
Abstract
Background
Men having sex with men (MSM) are at increased risk of acquiring sexually transmitted infections (STIs), including extra-urethral infections. This study aimed to provide information on the presence of genital and extra-genital non-viral STIs and associated risk factors among MSM in the Tshwane district of South Africa.
Method
Samples were collected from 200 MSM in the North-western area of Tshwane. After the completion of a questionnaire including demographics and sexual history and an HIV test, three swabs (pharyngeal, rectal, and urethral) were collected and tested for the presence of Neisseria gonorrhoeae (NG), Chlamydia trachomatis (CT), Mycoplasma genitalium (MG) and Trichomonas vaginalis (TV).
Results
Data were collected from 199 participants and 77/199 (38.7%) participants had at least one infection regardless of specimen site. Of these 34 (17.1%) were infected with NG; 36 (18.1%) with CT, 16 (8.1%) with MG and 14 (7.0%) with TV. NG and CT were most frequently detected in rectal specimens. The HIV prevalence in this study was 66.8% (133/199), with 56 (28.1%) of participants both STI and HIV positive
Conclusions
This study has highlighted the high burden of STIs in MSM in the local community, especially the prevalence of these pathogens in extra-genital sites.
Background
Men who have sex with men (MSM) are a vulnerable at risk population, prone to acquiring sexually transmitted infections (STIs) including HIV. 1 MSM engage in a variety of sexual practices, which vary on behaviours, partners, and condom use, all of which have to be considered when designing effective prevention programs. 2
Although an accurate MSM population estimate for South Africa does not exist, it has been reported that up to 3.1% of men had recent sex with a man, 3 and 5.4% of men ever had sex with a man. 4 National representative data of the prevalence of HIV in MSM are not available for South Africa, but it is estimated that this figure may be 34.6%. 5 A few studies in South Africa on STI prevalence in MSM regardless of presence of symptoms reported a prevalence of 10%–24% for Chlamydia trachomatis (CT) at any anatomic site and 3%–55% for Neisseria gonorrhoeae (NG) at any anatomic site,3,6–8 while rectal Trichomonas vaginalis (TV) infection in MSM has also been documented. 9
MSM are considered a core group in the spread of HIV and other STIs. 10 MSM have a higher risk of acquiring STIs because of the sexual behaviours that have been observed among this group, including a higher number of sexual partners, inconsistent use of condoms, receptive anal intercourse, transactional sex, the use of stimulants before and during sex, and infection with HIV.2,11–13
In Sub-Saharan Africa, management of STIs is generally syndromic. This strategy has associated challenges in MSM, among which are the many infections (particular rectal and oropharyngeal) that remain untreated because a large proportion is asymptomatic.6,7,13 In addition, despite constitutional protection in South Africa, MSM still experience stigma and discrimination when seeking health services.4,13 This limits access to sexual health services and leads to reluctance to disclose same-sex sexual behaviour, limiting appropriateness of care. 6
To address the burden of STIs among MSM in South Africa, it is important to not only understand the prevalence of these infections, but also to have insight in the underlying risk factors. This study aimed to provide information on the prevalence and associated risk factors of STIs in a MSM population in Tshwane, South Africa.
Methods
This study was undertaken from June 2016 to May 2017 at the Mecru Research Unit (MeCRU) in Ga-Rankuwa, a peri-urban suburb in the North-western side of Tshwane, South Africa and was approved by the Research Ethics Committee of the Sefako Makgatho Health Sciences University (SMU) (ref: SMUREC/P/196/2015: IR). Men who self-declared to have sex with other men, who were 18 years or older, resided in targeted areas, and who consented to participate in this study were included. A recruitment team comprising of a community liaison officer and 2 recruiters was formed, and recruitment was mainly through snowballing. Participants received an information leaflet upon arrival at the research unit, where after informed consent was obtained. Participants completed a self-administered questionnaire. Demographic data (age, place of residence, education), as well as current sex practice (received and/or performed oral sex, insertive and/or receptive anal intercourse, performed and/or received rimming, number of partners, condom, and substance use) were collected. Unsafe sex was defined as condomless anal sex and/or more sex partners. Current sex practice was defined as any of the described forms of sexual contact having occurred in the 6 months leading up to participant enrolment. For confidentiality, participants were assigned unique identifiers.
A rapid HIV test was performed, and three swabs (pharyngeal, rectal, and urethral) were collected by a clinician from each participant. These were tested for CT, NG, TV, and MG at SMU using the Seegene STI-7 real-time PCR kit (Seegene, Seoul, Korea) following the manufacturer’s instructions. Amplification was performed on the CFX Real-Time PCR Detection system (Bio-Rad, USA).
All the results and participants’ information extracted from the questionnaire were entered into a Microsoft® Excel® database. Laboratory results were also recorded. Descriptive statistics were used to summarize demographic data. Bivariate and multivariate logistic regression analyses were used to assess independent predictors of a STI and any cross-sectional association between risk factors and presence of STI. Bivariate analyses included two-sample tests for differences in proportions, χ2 tests of independence, and logistic regression assessing the associations between risk factors and presence of STI. Backward elimination with a relaxed p-value set to 0.20 (based on the Wald test from logistic regression) 14 was used to determine which variables were included in the multivariate model. In addition, basic demographic characteristics, including age and education, were also entered into the model. Variables that were significantly (p < .05) associated with the presence of an STI were reported, accompanied by respective odds ratios (OR) and 95% confidence intervals.
Results
Summary of demographics, sexual behaviour, and history with an STI infection.
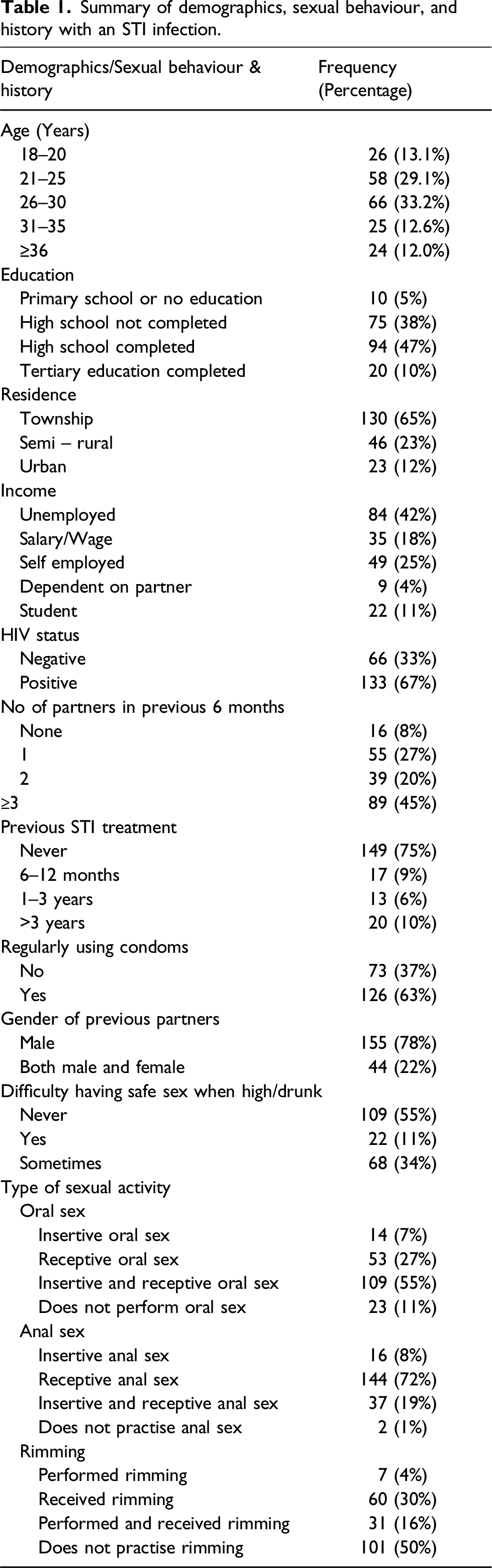
Of the participants screened, 77/199 (38.7%) had at least one infection regardless of specimen site. Of these, 34 (17.1%) were infected with NG; 36 (18.1%) with CT, 16 (8.1%) with MG and 14 (7.0%) with TV. No STI was detected in 61.3% of the participants. Co-infections with two or more pathogens, were seen in 23 (11.6%) of the participants. Of these, NG + CT was most often seen together (13/23). NG (20/48 positive NG tests [42%]) and CT (31/43 [72%]) were most frequently detected in rectal specimens, while TV (10/15 [71%]) was most often seen in oral specimens and MG was seen equally in rectal and urethral specimens (8/16 [50%]) (Figure 1). Infections in more than one anatomical site by the same pathogen was seen in 19 (9.5%) of the participants with pathogens detected in all three anatomical sites in 3 participants. Of the 14 participants where NG was detected in more than 1 site, half (7) were detected in both the oral and urethral sites, followed by 3 in the rectal/urethral sites and 2 in the rectal/oral sites. In two participants, the pathogen was detected in all 3 sites. CT were detected in more than 1 site in 4 participants, with 2 in the rectal/urethral sites, 1 in the rectal/oral site and 1 in all 3 sites. TV was found in both the rectal and oral sites in one participant while MG was not found in more than one site of a participant. Presence of sexually transmitted infections (%) in 199 MSM participants by anatomic site.
The HIV prevalence in this study was 66.8% (133/199), with 56 (28.1%) of participants both STI and HIV positive. HIV was not significantly associated with infection (p = 0.16; OR 1.56 CI 0.84–2.90). However, amongst the different age groups, HIV was significantly associated with infection in the age group 21–25 years (p = 0.03).
Logistic regression analysis of factors associated with non-viral sexually transmitted infections.
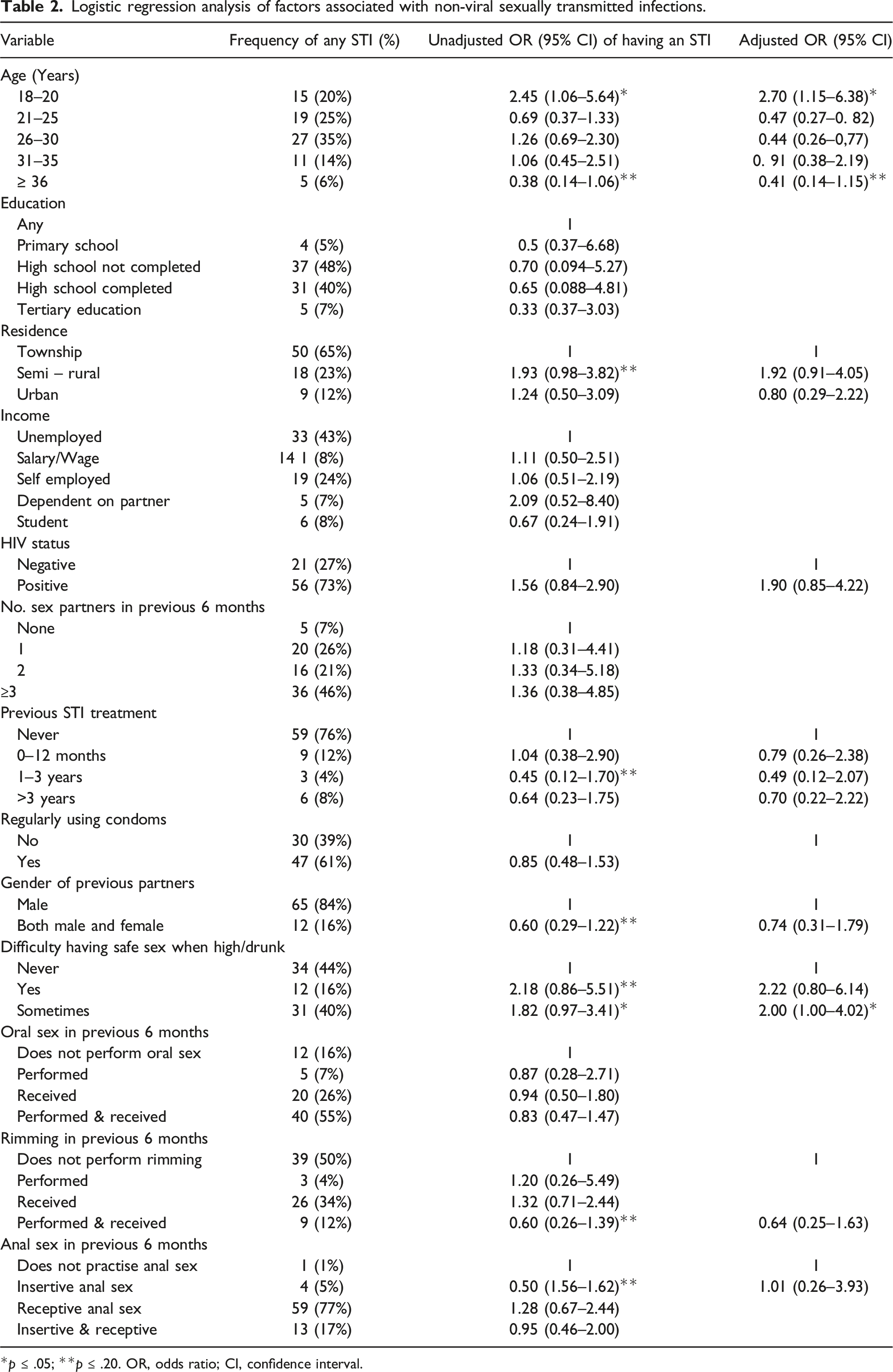
*p ≤ .05; **p ≤ .20. OR, odds ratio; CI, confidence interval.
Discussion
This study investigated the prevalence of 4 sexually transmitted pathogens in MSM in Tshwane, South Africa, as well as associations of infection with anatomical sites and several other factors that usually play a role in infection.
The median age of the men in this study was 26 years which is younger than the participants in two other South African studies (in Cape Town and Soweto), suggesting the probability that younger individuals more frequently openly identify themselves as MSM.6,15 This study further showed that the odds of contracting a bacterial STI increased in younger MSM, with participants between 18 and 20 years significantly more likely to be infected. This was also seen in a large national US sample of young MSM where the prevalence of STIs, and especially rectal STIs, was high. 16 More than half of the participants completed high school or had tertiary education which was lower than the 73% of participants that completed high school in the Cape Town study, and the 91% in a study in Johannesburg.6,17
Studies over the years have shown that there is a growing increase of HIV in MSM and as they have an increased risk for STIs compared to heterosexual men, they are severely affected by this pandemic.18,19 The HIV prevalence in this study was 66.8% which is higher than the 52.3% of MSM participants in a study in Cape Town, 20 37.5% among MSM/Trans gender (TG) participants in Johannesburg, 17 and only 10% among MSM/TG in Kigali, Rwanda. 21 However, a study done in Brazil on MSM reported an HIV prevalence of 72% which was almost similar to that seen in the current study. 22 Even though HIV was not significantly associated with an STI in this study, amongst the different age groups, HIV was significantly associated with infection in the younger participants (21–25 years). These findings prove the severity of the HIV burden on MSM in Africa, particularly in South Africa, and especially among the younger MSM.
In the multivariate analysis, being between 18 and 20 years of age and sometimes finding it difficult to perform safe sex (using a condom, restrict sexual partners) when high/drunk were the only factors that were significantly associated with a bacterial STI infection. Chemsex (i.e. drug use during sex) has been shown to be highly associated with sexual risk-taking behaviour (more sex partners and more often condomless anal sex) and a high prevalence of STIs. 23 The reported number of sexual partners over the 6 months preceding this study was not associated with any of the parameters examined in this study population, although almost half of the men reported to have had three or more sexual partners in the preceding 6 months, increasing the odds of having an STI. Most of the men reported regularly using condoms during sex in the preceding 6 months and had never received treatment for an STI. The odds for an STI infection increased when they were dependent on a partner, received treatment for an STI in the preceding 6 months, performed and received rimming or received anal sex. Many studies on MSM have reported receptive extra genital sexual intercourse being higher in MSM than in heterosexual men, 24 as was also seen in this study where the majority of MSM practiced receptive anal sex (72%). However, this was much higher than the results from the Soweto study where only 30.3% of MSM reported to ever have practiced receptive anal sex. 15 It has been found that MSM often underreport their behaviour, eg. receptive anal sex due to perceived judgement by clinicians or health care workers. 25 Participants in our study could have been more comfortable as it was a research environment different from a Health Care setting which could be judgemental. Results from our study highlighted the risk for STIs among local MSM, demonstrating the need for effective HIV and STI prevention interventions that are MSM-focused.
Unlike symptom-based screening, asymptomatic STI screening of the MSM community has resulted in higher STI detection. This is due to the biased nature of symptom-based screening as those MSM without any symptoms do not consult. 16 Just more than a third (38.7%) of the participants in the current study had at least one non-viral STI regardless of specimen site. This was higher than the 14.2% found at baseline among black MSM in the USA, 12 similar (30.1%) to a study among MSM in Germany, 11 but much lower than the 80% found among MSM in Johannesburg and Soweto. 3 The latter study was on both asymptomatic and symptomatic men, while in the current study, most of the men were asymptomatic. Co-infections with two or more pathogens, were seen in 22 (11.1%) of the participants which is similar to the 17% MSM co-infected with NG and CT in the Cape Town study. 6
The prevalence of sexually transmitted pathogens in this study was high even when considering infections from different sites in the same patient. NG was found in 17.1%, CT in 18.1%, MG in 8.1% and TV in 7.0% of participants. This differs from the prevalence reported in the study done on MSM in Germany where MG was the most frequently detected (17.0%) followed by CT (9.9%), NG (8.9%) and TV in only 0.1% of participants. 11 In South Africa, two studies that have reported on STIs among MSM that were recruited regardless of presence of symptoms found a prevalence of 3% and 16% for NG and 10% and 24% for CT at any anatomic site.6,7 Among symptomatic MSM in Johannesburg, TV and MG were seen in 3.8% and 1.3% of participants respectively. 26 The differences in these studies could be attributed to the different patient groups (asymptomatic/symptomatic), different settings that the studies were done in and the unavoidable selection bias influencing the general prevalence of these infections in the area that the study was done in.
NG, and CT were most frequently detected in rectal specimens, which is similar to most studies done on MSM worldwide and in South Africa.6,8,11,12,26–31 In addition, more than a quarter of the NG positives were found in the pharyngeal samples, which although higher than that seen in most studies, seems to be common amongst MSM.6,11,28,30,31 Oral sex has an important role in sustaining gonorrhoea in a population of MSM by providing a pool of untreated asymptomatic infections. Anorectal gonorrhoea can be acquired when saliva is used as a lubricant for anal sex and rimming (oropharyngeal route) and seems to best fit existing epidemiological and behavioural data.28,32 TV was most often seen in pharyngeal specimens (71%). However, it has been reported that the commercial PCR assay used in the current study (Anyplex™-II-STI-7 kit, Seegene, South Korea) had miss-identified Trichomonas tenax as TV in pharyngeal samples. 33 This could account for the high TV presence in the pharyngeal samples, and further investigation using another assay or nucleic acid sequencing should be done to verify this finding. Similar studies on MSM only reported on TV in rectal samples.9,27 MG was seen equally in rectal and urethral sites with no MG detected in oral samples. This is similar to results reported elsewhere.34,35
Infections in more than one anatomical site by the same pathogen was seen in 9.5% participants, with NG the most frequently seen in more than one site (74%). In the Cape Town study, 14.9% of participants were infected by the same pathogen in more than one site. 6 The high prevalence of rectal and pharyngeal STIs are concerning given that regular STI testing is not widely performed, especially for extragenital STIs. In our study 53 of the 77 participants (69%) with any extragenital STI would have been undiagnosed if only urethral samples were tested. This puts MSM at higher risk for having an unknown rectal/pharyngeal STI, drawing the attention to their high impact for an ongoing transmission of STIs, also taking in consideration that 22% of participants in this study reported to also have female partners. The WHO recommends having respective screening offers for MSM if the prevalence of asymptomatic pharyngeal and rectal infections exceeds 1–2%. 1 In resource-poor countries, like South Africa, that are unable to operationalize widespread direct screening for financial, logistic or other reasons, following the WHO guideline for empiric STI treatment for high risk MSM may still be the best approach currently. 1 For an effective public health response, it is important to ensure that MSM have access to HIV and STI prevention and treatment services.36,37 Services for MSM need to be both sensitive to diversity in gender and sexual orientation and should be competent in addressing MSM-specific sexual health needs. 38
Conclusion
Given the high overall prevalence of sexually transmitted pathogens in our study and the high proportions of extragenital and asymptomatic infections, the results strongly support broadly implemented STI-screening offers for MSM with special emphasis of screening at all three localizations, urethra, rectum, and oropharynx. However, the correct balance between cost effective empiric treatment of symptomatic STIs and screening for asymptomatic STIs in this population at increased risk of infection should be found.
Footnotes
Acknowledgements
We wish to thank Prof J-P Bogers from the University of Antwerp, Belgium for his guidance. We acknowledge the MeCRU team under leadership of Ms N Moeketsi for support and assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work received funding from the Flemish government (IUC-VLIR-OUS).