
Abstract
Background
Syphilis is one of the most common sexually transmitted infections (STIs), and it remains a significant public health concern, particularly in low-resource settings including sub-Saharan Africa. There are limited data on the prevalence of syphilis among pregnant women living with HIV in South Africa. This study determined the prevalence of syphilis infection in pregnant women living with HIV by the polymerase chain reaction (PCR).
Methods
This was a cross-sectional study that included 385 pregnant women living with HIV recruited from the antenatal clinic at the King Edward VIII Hospital in Durban, South Africa between October 2020 and April 2021. Treponema pallidum was detected using the Applied BiosystemsTM TaqMan® Assays from stored DNA samples extracted from vaginal swabs.
Results
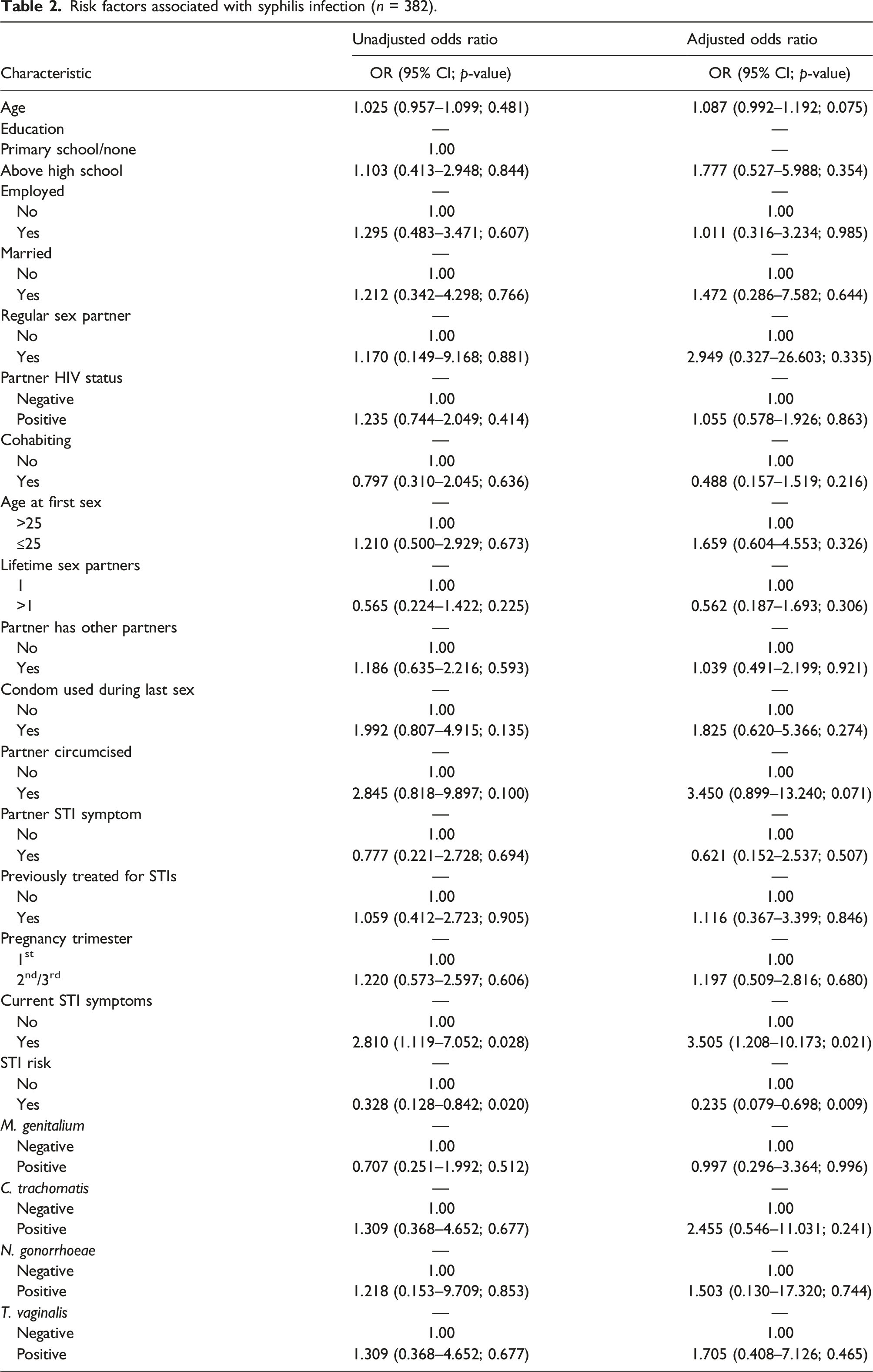
The prevalence of syphilis was 5.2% (20/385). The overall median (Q1–Q3) age of the women was 30.0 years (25.0–36.0). Of the women who tested positive for syphilis, 60.0% had reported STI symptoms (p = 0.030) and of those, 65.0% did not perceive themselves at risk of contracting STIs (p = 0.019). Women who reported having STI symptoms were more likely to test positive for syphilis when compared to women who reported not having any STI symptoms (OR: 2.810; 95% CI 1.119–7.052; p = 0.028). Women who perceived themselves as being at risk of contracting STIs were less likely to test positive for syphilis when compared to women who did not perceive themselves at risk of contracting STIs (OR: 0.328; 95% CI 0.128–0.842; p = 0.020).
Conclusion
The study has indicated syphilis is prevalent among pregnant women living with HIV in Durban, South Africa however STI risk perception is low. Educational programs on STIs are essential among pregnant women attending antenatal care clinics in Durban.
Introduction
Syphilis is one of the most common sexually transmitted infections (STIs), and it remains a significant public health concern, particularly in low- and middle-income countries including sub-Saharan Africa. 1 This sexually transmitted infection can be transmitted vertically,1,2 and can occur at any stage of gestation. 3 The World Health Organization 4 (WHO) estimated that ∼900000 and ∼661000 cases of maternal and congenital syphilis, respectively occurred in 2019. Some recent studies on African pregnant women have reported syphilis prevalence of 1.9% (Nigeria) 5 ; 3.3% (South Africa) 6 and 5.1% (Ethiopia). 7
Untreated syphilis infections during pregnancy have been associated with adverse pregnancy outcomes such as stillbirths, congenital anomalies, intrauterine growth restriction and neonatal morbidity, and mortality.1,2,8 Syphilis also increases the risk of HIV transmission and acquisition and alters the natural history of HIV.9,10 Screening for maternal syphilis during the early stages of pregnancy and prompt treatment of positive mothers cures syphilis in the mother and prevents negative impact on the baby. 8 In South Africa, point-of-care (POC) syphilis screening is performed routinely as part of the standard antenatal services. This was implemented to reduce adverse outcomes associated with syphilis and improve antenatal healthcare access. 11
The high prevalence of maternal and congenital syphilis has been attributed mainly to inadequate prenatal care worldwide. 12 Other risk factors that have been associated with syphilis include poverty, history of other STIs, HIV infection, teenage pregnancy, low education level, history of syphilis in previous pregnancies, low income, and multiple partners. 12
Nucleic acid amplification techniques (NAATs) such as routine PCR, real-time PCR, and nested PCR can be used for the diagnosis of syphilis.13,14 However, it is recommended that NAATs may be used as supplemental diagnostic techniques for syphilis screening.14,15 The specificity and sensitivity of these NAATs differ depending on the stage of syphilis infection and the technique used. 13 In the current study, only vaginal swabs were available for the screening of syphilis by PCR. Therefore, this study determined the prevalence of syphilis infection in pregnant women living with HIV by PCR. We acknowledge that this is not the ideal diagnostic method and that the prevalence of syphilis may be underestimated. This study also provided data on the risk factors associated with infection, which is currently lacking in our setting. The identification of significant risk factors will assist with the development and implementation of risk reduction interventions.
Materials and Methods
Ethical Statement
Ethics approval for this study (BREC/00001382/2020) was obtained from the Biomedical Research Ethics Committee (BREC), University of KwaZulu-Natal (UKZN).
Study Population
This was a cross-sectional study that included 385 pregnant women living with HIV recruited from the antenatal clinic at the King Edward VIII Hospital in Durban, South Africa. The recruitment for this study was conducted between October 2020 and April 2021. The women who were enrolled in the study were 18 years and older, living with HIV, willing to provide written informed consent, and willing to provide a self-collected vaginal swab sample to be tested for STIs. Women were educated on the complications of STIs during pregnancy and provided with information on risk reduction for STIs. Both symptomatic and asymptomatic women were included in the study. Women who complained of having STI symptoms (abnormal vaginal discharge, odour, itching, sores/ulcers, warts, and pain during urination) underwent a physical examination by the attending physician. However, these results were not available for this study reporting.
Data collection
Each enrolled woman provided a self-collected vaginal swab (dry swab) for the detection of vaginal infections and completed a questionnaire on sociodemographic, behavioural, and clinical factors. A standardized questionnaire was used to capture data on risk perception. This questionnaire included factors associated with the risk of STIs and these have been previously validated. The risk assessment form (Supplementary Material 1) and the participant enrolment form (Supplementary Material 2) used for data collection are available as supplementary material.
Sample Processing and DNA extraction
After collection, each vaginal swab was suspended in 2 mL of phosphate-buffered saline (PBS). Following vortexing and rinsing in PBS, the swabs were discarded. The remaining suspension was centrifuged at 14000 rpm for 10 minutes and the supernatant was discarded. Recovered pellets were then subjected to DNA extraction. DNA extraction was performed using the PureLink Microbiome Kit (ThermoFisher Scientific, United State), according to the manufacturer’s instructions. The concentration of extracted DNA was measured using the Nanodrop spectrophotometer (ThermoFisher Scientific, United States).
Detection of Treponema pallidum
PCR amplification was performed on the Quant Studio 5 Real-time PCR detection system (ThermoFisher Scientific, United States), in a 96-well microtiter reaction plate using the Applied BiosystemsTM TaqMan® Assays. Commercial primers and probes (Ba04646237_s1) targeting the polA gene of T. pallidum were used. Briefly, each reaction was performed in a final volume of 10 μL consisting of 1 μL FAM-labelled probe/primer mix, 5 μL Fast Start master mix (ThermoFisher Scientific, United States), 1.5 μL template DNA, and nuclease-free water. The runs also included a non-template control reaction. Amplification was performed under the following cycling conditions: 1 cycle at 95°C for 30 seconds followed by 45 cycles of denaturation at 95°C for 3 seconds and annealing at 60°C for 30 seconds. Detection of fluorescent products was performed at the end of the annealing period. The raw fluorescent data was automatically generated by the Quant studio 5 Real-time PCR system software.
Statistical Analysis
Significance testing was performed using the Mann-Whitney U test (also known as the Wilcoxon rank sum test), Fisher’s exact test, and Fisher-Freeman-Halton test for continuous variables, categorical binary variables, and categorical variables with 3 or more levels, respectively. Significance testing and odds ratios were calculated in IBM SPSS Statistics version 27 (IBM Corporation, Armonk, NY).
Results
Baseline characteristics and prevalence of syphilis
Baseline characteristics of the pregnant women who were screened for syphilis infection.

aCurrent STI symptoms–abnormal vaginal discharge, odour, itching, sores/ulcers, warts, and pain during urination.
Sociodemographic, behavioural, and clinical factors
In this study, none of the sociodemographic factors were significantly associated with syphilis infection (p > 0.05). However, of those who tested positive for syphilis (16/20; 80.0%) had a high school level of education, (14/20; 70.0%) were unemployed, and (17/20; 85.0%) were unmarried.
Under behavioural factors, most of the pregnant women living with HIV who tested positive had a regular sex partner (19/20; 95.0%), had partners living with HIV (11/20; 55.0%), were not co-habiting with their partners (13/20; 65.0%), reported 15–20 years as the age at sexual debut (16/20; 80.0%), and had circumcised partners (17/20; 85.0%). However, all these factors had no statistically significant association with syphilis status (p > 0.05).
For the clinical factors, of the 20 pregnant women who tested positive for syphilis infection, 12 (60.0%) reported STI symptoms as follows: abnormal vaginal discharge, odor, itching, sores/ulcers, warts, and pain during urination. Having current STI symptoms was significantly associated with testing positive for syphilis (p = 0.030). In terms of gestation age, most of the women who tested positive were in the third trimester of pregnancy (12/20; 60.0%), 65.0%, (13/20) had not been previously treated for STIs, and 85.0% (17/20) had partners that had no STI symptoms. None of the women who tested positive engaged in any intravaginal practices. All these associations were not statistically significant. Sixty-five percent (p = 0.019) of the women who tested positive perceived themselves as not being at risk of contracting STIs. The presence of other STIs (M. genitalium, N. gonorrhoeae, T. vaginalis, and C. trachomatis) was not significantly associated with testing positive for syphilis.
Risk factors associated with syphilis
Risk factors associated with syphilis infection (n = 382).
Discussion
Recently, a steady rise has been reported in the prevalence of syphilis among pregnant women. 16 This study reported a prevalence of 5.2% among pregnant women living with HIV from South Africa. Of the women who tested positive for syphilis, 60.0% had reported STI symptoms and of those, 65.0% did not perceive themselves at risk of contracting STIs. Women who reported having STI symptoms were more likely to test positive for syphilis when compared to women who reported not having any STI symptoms. Women who perceived themselves as being at risk of contracting STIs were less likely to test positive for syphilis when compared to women who did not perceive themselves at risk of contracting.
In this study cohort of pregnant women living with HIV from Durban, South Africa, the prevalence of syphilis by PCR was 5.2%, demonstrating that syphilis infection rates remain high in the South African context. In 2019, The South African National Antenatal Sentinel HIV Survey reported a national prevalence of 2.6% (95% CI: 2.4−2.9%) among pregnant women living with and without HIV. 17 Our findings are slightly higher than the prevalence reported by the National Antenatal Sentinel HIV Survey. From the 2019 survey, the prevalence of syphilis in KwaZulu-Natal was 3.2%, with the highest prevalence of 3.8% observed in the Eastern Cape. 17 Another study conducted between 2016-2017 on South African pregnant women living with HIV using surveillance data from the National Health Laboratory Service’s Corporate Data Warehouse (NHLS CDW), reported a syphilis rate of 3.3% (5943/178 319). 6 The high prevalence observed in this study may be due to the fact that KwaZulu-Natal, the province where Durban is located has been shown to have the highest HIV and STI prevalence. 18
In this study, all the participants were living with HIV. Therefore, the HIV and syphilis co-infection rate was 5.2%. Our findings are similar to the HIV and syphilis co-infection rate of 5.6% reported by a study conducted on pregnant women from Durban, South Africa. 19 Onyangunga et al. (2020) conducted a prevalence study in a regional hospital in the south of Durban (South Africa). From their study population, the prevalence of maternal syphilis and HIV co-infection was 1.6% (72/4451) which was lower than the current study’s co-infection rate. 16 In a study conducted on Ethiopian pregnant women, 5.1% (25/494) of the women tested positive for syphilis with an overall prevalence of 2.2% for syphilis and HIV co-infection. 7 The differences in the syphilis infection rates in these studies may be due to the different diagnostic techniques and the specimen used for testing. In the other studies, syphilis was diagnosed using rapid plasma reagin (RPR) in blood samples. Although PCR of vaginal swabs was used as a detection method in our study, the findings provide evidence that syphilis infection rates remain high among pregnant women living with HIV in Durban, South Africa. Future studies using serological testing are required in this population to determine the true prevalence of syphilis. Despite the fact that the use of PCR for syphilis diagnosis is not ideal, our findings provide evidence that larger population surveillance studies are needed regularly in South Africa to monitor syphilis prevalence.
Although serological testing remains the standard diagnostic method for syphilis diagnosis, 20 PCR has been shown to have high specificity and sensitivity for the diagnosis of primary syphilis.13,15 In contrast, the sensitivity of PCR for secondary and latent syphilis has been shown to be poor and this technique has been considered unnecessary since it adds little value over serology testing. 14 Previous studies, which compared serological testing and PCR reported conflicting results. Brischetto et al. 21 (2018) concluded serology to be sufficient for primary syphilis diagnosis without the need to perform PCR. Vrbova´ et al. (2020) reported that PCR can improve syphilis testing, particularly in individuals with discordant serology results. 15 In the current study, syphilis was detected using real-time PCR without performing serological testing to detect other stages of syphilis infection. In addition, the use of vaginal swabs for sample collection might have influenced the prevalence observed. The true prevalence of syphilis in this study population may be underestimated due to the low sensitivity of PCR and the use of vaginal swabs. Nonetheless, the prevalence observed in this study provides evidence that syphilis infection rates among South African pregnant women living with HIV remains high.
Syphilis infection progresses in multiple stages which can be symptomatic and asymptomatic. 22 Symptoms of syphilis may be aggravated in people living with HIV. People living with HIV are more likely to have severe clinical manifestations of infection such as multiple and larger ulcers. Furthermore, they may have overlapping primary and secondary infections. 10 In the current study, the majority (60.0%) of the women who tested positive for syphilis reported STI symptoms (abnormal discharge, vaginal odor, genital itching, genital ulcers and/or warts, dysuria). However, a study conducted by Gilbert et al. (2021) among people testing positive for syphilis and living with HIV in Africa, showed a lack of symptoms associated with STIs. 9
In this study cohort, it is alarming that the majority (65.0%) of the women who considered themselves to be at no or low risk of contracting STIs tested positive for syphilis. This provides evidence that the majority of pregnant women had inadequate awareness and/or knowledge of STIs and risk factors that contribute to contracting STIs. A study assessing the knowledge of STIs and associated factors amongst pregnant women in Gambia (n = 280), found that 100.0% of the participants were aware of HIV, 10.4% aware of gonorrhea and only 1.1% were aware of syphilis. 23 Another study assessing knowledge, perceptions of risk, and sexual behaviors in Mozambican women, showed that all participants were knowledgeable about HIV, had heard about gonorrhea (87.0%), cervical cancer (56.0%), syphilis (41.0%), candidiasis (19.0%) and trichomoniasis (15.0%). Furthermore, the authors of that study observed that most of the women demonstrated a low level of self-perception of contracting other STIs (other than HIV). 24 The low level of risk perception and knowledge of STIs in these studies highlight the need for more effective educational and awareness campaigns about other STIs in addition to HIV.
Risk factors associated with STIs have been shown to differ among different population groups and geographic locations. In the current study, syphilis was associated with STI symptoms and the perceived risk of contracting STIs. Women that reported STI symptoms were 3.5 times more likely to test positive for syphilis infection. This finding suggests that syphilis testing should be performed in pregnant women that report STI symptoms during any stage of gestation. Risk perception was also a risk factor significantly associated with testing positive for syphilis. Women who perceived themselves as being at risk of contracting STIs were 76.5% less likely to test positive for syphilis. Surprisingly, women who perceived themselves to be at no or low risk of contracting STIs were more likely to test positive. Previous studies on pregnant women reported living in a rural or semi-urban area, having 1–4 previous pregnancies, 25 younger age, illiterate or primary education level, and a positive HIV status 26 as risk factors associated with syphilis. Another study among pregnant women from Brazil reported drug use during pregnancy and a history of abortion to be risk factors associated with syphilis. 27
The main limitation of this study is that clinical symptoms were self-reported by study participants. There was no clinical examination by a nurse or physician for clinical manifestations such as genital ulcers, skin rash, and mucosal lesions. Physical examination and serological testing were only performed by the attending physicians as part of the routine screening in the clinic and the results were not available for this study reporting. Secondly, this study did not include women living without HIV for comparing the prevalence of syphilis between women living with and without HIV. Lastly, this study only performed PCR testing on vaginal swabs and serological testing was not performed. This might have produced results that underestimate the true syphilis prevalence in this study cohort. Despite these limitations, this study provides evidence that syphilis is prevalent in this population.
Conclusion
Although syphilis testing was performed using vaginal swabs PCR, the current study provides evidence that the prevalence of syphilis is high among pregnant women living with HIV from Durban, South Africa. The high percentage of women that reported STI symptoms and tested positive for syphilis indicates that testing should be performed at any gestational age for symptomatic women. It is evident that women from this study setting have poor knowledge about STIs and low STI risk perception. Educational and awareness programs for pregnant women and other high-risk populations are necessary to improve their STI knowledge, sexual behaviors, and risk perception.
Supplemental Material
Supplemental Material - Prevalence of Syphilis in Pregnant Women Living With Human Immunodeficiency Virus (HIV) From South Africa Using a Molecular-Based Assay
Supplemental Material for Prevalence of Syphilis in Pregnant Women Living With Human Immunodeficiency Virus (HIV) From South Africa Using a Molecular-Based Assay by Mabaso Nonkululeko, Ngobese Bongekile, Wail M. Hassan, and Abbai Nathlee in International Journal of STD & AIDS
Footnotes
Acknowledgements
We acknowledge the King Edward VIII Hospital antenatal clinic management and the women who participated in this study.
Declaration of conflicting interests
The Authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research: This work was supported by the Institut Mérieux Research Award.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.