
Abstract
We report the first published case of a drug induced liver injury (DILI) presumed secondary to a drug-drug interaction between ritonavir and levonorgestrel progestogen-only emergency contraception (POEC). Our patient is a 25-year-old female living with human immunodeficiency virus (HIV), taking antiretroviral therapy (ART) containing tenofovir alafenamide/emtricitabine and darunavir/ritonavir. She was found to have elevated transaminases at a routine clinic appointment consistent with hepatocellular DILI. Further investigation found the most likely cause of this was a drug-drug interaction (DDI) between the ritonavir component of her ART and recent use of levonorgestrel POEC 3 days earlier. Evidence suggests that ritonavir increases levonorgestrel exposure, yet our patient received double the usual dose as per dispensing guidance at the time. We review the pharmacokinetics of ritonavir-levonorgestrel DDIs and highlight the need for consistent guidelines on this topic.
Keywords
Introduction
Levonorgestrel is a commonly prescribed form of POEC. This report describes probable DILI following use of POEC in a patient taking darunavir/ritonavir ART for HIV. Various guidelines exist for prescribers and dispensers of POEC to avoid clinically-significant drug interactions.1–4 At the time of writing, there are discrepancies between guidelines on the expected interactions between ritonavir and levonorgestrel. We review the complex pharmacokinetics of ritonavir, and available data suggesting ritonavir increases levonorgestrel exposure.
Case report
A 25-year-old female with well-controlled, vertically-transmitted HIV attended a routine appointment. She was established on tenofovir alafenamide/emtricitabine and darunavir/ritonavir, with an undetectable viral load. Blood tests demonstrated transaminitis (alanine aminotransferase (ALT) 535, aspartate aminotransferase (AST) 380 IU/L). Repeat monitoring after 24 h showed an ALT rise to 1115 IU/L, prompting admission. On examination she had mild right upper quadrant tenderness, but was not jaundiced. Viral hepatitis and autoimmune screens were negative apart from the antinuclear antibody (ANA) (1:160, fine-speckled pattern), previously investigated and felt secondary to HIV. Abdominal ultrasound was normal.
Drug history identified two new medications: tobramycin/dexamethasone eye drops for keratitis completed the previous day and levonorgestrel POEC taken 3 days prior. The patient denied using herbal supplements or illicit substances and reported alcohol consumption of 4 units/week.
Three days before presentation, the patient had attended a community pharmacy for emergency contraception and disclosed her ART use to ensure there were no interactions. The pharmacist consulted current guidance on DDIs and advised her to take 3 mg (double the normal 1.5 mg dose) of levonorgestrel POEC, due to potential interactions with ritonavir reducing the efficacy of levonorgestrel.
Following admission, ALT peaked at 1228 IU/L and AST at 683 IU/L (Figure 1). The patient remained asymptomatic and was discharged with a diagnosis of likely hepatocellular DILI presumed secondary to levonorgestrel POEC. The Roussel-Uclaf causality assessment method (RUCAM) score was 7, indicating levonorgestrel was a “probable” cause for her DILI.5,6 Liver enzyme levels over course of DILI.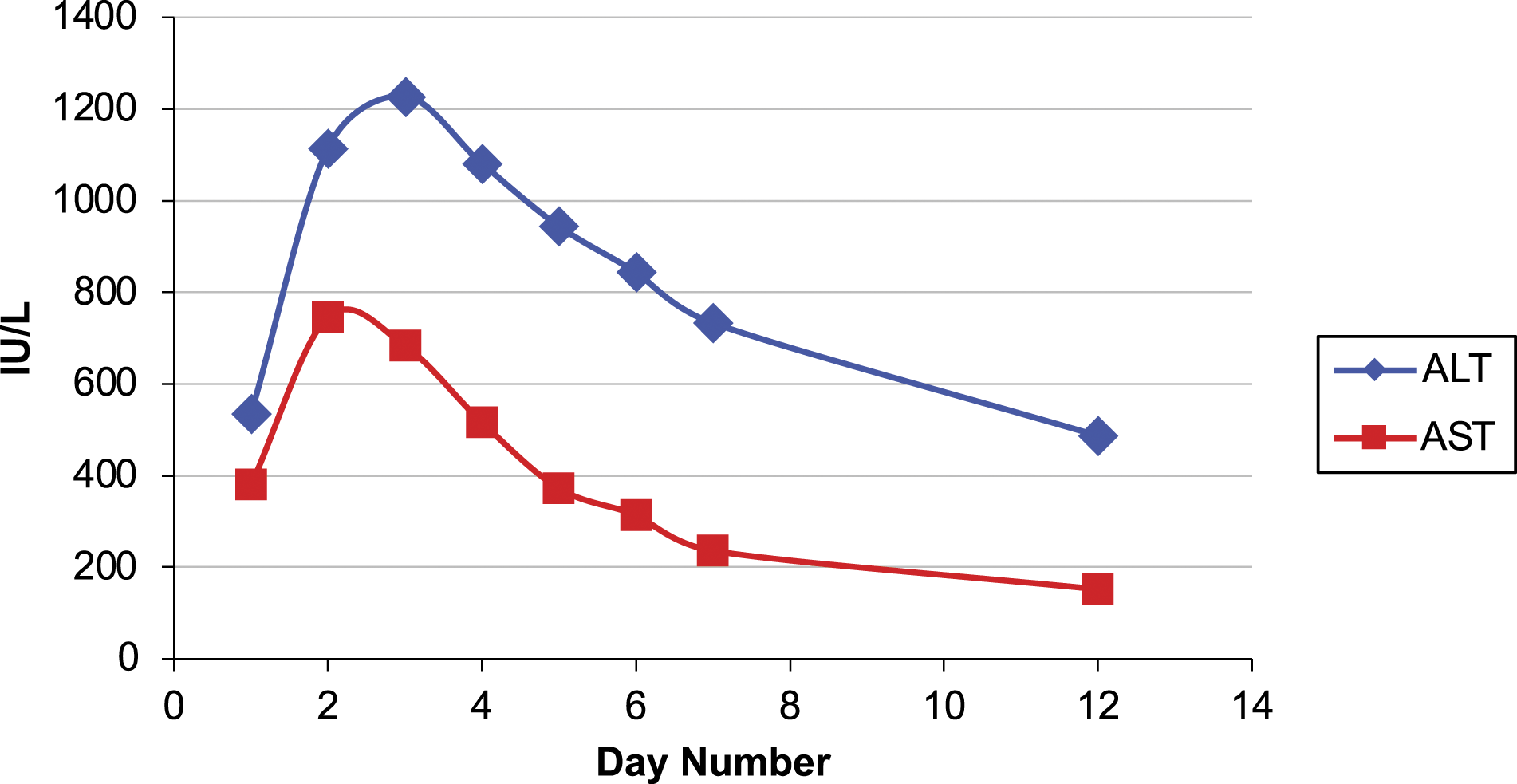
Discussion
The primary resources on contraception available for prescribers and pharmacists in the UK are the British National Formulary (BNF), and the prescribing guidelines from the Faculty of Sexual and Reproductive Healthcare (FSRH).1–3 Those prescribing ART or co-medications to people living with HIV, should additionally consult the Liverpool HIV Drug Interactions website. 7
At the time of this case, FSRH guidance classified ritonavir as a cytochrome P450 enzyme inducer, stating it might “decrease contraceptive efficacy” and “reduce the bioavailability of progestogens by inducing glucuronidation”. 1 For women on enzyme-inducing medication requesting emergency oral contraception, a single dose of 3 mg levonorgestrel (double the normal dose) was recommended by the FSRH, the BNF and the Medicines and Healthcare products Regulatory Agency (MHRA), where ritonavir was repeatedly mentioned to “decrease the efficacy of levonorgestrel”.3,4,8
Ritonavir has complex pharmacokinetics, with both enzymatic inducing and inhibitory activities. Its use as a pharmacokinetic enhancer for protease inhibitors in ART relies on its inhibition of CYP3A4-mediated phase I metabolism of these drugs. 9 Whilst ritonavir also inhibits CYP2D6, it is a clinically-significant inducer of other cytochrome P450 members. 10 Furthermore, ritonavir is an inducer of other enzymes, including uridine diphosphate–glucuronosyltransferase (UGT). Induction of UGT increases glucuronidation of certain drugs during phase II metabolism, reducing their bioavailability. Therefore, whether to consider ritonavir a pharmacokinetic inducer or inhibitor is not only drug-specific but may differ between different stage of a drug’s metabolic pathway.
Levonorgestrel undergoes phase I metabolism by CYP3A4 and CYP3A5, and phase II UGT-dependent glucuronidation. Therefore ritonavir’s effect on levonorgestrel bioavailability might be difficult to predict.11,12 However, pharmacokinetic studies in patients taking levonorgestrel-containing combined-oral-contraceptives and subcutaneous implants have shown that concurrent ritonavir use increases exposure to levonorgestrel.13,14 This suggests that ritonavir’s CYP3A4-mediated inhibitory DDI is more clinically significant, and is reflected on the Liverpool HIV Drug Interactions website. 7
Based on such data, the FSRH recently released new guidance advising to use normal doses of levonorgestrel in patients taking ritonavir. 15 However, the BNF continues to state that ritonavir is expected to decrease levonorgestrel efficacy, and levonorgestrel’s summary of product characteristics continues to recommend double dose levonorgestrel.8,16
There are multiple reports of DILI in response to combined-oral-contraception containing levonorgestrel/oestrogen, including reports to the MHRA.17,18 Reports include one case where the DILI returned on re-challenge, a case in a patient taking a boosted protease inhibitor for HIV, and a case of confirmed panacinar hepatitis secondary to the levonorgestrel intrauterine system (IUS).19–21 To our knowledge, there are no reports of DILI secondary to the use of levonorgestrel POEC and none are listed by the MHRA. 17
In conclusion, we present the first case of presumed DILI secondary to a levonorgestrel POEC interaction with ritonavir, resulting in increased exposure to levonorgestrel. The prevalence of such reactions is unknown. Whilst the FSRH no longer recommends double dose levonorgestrel, further clarification from other sources of guidance is required to better inform safe prescribing in community settings.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent
The patient has provided written consent for the publication of the information in this present work. A copy of the signed consent form is available on request.