
Abstract
Malignant syphilis is an infrequent secondary manifestation in patients with human immunodeficiency virus (HIV), with polymorphous and disseminated skin lesions being related to severe immunosuppression. Lesions have intense inflammatory circinate, ulcer-crusted and nodular skin lesions of diffuse distribution throughout the body, that can be confused with vasculitis or cutaneous lymphomas. We report a patient recently diagnosed with HIV infection in the acquired immunodeficiency syndrome stage with malignant syphilis as the debut of HIV.
Keywords
Introduction
Malignant syphilis (MS) is an infrequent secondary manifestation of Treponema pallidum. The atypical lesions of MS can be confused with other causes (infectious or non-infectious diseases). A frequent manifestation is the presence of nodular-ulcerative lesions that start as papulopustular skin lesions that spread rapidly and evolve to round or oval ulcers with raised, well-defined borders and hyperkeratosis with a dark red or necrotic background 1–3
Case report
A 41-year-old heterosexual woman (reporting three sexual partners in the preceding 5 years) with a history of drug consumption, alcoholism (on treatment with quetiapine), asthma, and tattoos presented to clinic. The woman reported the development of erythematous, pruriginous, and painful plaque over the thorax, extremities, and face one month previously that had progressed to scabs with color change of skin lesion in addition to fever which subsided with antipyretics. In light of the presenting complaint, the patient was screened for sexually transmitted infections and was diagnosed with human immunodeficiency virus (HIV) and syphilis. Skin lesions at admission were well-defined circinate plaques with an intense peripheral inflammatory-necrotic reaction, raised scabs, and pustular areas with well-defined violaceous erythematous background between 2–3.5 cm diameter without altered sensitivity. These lesions were distributed on the thorax, extremities, cervical and facial region with involvement of the lower labial area (Figure 1) plus conjunctival infiltration and uveitis. The patient had no neurological symptoms. There was no lymphadenopathy found or any other abnormal findings on examination. The laboratory results showed: hemoglobin: 8.8 g/dl; lymphocytes: 834/μL; albumin: 2.53 g/dl; alkaline phosphatase and gamma-glutamyl transferase values were twice the upper limit without other alterations in the hepatic or coagulation analytic profile. The CD4 Lymphocyte cell count was 164 cells/mcl; HIV viral load: 223 000 copies/ml; hepatitis B and C virus and human T-cell lymphotropic virus serological tests were negative; rapid plasma reagin was: 1:128. Circinate skin lesions with peripheral and necrotic-ulcerative infiltrate on (a) chest (b) neck (c) lower lip (d) and necrotic scab circinate ulcers on the chest with desquamative lesions.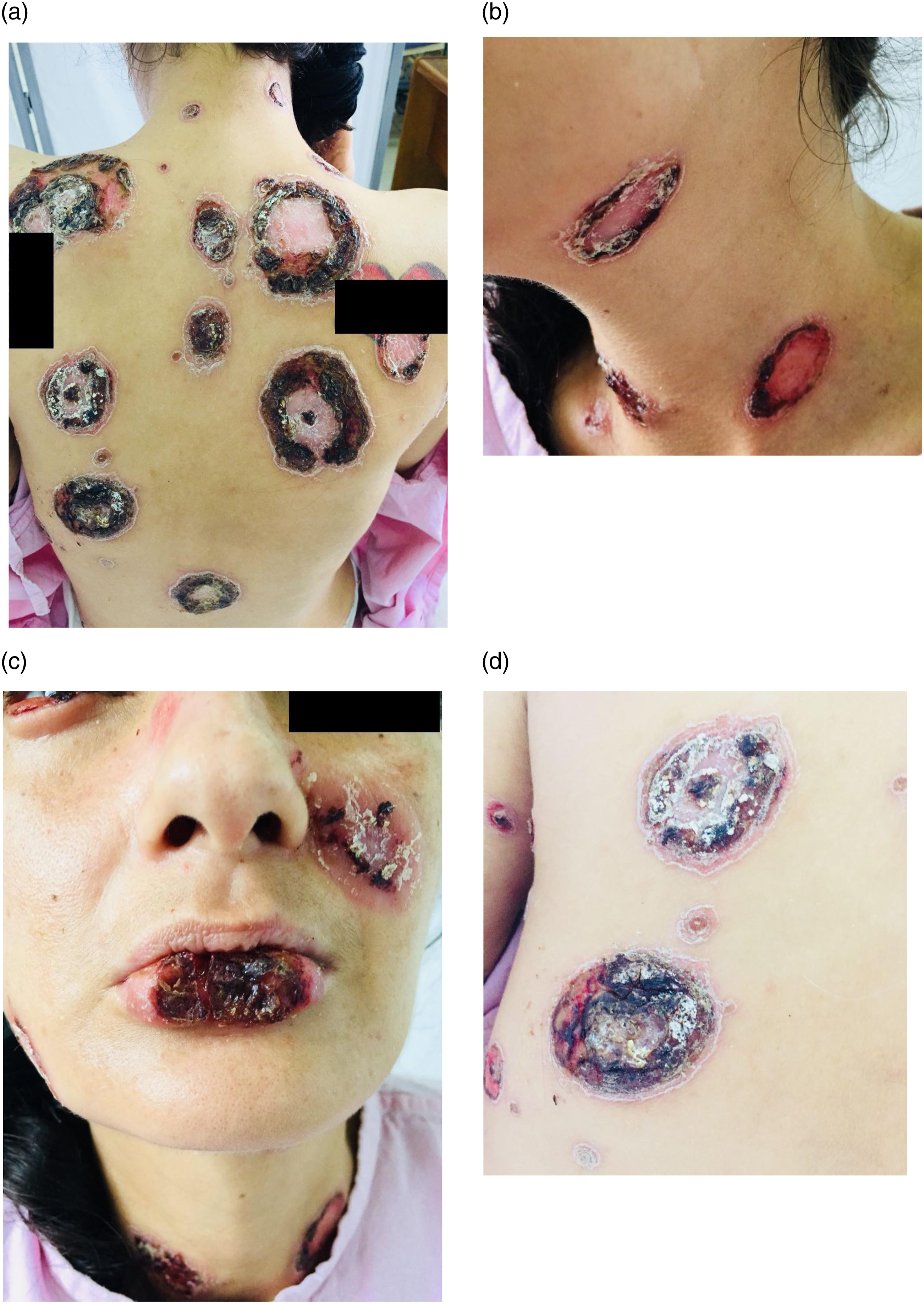
Skin biopsy showed lymphoplasmacytic-histiocytic superficial and deep perivascular and periadnexal chronic dermatitis, as well as epidermis with pseudoepitheliomatous hyperplasia, parakeratosis, neutrophilic exocytosis, spongiosis, and suprabasal vascular degeneration. Periodic acid-Schiff and Ziehl-Neelsen stains were negative. Warthin’s staining identified suspicious Treponema spp. Structures were confirmed by immunohistochemistry as Treponema pallidum (Figure 2). Cultures for fungi, mycobacteria and bacteria were negative. The patient received penicillin sodium 4 million IU 6x/daily for 14-days for uveitis, in addition to topical ophthalmic drops of ciprofloxacin/dexamethasone for 10-days. The patient showed clinical improvement and antiretroviral treatment with tenofovir/lamivudine plus lopinavir/ritonavir was started 1 month after discharge with no new manifestations of skin lesions during 1 year of follow-up. Skin biopsy: (a) HE (10x) Perivascular and endothelial lympho-histiocytic infiltrate; arrow points to Treponema structures (b) Immunohistochemical study (100x) positive for Treponema pallidum.
Discusion
MS in HIV is infrequent, and syphilis infection usually being diagnosed during a recent HIV infection.4–11 The severity4,8,10,12,13 and early presentation of MS4–6 may be related to immunocompromise. Thus, in people living with HIV with CD4 levels ≤200 cells/ml, non-treponemal serology (RPR) dilutions titers are low (<1:64),4,8 unlike those of patients with CD4 levels >200 cells/mm3 and nontreponemal serology titers ≥1:128.5–7,9,10 Therefore, this presentation may be observed in people with controlled HIV or non-immunosuppressed patients.
According to Fisher et al. the diagnostic criteria of MS are: (1) high serologic titers, (2) Jarisch-Herxheimer reaction, (3) suggestive histopathology findings, and (4) response to antimicrobial therapy. Our report meets three of these four criteria (the patient did not develop Jarisch-Herxheimer), and corticosteroids administration was not necessary as in most HIV-MS reports.5–7,9,11
Fever, myalgia, and headache2,3,5 are described as prodromal and self-limited as described in this case report. In other cases neurological manifestations which have also previously been reported,4,7,8 were absent in our case, but uveitis was considered related to syphilis. Skin lesions mainly involve the face, neck, and thorax; and spread rapidly and evolve into round or oval ulcers with raised, well-defined borders and hyperkeratosis with a dark red or necrotic background.2,3,15,16 These may be due to mucosal compromise and superficial infection aggregate.4–10 Our case had lesions in the lower labial area and initially reported yellow secretion from the skin lesions as a possible overlapping bacterial skin infection. Histopathology usually reports granuloma in patients without HIV,13,14 that it is absent in HIV patients regardless of the CD4 cell count.4–10 In most cases perivascular and endothelial lymphocytic infiltration are common, 11 similar to that described in our report.
Standard antimicrobial therapy in the MS usually includes benzathine penicillin in some cases, or procaine (1.2 million units daily for 3 weeks, intramuscularly) 7 or sodium (4 million units every 4 hours for two weeks, intravenously)4,8 when there is neurologic or ophthalmologic compromise as in our case with uveitis. Our case did not develop Jarrisch-Herxeimer reaction with penicillin and showed clinical improvement after treatment completion similar to previous cases described in the literature.5–7,9,11
This case evidenced typical MS skin lesions in a patient with acquired immunodeficiency syndrome as the debut of HIV. Despite presenting a disseminated and intensive reaction, clinical improvement was achieved with only the administration of penicillin treatment, with no further complications described.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.