
Abstract
Background
Herpes simplex virus-1 (HSV-1) is a member of the alphaherpesvirus (alphaherpesvirinae) subfamily, allowing it to affect a wide range of hosts. Herpes simplex virus-1 affects 3.7 billion people, or 67% of the population, under the age of 50. With a vast number of people infected by the virus, everyday objects are often contaminated with this agent. In this study we determined how long HSV-1 can remain viable on contaminated fomites.
Methods
Fomites were selected for their use near potentially contaminated orifices and variable frequency of sanitization. Toothbrushes and surrogate phallic devices (SPDs) were cut, sterilized, and contaminated. After contaminating the fomites, we collected samples over a 24 h period, then used plaque assays to determine viral titers at prescribed time points.
Results
The quantity of replication-competent virus present appears to decrease significantly 2 h post-contamination, then steadily declines over time, nearing zero at 24 h.
Conclusions
Our findings suggest that different surfaces influence HSV-1 survival. Proper cleaning must be performed for these types of fomites, especially if shared in an environment where someone with active genital or oral herpes lesions uses one of these fomites shortly after someone else.
Introduction
Herpes simplex viruses 1 and 2 (HSV 1 and 2) are alphaherpesviruses that have a short replicative cycle, induce cytopathology in cell cultures, and have a broad host range. 1 While frequently associated with oral lesions termed “cold sores,” HSV-1 infection can be exhibited as orolabial herpes, herpes gladiatorum, HSV folliculitis, herpetic whitlow, ocular herpes, genital herpes, or herpes encephalitis. 1
Common transmission of HSV-1 and -2 occurs through direct contact between a host and a recipient. 2 Individuals who are infected but show no signs or symptoms still sometimes shed virus asymptomatically. 1 Hence, many of the 60–95% of HSV-1 and/or HSV-2-positive patients worldwide have a chance to transmit the virus;1–3 regardless the titer; symptomatic shedding may reach 105–106 plaque-forming units (PFU), 4 while asymptomatic shedding may contain as low as 100 PFU. 5 Although transmission from patient-to-patient is often cited, 2 indirect transmission through contact between an active lesion and inanimate objects (i.e. fomites) is seldom considered.
We explored survival of HSV-1 on two common fomites, toothbrushes and surrogate phallic devices (SPDs). Although toothbrushes are rarely considered a potential source of transmission, they may harbor HSV-1 that may be shed during regular use. The moist environment of a used toothbrush can sustain Staphylococci, coliforms, pseudomonads, and yeasts,6,7 all organisms subject to dehydration, suggesting that even viruses sensitive to dehydration may persist. Silicone-based SPDs, another possible source for indirect genital or oral transmission, may be contaminated with HSV because of their use near potentially contaminated orifices. We hypothesized that through verifying viral titers post-contamination, we could determine viral persistence on different fomites over 24 h and distinguish at what point clinical transmission of HSV-1 by fomites is a less relevant clinical issue.
Of note, survival of HSV-1 on fomites has been studied previously. However, the methods executed lacked safety and/or rigor.8–12 Therefore, our research was designed to address these shortcomings and to approach the question of HSV survival on other fomites that may be ready sources of HSV transmission.
Materials and methods
Cells and viruses
Vero cells [ATTC CCL-81] were cultured in alpha-MEM (α-modification of minimal essential media [Corning CellGro, Corning, NY]) with 10% FBS (Thermo Fisher Scientific), 1% antibiotic/antimycotic (Gibco-Thermo Fisher Scientific), and 1% Glutamax (Gibco-Thermo Fisher Scientific) according to standard protocols. 13 Herpes simplex virus-1 (KOS) (ATCC #VR-1493) was cultured and titered according to published methods.13,14
Preparation of fomites
Toothbrushes (Standard Classic Medium Soft Individually Wrapped; Amazon, Seattle, WA) were removed from packaging and cut into 12–15.6 mm segments of both plastic and bristles to fit into each well of a 24-well plate (Corning) with no other treatment. These pieces were then sterilized with isopropyl alcohol as previously described. 13 The toothbrush fragments were left to dry under a UV light overnight at 25°C in a biosafety cabinet, then stored covered for later use. A silicone SPD (Large Bulge Waterproof Packer, 6.5-inch; Spencer’s Gifts, Towson, MD) was removed from packaging and cut into 12–15.6 mm cubes, each of which fit into one well of a 24-well plate in a similar fashion. These fragments were then sterilized, rinsed, dried, and stored following the same steps as described above for the toothbrush pieces.
Contamination of fomites
A group of cryovials (40) were prepared with 1 mL each of VSM (Virus Storage Medium (alpha-MEM containing 10% glycerol); 15 glycerol was chosen as a cryopreservative because freezing (at −80°C) and thawing of enveloped virus specimens can occur without loss of titer. 15 Freezing allowed us to collect samples over the period of 1 day but run plaque assays separately and non-consecutively. Herpes simplex virus-1 (10 μL, 6.04 × 105 PFU per sample) was added to 36 of the 40 fomites (one set of four was contaminated with 10 μL PBS as a control), and the control and first set of four HSV-1-contaminated samples were swabbed immediately with a sterile Dacron swab (Thermo Fisher Scientific; these first samples were designated as 0 h (H0) post-contamination. Swabbing consisted of thorough, circular motions across the surface of each fomite at least 5 times per sample. Each swab was immersed immediately into one of the cryovials, shaken in the VSM, and squeezed against the side of the vial to release any viruses into the VSM, then frozen at −80°C. The remaining fomites were swabbed and processed similarly in sets of four at hours 1, 2, 4, 6, 8, 10, 12, and 24 post-contamination. Plaque assays consisted of each sample being serially 10-fold diluted and added to Vero cells; 14 cells were incubated, stained, and plaques were counted according to protocol. 14 Final titers from each sample in each cryovial were determined if they fell within a statistically significant threshold (10–100 plaques). 14
Results
Herpes simplex virus-1 survival on toothbrushes
Nylon toothbrushes were contaminated and sampled as in Materials and Methods. The average viral titer of HSV-1 at H0 (Hour 0) was 4.7 ± 0.24 × 105 PFU (Figure 1(a); Table 1), the maximum/baseline viral titer on toothbrushes (Table 1) and approximately 78% of the original input. At H1 there was 90.7% (Figure 1(b)) of viable remaining virus from H0 (4.3 ± 0.44 × 105 PFU; Figure 1(a); Table 1), demonstrating a slight decrease that was not statistically significant (Figure 1(a) and (b); Table 1). However, there was a considerable titer reduction at H2 with 4.4% replication-competent virus remaining from H0 (2.08 ± 0.081 × 104 PFU; Figure 1(a) and (b); Table 1). For H4-H8 the remaining replication-competent virus from H0 fell steadily to 0.59% (2.8 ± 0.83 × 103 PFU) (Figure 1(a) to (c); Table 1). Viable HSV-1 titer continued to gradually decline from H10-H12, and by H12 there was only 0.024% of replication-competent virus remaining (1.2 ± 0.14 × 102 PFU) (Figure 1(a) to (c); Table 1). By H24 the viral titer was nearly undetectable, with only 3.5 ± 0.18 × 100 PFU remaining of replication-competent virus (Figure 1(a) to (c); Table 1). (a) Survival of HSV-1 on contaminated toothbrushes. Cut toothbrushes were contaminated with 10 μL (6.04 × 105 PFU) of HSV-1 and swabbed at incremented hours. Each sample was subjected to plaque assays to determine the level of surviving HSV-1 at each time point.
14
Student t-tests were conducted to determine the significance of differences in titer between time points (Table 1). (b) Percent of remaining replication-competent virus over time. Data from (a) are represented as percent replication-competent virus remaining over time. Note the significant drop in viral titer (96%) by the second hour. (c) Inset of remaining replication-competent virus. Inset shows data from (b) from H4 post-contamination through the end of the sampling period. t-test for toothbrushes.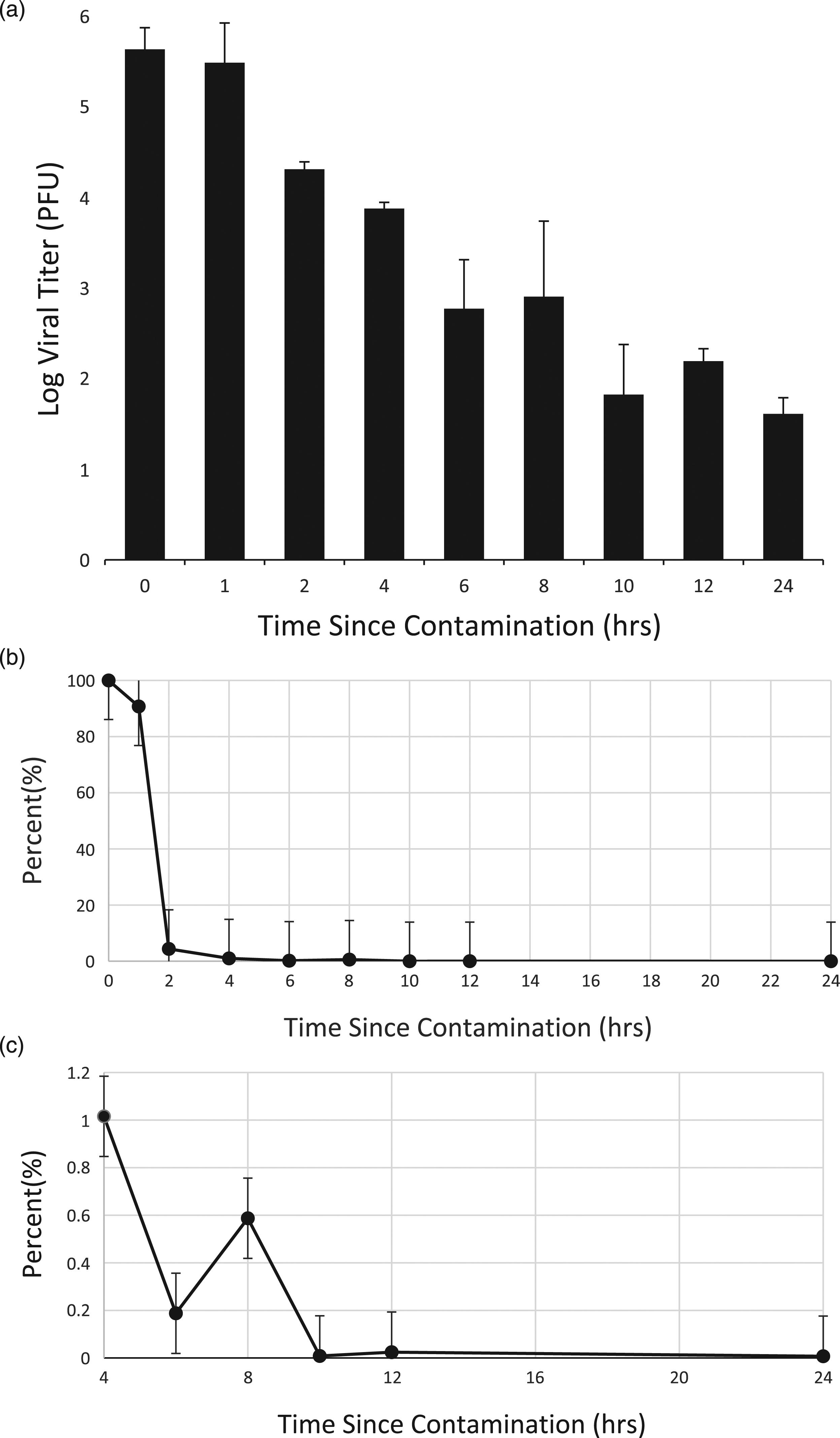

Herpes simplex virus-1 survival on SPDs
Small pieces of silicone from an SPD were contaminated and sampled as above for toothbrush pieces. The average viral titer for swabbed SPDs of HSV-1 at H0 was 1.06 ± 0.17 × 106 PFU (Figure 2(a), Table 2), the baseline/maximum titer for these experiments and about twice as much as the initial titer obtained from toothbrushes (Figure 1(a), Table 1). For H1 there appeared to be 130% of replication-competent virus from H0, but a pairwise t-test comparing H0 to H1 titers showed that there was no statistically significant difference between these measurements (Figure 2(a) and (b); Table 2). The titers between timepoints H1 to H2, however, were significantly different (Table 2; p < .05), showing a decrease in replication-competent HSV-1. For H2 there was 14% of remaining virus from H0 (1.5 ± 0.14 × 105 PFU; Figure 2(a) and (b); Table 2), and that titer continued to decline through H6 (Figure 2(a) and (b); Table 2). By H8 there was only 0.0016% of replication-competent virus from H0 remaining, a statistically significant drop from H0 (Figure 2(a) and (b); Table 2). Similarly, the titers from H6 to H8 are also significantly different (p = 1.5 × 10−4; Table 2). Viral detection ended at H8, when no viral plaques could be obtained for samples taken between H10 and H24 (Figures 2(a) and (b)). A. Survival of HSV-1 on contaminated SPDs. SPDs were contaminated with 10 μL (6.04 × 105 PFU) of HSV-1, swabbed, and subjected to plaque assays at incremented hours as in Figure 1. Student t-tests were conducted to determine the significance of differences in titer between time points (Table 2). (b) Percent of remaining replication-competent virus over time. From H0 to H2, there is a significant drop in viral titer of 86%, observed in both (a) and (b). Note that there was no detectable viable virus subsequent to 8 hours post-contamination. t-test for simulated phallic devices.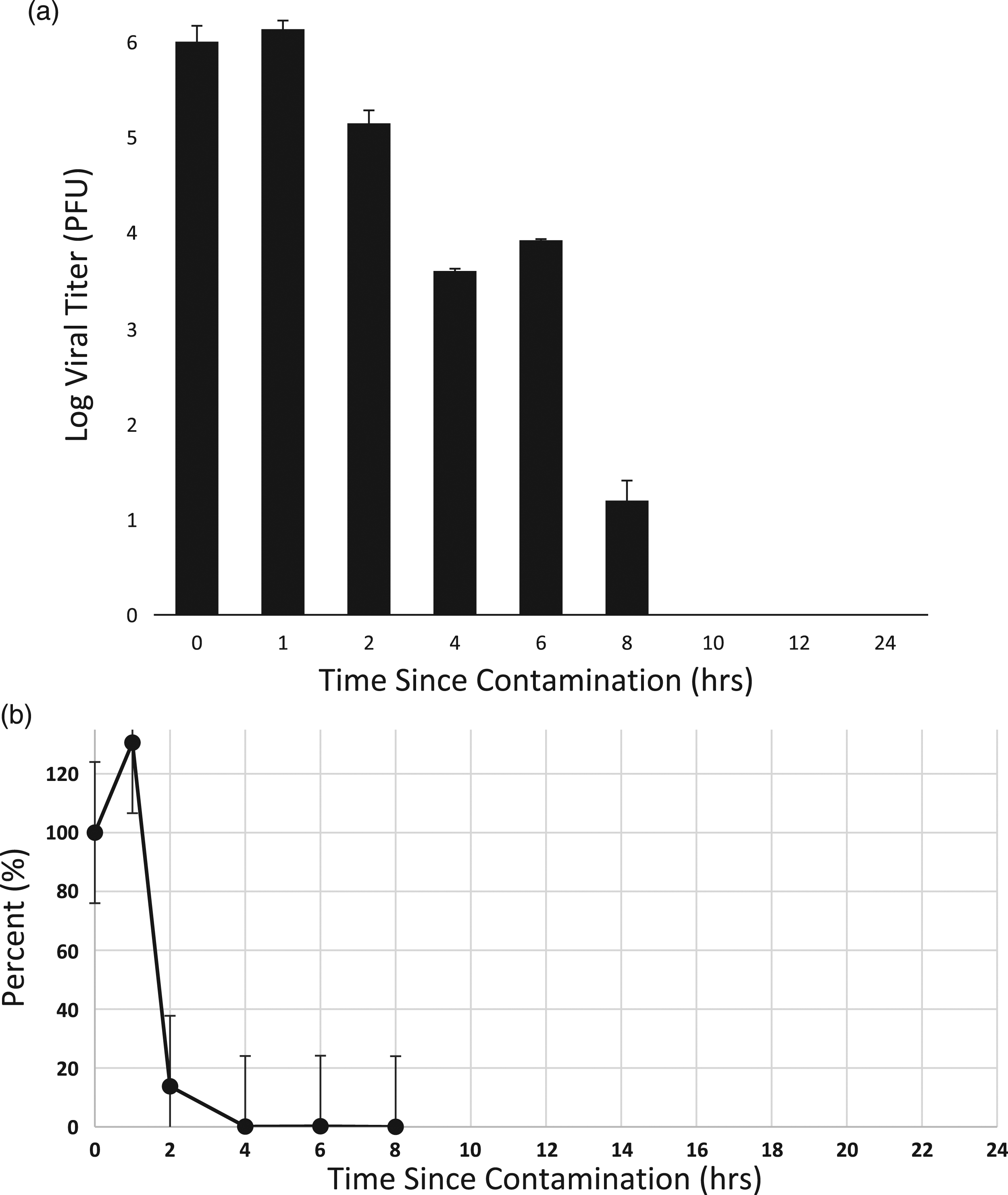

Discussion
We chose to contaminate samples with 6.04 × 105 PFU, which represents the titer to account for a 50% transmission rate for a highly infectious HSV. 2 We thought that the nylon bristles of the toothbrush might provide an environment for survival of HSV-1 over the course of 24 h. The increased surface area of the bristles potentially provided more protection for HSV-1, locking in moisture to preserve the virus. However, we found that replication-competent HSV-1 decreased to only 4.3% of the original replication-competent virus titer by 2 h post-contamination, decreasing progressively after that until little viable HSV-1 was recoverable after 24 h (Figure 1). This decrease in viable HSV-1 decreases the likelihood for transmission, although not necessarily completely eliminating it. Since the ADA-recommended frequency for brushing teeth is twice a day (approximately an 8 h overnight gap and 12–14 h daytime gap), 16 a contaminated toothbrush could potentially be harboring between 0.59 and 0.024% replication-competent HSV-1 after it has been used (Figure 1(c)). These data also emphasize the necessity to maintain proper care of oral hygiene equipment, 16 especially for users exhibiting active oral herpetic lesions.
Frequent use and improper care may also be relevant for silicone-based SPDs. As with the toothbrushes, there was considerable replication-competent virus remaining through H2 (Figures 1(b) and 2(b)). However, the remaining viable virus titer declined significantly at H4 and thereafter, while the toothbrushes still had measurable virus up to H24 (Figures 1(a) and 2(a)). This may have been caused by the smaller wettable surface area of the SPD in contrast to the toothbrush fragment; perhaps the virions dried out more quickly on the SPD than on the toothbrush.
Enveloped viruses like HSV tend to lose viability rapidly due to dehydration, while naked viruses, such as rotaviruses, do not. 17 This impacts the overall survivability of viruses on different fomites, especially given other factors such as chemical makeup of the materials and different environments. The chemical treatments of materials cannot be ignored, since the nylon of the toothbrush bristles are often treated with harmful chemicals such as Triclosan to prevent bacterial growth. 18 While both nylon and Triclosan are considered nontoxic, the different chemical manufacturing processes may also have an impact on HSV survivability.
Our findings suggest that the surface of the SPDs was a less favorable environment for HSV-1 survival compared to that of nylon bristles. As with toothbrushes, proper post-use care for these types of fomites is highly encouraged; our data suggest that one must wait at least 2 h after contamination for any appreciable decrease in virus titer and, hence, the chance for transmission (Figures 1(b) and 2(b)).
Herpes simplex virus-1 survival can be affected not only by time, but also by its environment. For example, further experiments to determine whether humidity, which may provide extra environmental moisture to enhance virus survival, could be conducted. We also foresee expanding investigations to other fomites such as cigarettes, glassware, plastics, and washcloths, commonly shared fomites composed of different materials. And while one may assume similar inactivation profiles for other herpesviruses, e.g. Epstein-Barr virus, experiments with those viruses should also be conducted for reliability.
The recent COVID-19 pandemic proved that it is crucial to understand the timeline in which a virus can survive on possible fomites, a medium for indirect transmission. We also note the importance of cleaning potentially HSV-contaminated fomites because acquiring a genital HSV infection may make HIV infection more likely; it is estimated that 29.6% of new HIV infections were attributed to an initial HSV infection,1,19 and HSV-1 infections in immunocompromised individuals may also be deadly.1,19 Highlighting the time course of HSV inactivation sheds further light on preventative measures against spreading viral infection.
Footnotes
Acknowledgements
We wish to acknowledge Imani Pearson, Ryan A. Williamson, and Haley Zack for their assistance in the early stages of this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We thank Project Accept and the Towson University Foundation. BJM was the recipient of a Towson University Faculty Development Award. This work was also supported by Towson University Undergraduate awards to CS, RU, RJM, IP, and DM. A Bridges to the Baccalaureate grant from The National Institutes of Health, R25 GM058264, helped support the work of RAW and MDD.