition is part of nPEP care, the relatively low rate of transition from nPEP to PrEP, despite widespread availability, suggests the need to remain attuned to patient perceptions of and barriers to PrEP use and for continued attention to other HIV prevention strategies, including promoting awareness of nPEP in those at risk of HIV and not choosing to use PrEP.
Footnotes
Authors' contributions
SW, AB and SM contributed to the study conception and design. Data collection and analysis were performed by SW, AB and WD. The first draft of the manuscript was written by SW, AB, WD and AT with revisions by SM. All authors read and approved the final manuscript.
Ethical approval
Ethical Approval was obtained from the ACT Health Human Research Ethics Committee, Canberra. ACT HREC Reference Number: 2020.LRE.00002.
Data availability
All data and materials support our published claims and comply with field standards.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.