
Abstract
Mpox virus infection (MPXV) has recently been recognized as a public health emergency by the World Health Organization. While several studies have described the clinical characteristics of MPXV-oral lesions, there remains a dearth of information regarding the histological and ultrastructural oral findings. A 24-year-old HIV-positive man presented with a shallow ulcer, covered by a fibrinoid membrane, and surrounded by an erythematous halo in the hard and soft palate. The clinical appearance of the lesion raised suspicion of a viral infection; thus, the diagnosis was based on histological and electronic microscopy findings and confirmed by RT-PCR testing in the skin specimen. This case report aims to offer comprehensive insights into the clinical, histopathological, and ultrastructural features of oral lesions caused by MPXV in an individual with HIV. This report provides valuable information about the characteristics of MPXV infection in the oral mucosa, particularly in people living with HIV.
Keywords
Background
In 2022, the World Health Organization (WHO) declared MPXV virus infection (MPXV) as a public health emergency of international concern; to January 2023, 84,471 cases were reported in 110 countries. 1 The upsurge of MPXV is primarily observed in middle-aged men, with a significant proportion of people living with human immunodeficiency virus. 2
Several recent reports on MPXV-oral lesions have been published.3–10 Two scoping reviews3,4 and a meta-analysis 5 have provided valuable insights into the presence and clinical characteristics of MPXV-oral lesions. However, to our knowledge, information regarding the histological and ultrastructural MPVX findings in the oral mucosa is not available. The purpose of this work is to present the clinical, histopathological, and ultrastructural characteristics of an individual with both HIV and MPXV infection, to contribute to the knowledge of the oral mucosae manifestations of this entity.
Case description
A 24-year-old man was referred to the Oral Medicine and Pathology Service at an HIV/AIDS-referral center in Mexico City. The patient presented with a three-day-old lesion on the palate, which was preceded by a multifocal cutaneous rash on the thorax and pubis. The rash had significantly diminished at the time of the consultation, leaving behind a shallow erythema of the trunk (Figure 1(a)); crusty lesional remnants were also observed (Figure 1(b)). The patient also presented other symptoms such as headache, fever, weakness, fatigue, pharyngodynia, and diaphoresis. Clinical presentation of MPVX. (a) Diffuse erythematous area disseminated to the trunk. (b) Crusty and umbilicated papule on the trunk. (c) Large irregular-shaped red patch with a central ulcerated and necrotic area, partially covered with a fibrinous pseudomembrane, located on the hard and soft palate. (d) Grey-brown patch exhibiting superficial ulceration covered by pseudo fibrin in the upper left alveolar gingiva.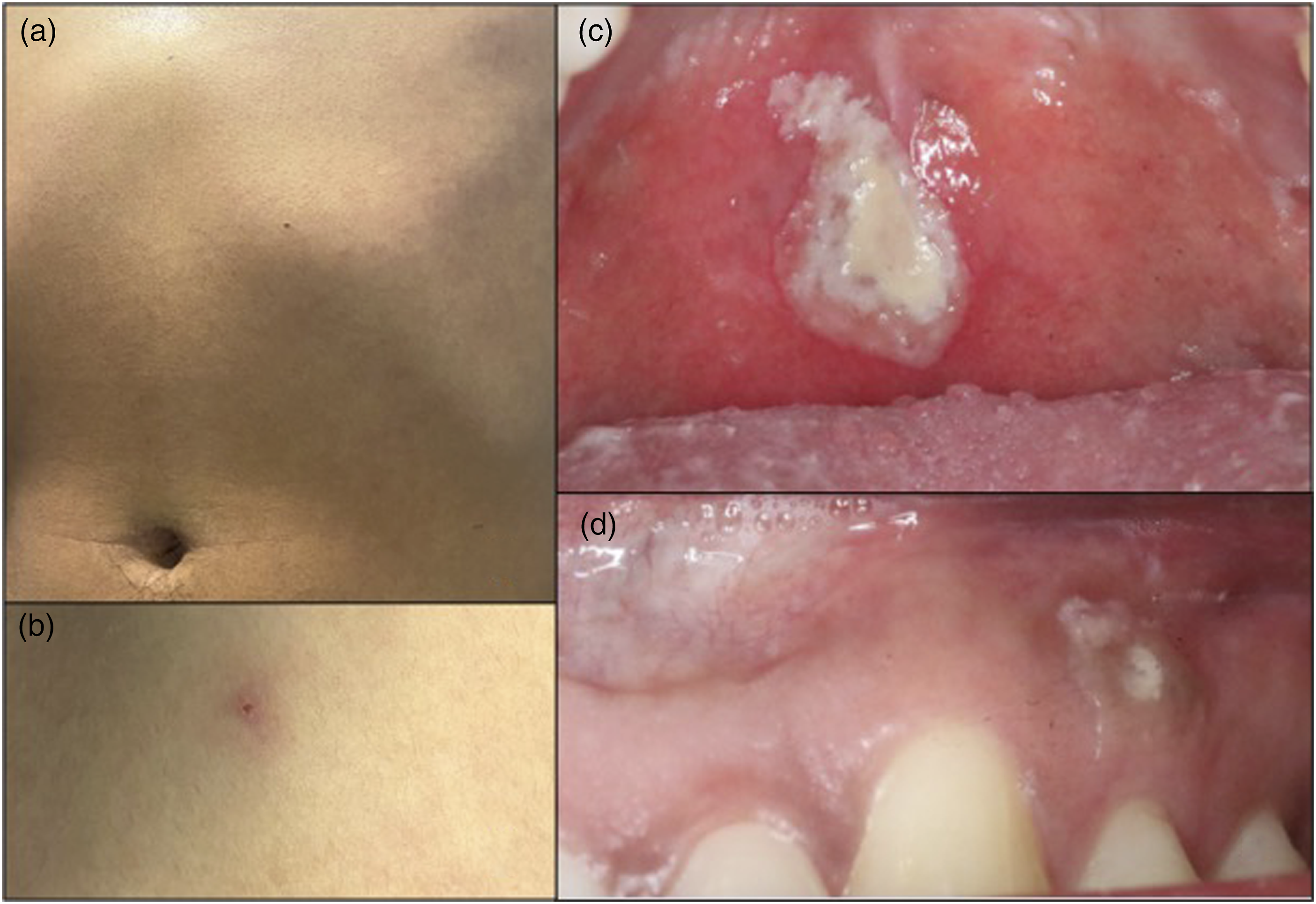
The patient was notified as HIV-positive in November 2022, starting antiretroviral treatment 1 month later (bictegravir/emtricitabine/tenofovir alafenamide), which improved the course of the HIV disease (CD4 lymphocytes: 398 cells/mm3, and undetectable HIV-plasma viral load).
On oral examination, a 3 cm shallow ulceration with well-defined but irregular edges was identified. The ulcer was covered by a fibrinoid membrane, and was surrounded by an erythematous halo, which was extended to the mucosa of the hard and soft palate (Figure 1 (c)). An irregularly shaped brown plaque with central ulceration covered by a fibrin pseudomembrane was also observed in the left upper alveolar mucosa (Figure 1 (d)). The patient also exhibited palpable, indurated, and painful bilateral cervical lymph nodes.
With the patient’s consent, an incisional biopsy of the palate was performed. Histopathological analysis revealed a central ulcerated and necrotic area (arrows, Figure 2(a)); cytopathic changes in the superficial epithelial cells, such as hyperchromatism, prominent nucleoli, and necrosis of basal and suprabasal keratinocytes, were also observed (Figure 2(b), yellow head arrows). In addition, ballooning of epithelial cells in the superficial stratum, with vacuolated cytoplasm and a perinuclear halo, suggestive of cytopathic damage, were also found (Figure 2(b), black head arrow, redhead arrows). The presence of lymphocyte exocytosis and Munro’s abscesses were also present (Figure 2(c)). Notably, the typical poxvirus eosinophilic plasma inclusions previously described were absent.
11
The underlying connective tissue exhibited dense collagen fibers and a mild mixed inflammatory infiltrate (Figure 2(d)). Histopathological and ultrastructural features of oral MPVX. (a) Oral epithelium showing acanthosis and an extensive central ulcerated and necrotic area indicating viral infection (arrows) (H&E, x30). (b) Histopathological analysis showing hyperchromatism, prominent nucleoli, and necrosis of basal and suprabasal keratinocytes on the superficial epithelial cells (yellow head arrows). Several epithelial cells in the superficial stratum exhibited balloon cell degeneration of keratinocytes (blackhead arrow) and a vacuolated cytoplasm with a perinuclear halo (redhead arrows) (H&E, x100). (c) Lymphocyte exocytosis and Munro abscesses (H&E, x50). (d) Mild mixed inflammatory infiltrate on the underlying connective tissue, showing dense collagen fibers (H&E, x100). (e)-(f) Electron microscopy revealed intranuclear immature viral MPXV, characterized by ovoid to rounded multilayer particles.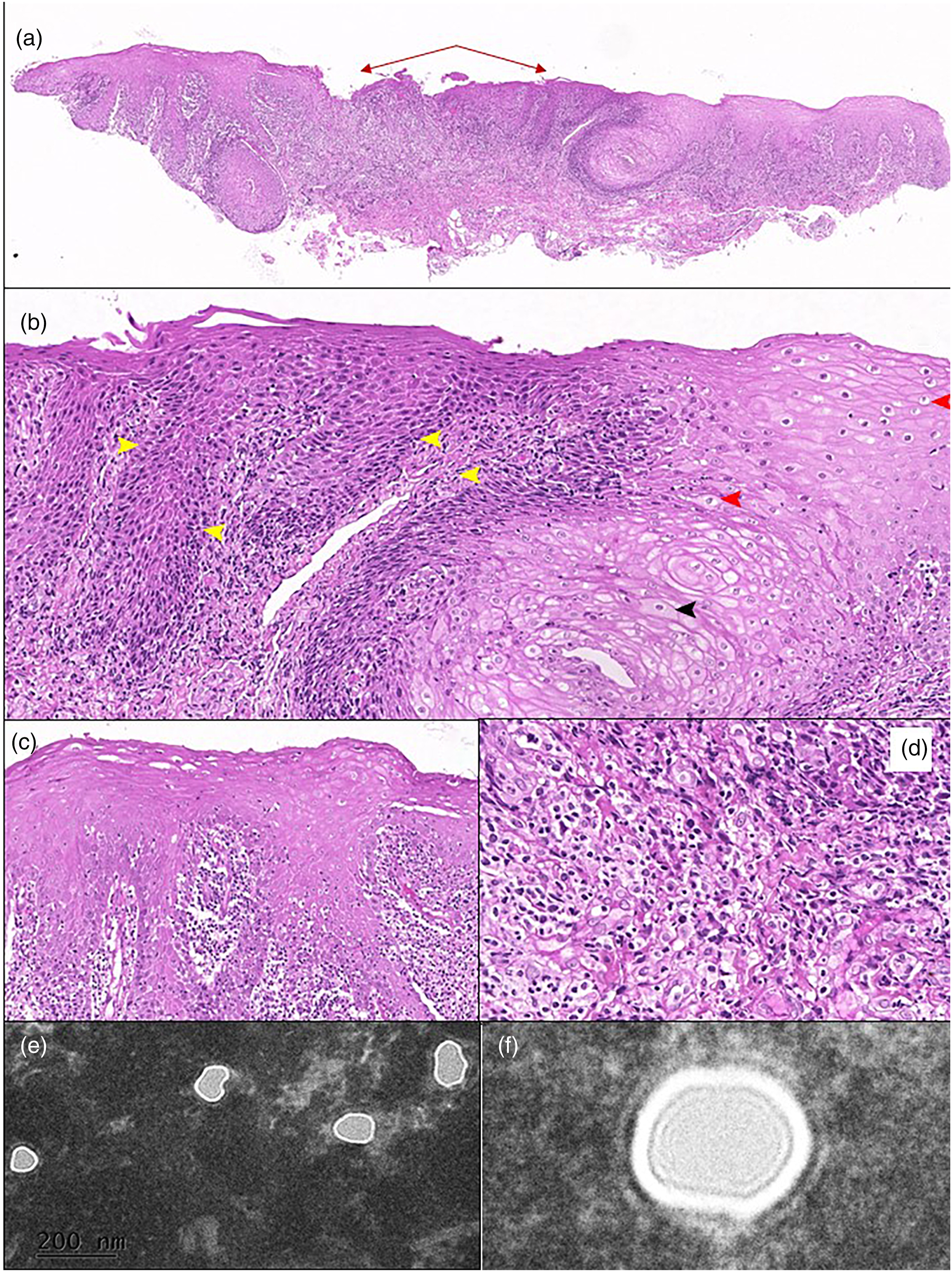
Sections from the paraffin-embedded blocks were dewaxed and then processed following conventional transmission electron microscopy protocol. Ultrastructural findings revealed several intranuclear particles with a medium electron-dense core surrounded by laminar and granular layers (Figure 2 (E–F)), characteristic of immature particles of MPXV.11,12
Simultaneously, the diagnosis of MPXV was confirmed through nucleic acid amplification testing using real-time polymerase chain reaction (RT-PCR), detecting viral DNA sequences in a skin lesion.
Discussion
Mpox is a rare viral disease that belongs to the same family as smallpox and is primarily found in central and West African countries. 2 While it can cause a wide range of symptoms, including skin lesions, MPXV-oral lesions are present in 37%–41% of patients5,13 as papules, vesicles, pustules, and ulcers.3,4 An early MPXV diagnosis helps to limit the infection spreading and to establish appropriate medical and dental treatment. 14
The reported clinical symptoms in this case, such as rash, headache, fever, weakness, fatigue, odynophagia, and lymphadenopathy, presented in our case are consistent with MPXV infection. 13 However, these symptoms can also be seen in other conditions, leading to a differential diagnosis that may include varicella zoster (chickenpox or shingles), herpes simplex infection, secondary syphilis, and impetigo. 15
The most notable histopathological findings, in this case, include early cytopathic changes and the ballooning degeneration of keratinocytes, as described on MPXV skin lesions.11,16 Although no multinucleated keratinocytes or Guarneri bodies were identified, they have been reported in other case series.11,16
The confirmation of the MPXV infection was achieved through RT-PCR from a skin lesion sample, which is considered the gold standard for the diagnosis of MPXV infection. 17 Additionally, electron microscopy analysis provided further insights into the ultrastructural characteristics of MPXV infection, contributing to our understanding of the pathological oral changes induced by MPXV.
This case report highlights the clinical, histopathological, and ultrastructural characteristics of MPXV-oral lesions in a patient with HIV and may provide valuable insights into the features of MPXV infection in the oral mucosa, specifically in people living with HIV. Future studies should focus on unraveling the pathogenesis and exploring potential therapeutic interventions for MPXV-associated oral lesions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.