
Abstract
The Centers for Disease Control and Prevention (CDC) published a health advisory on the occurrence of severe cases of mpox in immunocompromised patients, namely those with advanced HIV. Treatment options are limited, and very little is known about how to optimally treat patients with severe disease. Herein we describe two cases of severe mpox in Chicago in the setting of advanced HIV and provide suggested guidance for managing cases of severe disease in immunocompromised patients based available data, CDC recommendations, and our experience managing these patients.
Summary
In light of recent cases of severe mpox virus being reported by the CDC, it is pertinent for clinicians to be aware of available therapeutic options. Specific guidance on how to optimally treat severe mpox in patients with advanced HIV is lacking. Based on review of available data, CDC and WHO recommendations, and our experiences managing severe mpox in patients with advanced HIV – we provide our expert opinion on optimal therapeutic approach.
Background
The World Health Organization (WHO) declared the mpox outbreak a global public health emergency in July 2022. As of 19 December 2022, there have been over 82,000 cases of MPV worldwide and over 29,000 in the United States (U.S.). 1 While the number of new cases overall have begun to decline, there are increasing reports of immunocompromised patients (specifically in those with advanced HIV) presenting with severe mpox or relapsing disease following an initial response to anti-viral therapy. 2
According to a recent CDC Health Advisory in September 2022, severe manifestations of disease have been observed in primarily patients living with HIV with CD4 counts <200 cells/ml. 3 The observed manifestations in these severe cases include: atypical or persistent rash with coalescing necrotic lesions, lesions on a significant proportion of the total body surface area, lesions in sensitive areas including mucosal surfaces, exudative bowel lesions, severe lymphadenopathy, lesions leading to stricture and scar formation, involvement of multiple organ systems (e.g. pulmonary, oropharyngeal, neurologic, cardiac, ocular, urologic).
While the CDC advisory notes that the majority of patients are those with advanced HIV, they outline the need to consider patients with moderate to severe immunocompromising conditions as high risk for severe disease. The CDC lists the following as such conditions: advanced or poorly controlled HIV (CD4 <200 cells/ml 3 ), solid organ transplant recipient, leukemia, lymphoma, therapy with alkylating agents, antimetabolites, radiation, tumor necrosis factor inhibitors, high-dose corticosteroids, hematopoietic stem cell transplant (HSCT) recipient in past 24 months, HSCT recipient >24 months ago with graft-vs-host-disease or disease relapse, or having auto-immune disease with immunodeficiency as a component. Patients with advanced HIV or other immunocompromising conditions that limit innate immunity, B-cell response, and T-cell response are at greater risk for developing severe disease and potentially developing resistant mpox that could result in a higher level of virulence. The CDC advisory calls for restoration of effective immunologic control to the degree possible, for example with the resumption or optimization of antiretroviral therapy in people with HIV infection, as a critical element in the response to severe mpox. The immune response to mpox and other orthopoxviruses has been extensively reviewed by Fok-Moon Lum, et al., and should be reviewed for further detail. 4
Summary of available mpox therapies.

aAdult dosing included in table, for pediatric dosing and those weighing <40 kg, refer to respective expanded access investigational new drug (IND) protocols (U.S.) or manufacturer provided prescribing information.
bHydroxypropyl-β-cyclodextrin (excipient in IV formulation eliminated through glomerular filtration)
Patient cases
Case 1: 46 year old male with untreated, advanced HIV (CD4 count 58 cells/mm3) initially presented to multiple outside hospitals with rectal and groin pain for several days. The patient had not received the mpox vaccine. He was ultimately confirmed to have mpox on PCR testing as presentation progressed with the development of multiple skin lesions and he was treated with 14 days of tecovirimat during an admission at another facility. During this time, antiretroviral therapy (ART) with bictegravir-emtricitabine-tenofovir/ alafenamide was also initiated (his CD4 count remained <100 cells/mm3 even after initiation of therapy). Of note, 4 days after completion of tecovirimat, the patient continued to have rectal pain and ongoing pain from his other skin lesions prompting him to present to our hospital approximately 3 weeks following his original mpox diagnosis. On presentation, ulcerated, non-healed lesions were noted on his extremities, torso, face, buttocks, and genitals (Figure 1). A CT of the abdomen and pelvis revealed a 2 cm abscess in the left anterior perineal crease. An MRI of the pelvis revealed a small intersphincteric fistula without associated abscess but extensive irregular perirectal enhancement concerning for ongoing inflammation. He was continued on his ART and given medications for pain management. During his hospitalization he required aggressive wound care with twice-daily mupirocin with lidocaine, twice-daily silver silvadene, and zinc oxide three-times daily. The patient was receiving a multimodal pain control with gabapentin, lidocaine topical jelly, acetaminophen, benzocaine spray, ibuprofen, scheduled oxycodone, and fentanyl continuous infusion. He developed new lesions at his oropharynx and abdomen as well as progressively indurated and painful left inguinal lymph node. The patient continued to be febrile with progressive hypoxia requiring maximum high-flow nasal cannula support; given the paradoxical clinical deterioration in setting of recent ART initiation, there was some concern for immune reconstitution inflammatory syndrome (IRIS). ART was held for 8 days and patient was given methylprednisolone and dexamethasone during this time (methylprednisolone 32 mg q12 h × 5 days then dexamethasone 20 mg q24 h × 5 days, 10 mg q24 h × 5 days, 5 mg q24 h × 5 days) as part of empiric therapy for Pneumocystis carinii (PCP) given ongoing hypoxia at hospital day 25. A bronchoalveolar lavage was performed and a Pneumocystis assay was obtained that was negative, at which time empiric antibiotic PCP treatment was discontinued and steroids were tapered off. Fifteen days after presenting to our hospital, after discussion with the CDC, intravenous (IV) tecovirimat was started for an additional 14-day course; IV was chosen given the patients inability to take oral therapy with extensive and painful oropharyngeal lesions. Following this regimen, the patients’ condition continued to decline, and IV tecovirimat was restarted 5 days after discontinuation based on CDC recommendations and continued through the remainder of his hospital course. At multiple time points during his admission, IV cidofovir was considered, however it was decided to avoid use given the patients significant renal dysfunction that developed over the course of admission. The patient was given vaccinia immunoglobulin (VIGIV) 9,000 u/kg for 2-doses given 10 days apart, with the first dose given approximately 1 month from admission. His hospital course was complicated by development of acute respiratory distress syndrome (ARDS) requiring intubation, acute renal failure requiring initiation of continuous renal replacement therapy, CMV viremia, and severe/fulminant Clostridioides difficile infection. Unfortunately, approximately 6 weeks following admission, the patient expired due to multi-organ failure after the family had decided on comfort care measures. An autopsy was performed and key findings on preliminary report include: consolidated heavy lungs with pleural adhesions, hepatosplenomegaly, ulcerating skin lesions on the face, chest, extremities and genital area. Viral sequencing to evaluate for tecovirimat resistance was not performed. (a) (Case 1): patient presented with demarcated erosion along the gluteal fold, also present are several flesh colored and hyperpigmented papules with central crusting on the buttocks. (b) (Case 1): shows some of the observed facial lesions and also lesions on the oral mucosa. (c) (Case 2): Crusted lesions on forehead/face. (d) (Case 2): Image from bronchoscopy of the nasopharynx with presumed mpox lesions.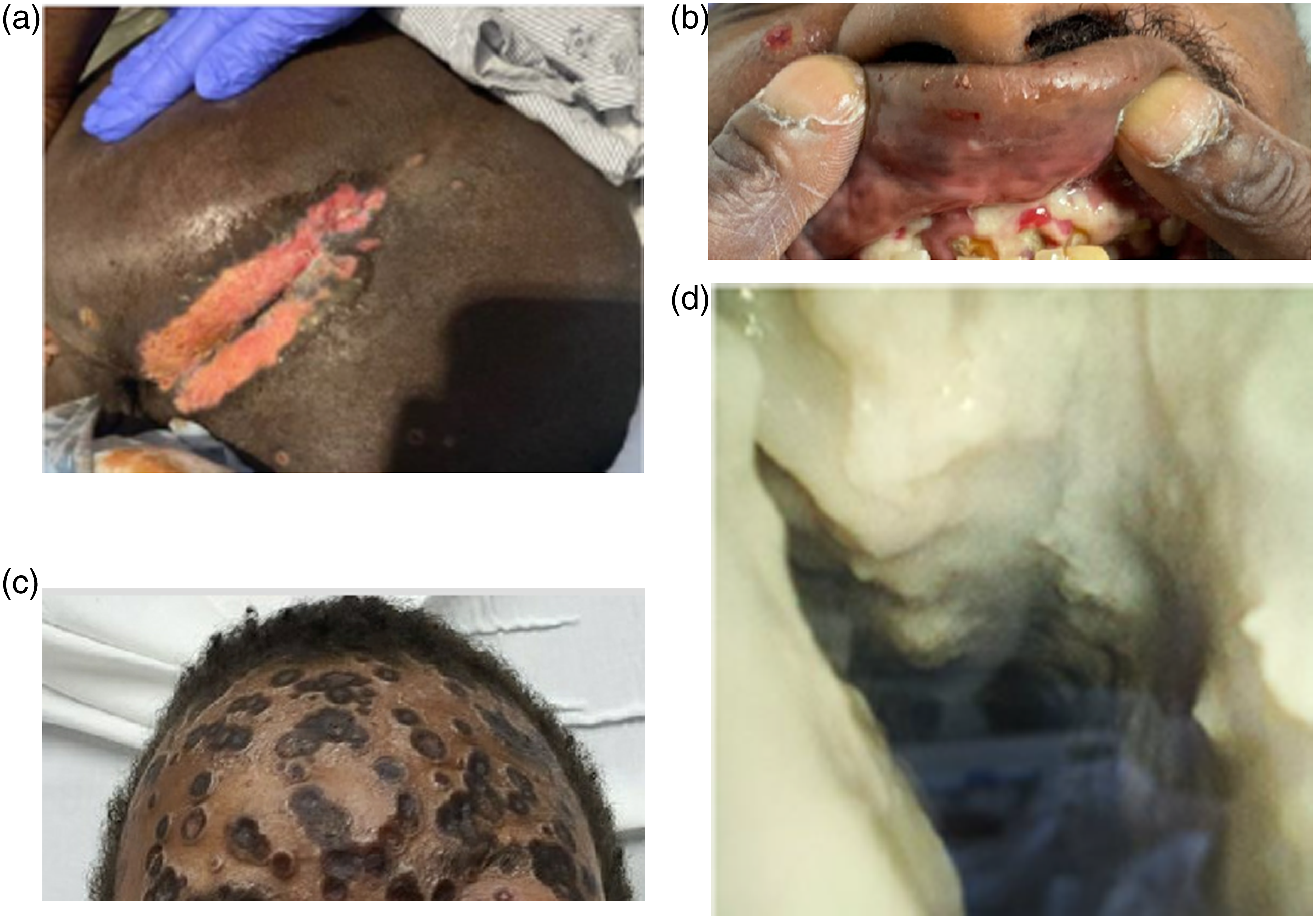
Case 2: 33 year old male with advanced HIV (CD4 9.9 cells/mm3 on admission) recently discharged from another hospital for management of mpox during which time he was also initiated ART with bictegravir-emtricitabine-tenofovir alafenamide the patient was not vaccinated for mpox. Approximately 1 month prior to admission at our institution, he was evaluated at an outside hospital emergency department (ED) for new onset lesions involving his face and mouth. One week after he was discharged home from the ED, his mpox testing returned positive, and he was seen in our Infectious Diseases clinic and started on PO tecovirimat therapy. Unfortunately, he stopped tecovirimat after 2 days, citing gastrointestinal side effects (diarrhea, abdominal pain, nausea, vomiting). Two weeks prior to admission at our institution, he presented to an outside hospital with disseminated lesions involving his mouth, face, anus, and penis complicated by extensive oropharyngeal and anorectal pain (Figure 1). In addition to mpox, he was diagnosed with candida esophagitis and infectious diarrhea (GI PCR panel positive for Shigella, norovirus, and Campylobacter); he was treated with tecovirimat as well as fluconazole, ceftriaxone and azithromycin before being discharged on oral tecovirimat, fluconazole, and doxycycline. Of note, he was also started on ART as above when hospitalized. Unfortunately, again he stopped all antimicrobials shortly after discharge, reporting difficulty tolerating medications. Two weeks after discharge, the patient presented with facial swelling now involving the jaw, eyelids, and scalp that his husband noted had progressively worsened. The patient also had increased work of breathing, cough and increasing confusion prior to admission. The patient was admitted to the medical intensive care unit, he was intubated given extensive laryngeal and tracheal edema, and started on IV tecovirimat, this was continued throughout the entirety of his admission. Prednisone was also initiated for the tracheal edema on admission and continued until day 14 (prednisone 40 mg q12 h × 2 days, 40 mg q24 h × 11 days). Intravenous cidofovir (with probenecid and fluids) was given on hospital day 5 of admission and again on day 21. After the first dose of cidofovir he developed acute kidney injury so it was decided not to redose at 1 week, he also was clinically stable at the time he was due for a second dose. It was later given on day 21 when he began to decompensate. VIGIV was also given at a dose of 9,000 u/kg on day 5 and day 11 after discussion with the CDC. His ART was held on admission and not restarted until hospital day 13 given inability to take oral therapy and there being some concern for possible IRIS despite intermittent adherence to ART. His hospital course was complicated by Pseudomonas pneumonia, CMV viremia, ESBL E. coli bacteremia, Enterococcus gallinarum bacteremia, and adenovirus viremia. He had also required intubation given severe altered mental status and reintubation for a pneumothorax. Towards the end of his hospital course, the patient had two occurrences of asystole thought to be secondary to pulmonary process (hypoxia and increased peak pressures on vent) leading to increased vagal tone causing bradycardia, associated AV block and eventually asystole. He also developed renal failure following the second dose of cidofovir requiring initiation of continuous renal replacement therapy. The patient unfortunately expired 27 days following admission with multi-organ failure. The patient’s family refused autopsy. Viral sequencing to evaluate for tecovirimat resistance was not performed.
Therapeutic options 7
Tecovirimat (TPOXX®)
Tecovirimat is an orthopoxvirus VP37 envelope wrapping protein inhibitor available in oral and intravenous formulations and is currently approved by the Food and Drug Administration (FDA) for the treatment of smallpox and the European Medicines Agency (EMA) for smallpox, mpox, and cowpox. Use for the treatment of mpox in the U.S. remains available only through an Expanded Access Investigational New Drug (IND) protocol. Use for the treatment of orthopoxviruses such as mpox was initially primarily based on animal studies showing significantly reduced viral loads, reduced clinical signs of disease, protection from severe disease, and improved survival. 8 Data are also now available on the use of tecovirimat in patients with mpox through compassionate use from a recent study where 25 patients received oral therapy. 9 Therapy was well tolerated with the most common side effects being fatigue, headache, nausea, itching and diarrhea. In this cohort of patients, 23 (93%) experienced resolution of lesions and pain by day 21. Additional studies are also now available reporting real-world use of tecovirimat for mpox during the current outbreak.10–13 Of note, recent CDC data on use of tecovirimat in the U.S., out of 369 patients receiving tecovirimat only 6.9% were hospitalized, highlighting the fact that there is minimal data on the use of this agent in patients with mpox severe enough to require hospitalization. 11
Intravenous tecovirimat is generally not recommended for patients with a creatinine clearance of <30 mL/min (due the concern of renal toxicity related to hydroxypropyl betadex accumulation), however oral therapy can be used in those with severe renal impairment. Oral is preferred, however if the patient cannot tolerate oral therapy or there is concern for poor absorption the intravenous formulation may be used. Of note, the oral capsules can be opened and mixed with water to give to those unable to swallow solid oral dosage forms and they may also be given via nasogastric tube (NGT) if there is no enteral access and the intravenous form is not available or feasible per the IND protocol. Dosing is weight based and is given every 12 to 8 h orally, or every 12 h intravenously. Of relevance, particularly for patients with HIV that may be on antiretroviral therapy, tecovirimat is a weak CYP3A4 inducer and weak inhibitor of CYP2C19 and CYP2C8. 7 The effects of tecovirimat are not expected to be of clinical relevance for most substrates of the enzymes. However, use may increase rapaglinide levels requiring close monitoring of blood glucose levels, and can decrease levels of midazolam requiring monitoring anxiolytic effectiveness. It is also recommended not to start the combination antiretroviral cabotegravir with rilpivirine during treatment and for 2 weeks after. For a comprehensive drug interaction evaluation, providers are referred to the University of Liverpool HIV medication drug interaction resource. 14
Providers are encouraged to enroll patients with mpox in ongoing clinical trials to further evaluate the safety and clinical efficacy of tecovirimat for the treatment of mpox (e.g. NCT05534984).
Vaccinia immune globulin intravenous
Vaccinia immune globulin intravenous is currently FDA approved for the treatment of complications of the smallpox vaccination that are due to continued Vaccinia virus (an orthopoxvirus similar to smallpox) replication following vaccination. There are currently no clinical effectiveness data available on the use of VIGIV for the treatment of mpox. However, there are several case reports using VIGIV for patients with other orthopoxviruses showing potential clinical efficacy, in most cases when give in combination with an antiviral agent.7,15 Use of this immune globulin provides passive immunity through orthopoxvirus-specific antibodies collected from pooled human plasma from those vaccinated with the smallpox vaccine, with high titers of anti-vaccinia antibodies. Use for mpox is also only available under an Expanded Access Investigational Drug Protocol in the U.S.
Vaccinia immune globulin intravenous has a black boxed warning for interacting with blood glucose monitoring systems requiring that glucose monitoring be performed using glucose-specific methods. While severe complications or adverse reactions are rare, similar to other immune globulin products, use can be associated with immediate hypersensitivity reactions, acute renal failure, and transfusion related acute lung injury (TRALI) among others. For mpox, the suggested dosing is 9000 Units/kg, and should be infused through a dedicated line at a rate not to exceed 2 mL/min (starting with slower rates over the first hour of administration). Clinical data on repeat doses are lacking, however it may be considered to redose based on severity of symptoms and response to treatment, doses up to 24,000 U/kg have been safely used in clinical trials as noted in the IND protocol for VIGIV use for mpox treatment. Consideration for re-dosing should be discussed with CDC. It should be considered that the mean half-life of VIGIV is 30 days with a range of 13–67 days, so the clinical utility of dosing prior to 13 days may be unclear. That said, in a case of severe post-vaccination progressive vaccinia infection in a patient with acute myelogenous leukemia following receipt of chemotherapy, VIGIV was redosed at doses ranging from 6,000 u/kg to 24,000 u/kg at multiple time points in 1-month intervals to maintain stable IgG levels. 16 Therefore the half-life of VIGIV should not be the sole parameter on which redosing decisions are based.
Cidofovir and brincidofovir
Intravenous cidofovir, a viral DNA polymerase inhibitor, is another option for the treatment of mpox, and similar to the other therapeutic options discussed there are no clinical effectiveness data available for this specific virus. Its use is only currently FDA approved for the treatment of cytomegalovirus infections in patients with AIDS. In vitro data is available that shows this antiviral to have activity against orthopoxviruses, and there are some animal data showing effectiveness.4,15 The major limitation with the use of cidofovir, which is noted as black boxed warning, is nephrotoxicity. For mpox treatment, it is suggested to dose cidofovir following the same guidance for the treatment of CMV disease, 5 mg/kg weekly for 2-doses and once-weekly thereafter (with concomitant fluids and probenecid), with dosage adjustments for patients with reduced renal function. Use of cidofovir is not recommended if creatinine clearance is < 55 mL/min, if serum creatinine is > 1.5 mg/dL, or if urine protein is ≥ 2+.
Brincidofovir is an oral lipid conjugate prodrug of cidofovir that has also been shown in in vitro and animal studies to have activity against orthopoxviruses.4,15 This agent is currently FDA approved for the treatment of smallpox. The advantage of this oral prodrug is that is not a substrate for the organic anion transporter (OATP)-1 in the renal tubules and hence is not nephrotoxic. Reported side effects include GI intolerances (nausea, diarrhea, abdominal pain, vomiting) and elevated liver function tests. Use of brincidofovir has also been found to be associated with male infertility in animal studies. 17 There are also several clinically significant drug-interactions with OATP 1B1 and OATP 1BS inhibitors such as protease inhibitors and cyclosporine that can increase the serum concentrations of brincidofovir; it is thus recommended to try to avoid these therapies or postpone the administration of these interacting medications at least 3 h after brincidofovir administration. The recommended dosing is 4 mg/kg once weekly for two doses. While not an option when we were managing the two reviewed cases, brincidofovir is now available for use in the U.S. under an Expanded Access Investigational New Drug protocol.
Trifluridine (ophthalmic)
For patients with ocular involvement or with lesions surrounding the eyes, topical trifluridine may also be added to systemic therapy. This recommendation is based on the role of this agent in managing patients with ocular vaccinia virus infections. In vitro data is available showing activity against orthopoxviruses and there are several published case reports using this agent for orthopoxvirus infections as well. Use of this agent and optimal management of ocular mpox should be discussed with ophthalmology. Suggested dosing for mpox conjunctivitis or keratitis for adults is 1 drop in the effected eye(s) every 2 h (maximum 9 drops per day) until re-epithelialization, then 1 drop every 4 h (minimum 5 drops per day) for 7 days, or until all periocular lesions have healed (maximum duration of 21 days). 18 Extended use can be associated with corneal toxicity.
Antiretroviral therapy in people with HIV infection
A recent CDC Health Advisory recommends that clinicians should optimize immune function among immunocompromised people with suspected or confirmed mpox, specifically by ensuring those with HIV are on effective antiretroviral therapy (ART). 3 As previously noted, and reviewed in detail elsewhere, T-cell response is a critical component for immune response and viral clearance. Immune reconstitution should be the primary goal in patients with severe mpox, hence prompt initiation of antiretroviral therapy and avoidance of immunosuppressive therapies should be prioritized. Delay of the initiation or resumption of ART is not indicated in almost all settings when IRIS is suspected, with the important exceptions of cryptococcal meningitis and disseminated tuberculosis. 19 The benefits of starting ART likely outweigh the risk of IRIS and its consequences with severe mpox. And while it is recognized that patients presenting with severe mpox may require corticosteroids for other indications (e.g. stress dose steroids in the setting of septic shock or severe inflammation such as airway edema resulting from mpox infection itself), limiting exposure to this therapy is advised.
Treatment decisions should be independent of mpox vaccination status
It also important to recognize that mpox can still occur despite vaccination and that treatment decisions should not be based on vaccine status. A recent analysis reported on infections following a single dose of the Modified Vaccinia Ankara-Bavarian Nordic mpox vaccine. 20 Four-hundred patients tested positive for mpox out of 7339 patients that received vaccination, with most post-vaccine infections occurring within 2 weeks of receiving the first dose (before full effectiveness was likely to be achieved). However, of concern, is that two patients had breakthrough infections 3 weeks after a second dose of the vaccine. Another study evaluating the same mpox vaccine found a vaccine effectiveness of 79%, with 3 patients in the vaccinated group with post-vaccine infection. 21 Recent CDC data reports an incidence of mpox among vaccinated individuals of 14% (796 of 5402 cases). 22 Importantly, mpox incidence was 14-times higher among unvaccinated individuals compared to those that are vaccinated.
Recommended regimen
For patients diagnosed with severe mpox disease, meeting any of the criteria for severe disease as outlined previously that are severely immunocompromised, we recommend consultation with the CDC and local departments of health, as well as immediate initiation of tecovirimat in combination with VIGIV, and brincidofovir (or cidofovir if brincidofovir is not available). While tecovirimat is the primary antiviral recommended for treatment, it is pertinent to consider combination therapy given that tecovirimat is not directly lethal to the virus as its mechanism of action targets viral spread. It also pertinent to consider combination therapy with tecovirimat to reduce the likelihood of antiviral resistance emerging given that tecovirimat has a low barrier to resistance in vitro, and the risk of resistance is likely to be greater in severely immunosuppressed patients. The combination of tecovirimat with brincidofovir has been shown to be synergistic against other orthopoxviruses 23 The addition of VIGIV for passive immunity in immunocompromised patients where host immune response will be limited is also an important component to the therapeutic regimen. CD4 T-lymphocytes are vital to a host’s ability to develop a protective antibody response. Animal model data shows that low CD4 T-lymphocyte counts (<300 cells/mm3) are associated with a lack of ability to produce vaccinia virus specific immunoglobulins following vaccination, and animals with low CD4 counts died when exposed to mpox. 24 Those with low CD4 T-lymphocytes are thought to be more likely to develop severe disease, and the lack of antibody response may predispose to mutations that could result in greater virulence.4,25 Hence the importance of providing passive immunity with VIGIV in patients with advanced HIV that are infected with mpox. Mpox convalescent plasma has been considered as another therapeutic approach in the past, however given ongoing restrictions on blood products from sexual minority men, we are unable to investigate this potential intervention given the epidemiology of the current outbreak. 26
The recommended duration of therapy for mpox in severely immunocompromised patients is not well established. While the IND protocol from the U.S. outlines the recommendation for at 14-day course of therapy with tecovirimat, in the setting of severe immunocompromise where prolonged viral replication is likely, longer durations should be considered. Therapy should ideally continue at least until the patient is no longer showing signs of end-organ involvement (e.g. extubated, off renal replacement therapy, etc.) and have clinically improved, but should not be continued longer than 90 days. There is the consideration that prolonged courses could potentially increase the risk for developing tecovirimat resistance and if available or feasible, it may be of value to perform viral sequencing. A recent update from CDC reported on two cases of tecovirimat resistance that developed in immunocompromised patients that received more than 14 days of therapy. 27 At this time however, because there is no Clinical Laboratory Improvement Amendments (CLIA) approved test for tecovirimat resistance and given resistance testing may take up to 2 weeks, concerns for resistance should be based on clinical status and therapy medications should not await confirmatory resistance testing.
Review of cases 1 and 2, lessons learned
In both cases we presented, we can derive a few important lessons. First, based on evolving data, tecovirimat should be continued in these severe mpox cases until improvement in clinical status, and perhaps avoiding stopping and restarting therapy would be of importance to avoid the risk of resistance with an antiviral with a low barrier for resistance. When the patient described in case 1 presented to the hospital with ongoing symptoms of mpox, therapy with IV tecovirimat should likely have been immediately started. Second, when tecovirimat resistance could be a concern or there is lack of response to initial therapy, additional antivirals or immunoglobulin agents should be promptly considered. Communicating with the CDC (or your applicable national public health agency) early upon presentation to discuss optimal management, recommended evaluations or laboratory assessments, and additional therapy options is highly recommended. In these cases, perhaps more timely pursuit of VIGIV would have been advantageous as well as potentially more doses and IgG monitoring following dosing. Additionally, initiation and continuation of brincidofovir (or IV cidofovir if brincidofovir is not available) should be considered in severe cases while weighing the risk and benefits of this therapy if the IV route is the only option. Finally, restarting ART and avoidance of corticosteroids should ideally be prioritized, as cellular immunity is critical in the host’s ability to clear the virus. For both of these cases, the patients developed numerous infectious complications throughout their hospital course that could have contributed to their poor outcome. However, it stands to reason that with availability and appropriate initiation of effective therapies for the other infections complications, further optimization of their mpox management was needed.
It would be remiss not to highlight the unbalanced global mpox response. The ongoing, decades-long impact of this neglected zoonoses on West and Central Africa remains largely ignored with the current multi-national outbreak. The countries with the greatest historical burden of disease have had little to no access to antiviral treatment until recently (NCT05559099). Of note, there is still not a single vaccine dose allocated to any region of Africa. Any conversation on management of severe mpox must recognize this widening gap between global disease burden and resource allocation. Countries with access must advocate for their national agencies to correct these inequities with meaningful deliverables for this current outbreak and those to come.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.